
Abstract
Introduction:
Metabolic syndrome which is a syndrome complex that is associated with insulin resistance. Osteocalcin (OC), a bone derived protein has been found to decrease insulin resistance and stimulate production of insulin from the pancreas. Serum osteocalcin levels correlate with body mass index (BMI) and waist circumference. Thus, serum osteocalcin levels in metabolic syndrome could potentially be a new area to explore therapeutically. However, its role in clinical practice needs to be established.
Methods:
We conducted a cross-sectional study on patients, who visited Kasturba Hospital, Manipal between September 2018 and September 2020, to study the relationship between Serum Osteocalcin and the parameters of metabolic syndrome. All patients above the age of 18 years who satisfied the NCEP-ATP III guidelines (Asian adaptation) for metabolic syndrome were considered for the study. Patients who had thyroid and parathyroid disorders, bone malignancies, osteoporosis, liver failure and renal dysfunction were excluded.
Results:
A total of 115 subjects were analyzed. As serum osteoclacin increased, there was a significant decrease in fasting blood glucose levels (r = −.748, P < .05) and a significant increase in serum HDL levels (r = .617, P < .01). There was no correlation found between serum osteocalcin and BMI/waist circumference in this study. Finally, it was observed that individuals with fewer components of metabolic syndrome had a significantly higher serum osteocalcin when compared with individuals with a higher number of components of metabolic syndrome (P < .01).
Conclusion:
This data further confirmed the association between serum OC and parameters of metabolic syndrome such as FBS and serum HDL. It also found that increased serum OC was associated with fewer components of the metabolic syndrome indicating that OC could have a positive metabolic impact and may prevent atherosclerotic risk.
Introduction
Metabolic syndrome or Syndrome X is a cluster of conditions that include central obesity, hypertension, dyslipidemia and insulin resistance. This syndrome is also called the insulin resistance syndrome. The past few decades have seen an increase in individuals with metabolic syndrome and these individuals have a higher risk of progression into diabetes or cerebrovascular disease.
Osteocalcin is a bone-derived protein, secreted by osteoblasts which is traditionally used as an index for bone turnover. It undergoes post-translational modifications by gamma carboxylation. It is present in the circulation as both carboxylated and uncarboxylated form. 1
It has been found that osteocalcin influences white adipocytes to increase secretion of adiponectin, which in turn decreases insulin resistance. Osteocalcin also has a role in stimulating beta cells of the pancreas to produce insulin. 2 Studies have also shown that increased serum osteocalcin levels have an association with body mass index (BMI) and waist circumference (WC).
So, serum osteocalcin levels may be targeted in individuals with metabolic syndrome and explored for therapeutic benefit. However, its role in clinical practice needs to be established.
Aims and Objectives
Aim
Relationship Between Serum Osteocalcin and The Parameters of Metabolic Syndrome.
Objectives
Association of serum osteocalcin with BMI and waist circumference in metabolic syndrome.
Association of serum osteocalcin with blood pressure in metabolic syndrome.
Association serum osteocalcin with biochemical parameters of metabolic syndrome (FBS, HDL, Triglycerides).
Methodology
This is a cross-sectional study done on patients who attended the medicine outpatient department and inpatients in the wards in Kasturba Hospital, Manipal in between September 2018 and 2020 and fit into the inclusion criteria of the study.
Inclusion criteria
Individuals above the age of 18.
According to the NCEP-ATP III guidelines using Asian adaptation, the inclusion criteria were defined as meeting 3 or more of the following 5 factors:
Central obesity- waist circumference ⩾ 90 cm in males, ⩾80 cm in females.
Low HDL cholesterol- < 40 mg/dl or under treatment.
High serum triglycerides- ⩾ 150 mg/dl or under treatment.
Increased blood pressure- ⩾ 135/80 or under treatment.
Fasting plasma glucose ⩾ 100 mg/dl or under treatment.
Exclusion criteria
Patients with hyperparathyroidism, hypoparathyroidism, thyroid disorders, osteoporosis, rheumatoid arthritis, Cushing disease, bone related malignancies, liver diseases, renal failure, pancreatic gland dysfunction were excluded. Patients on oral contraceptives, hormone replacement therapy, steroid therapy, vitamin k, vitamin D, calcium, anti-epileptic drugs, calcitonin, bisphosphonates, denosumab or anabolic agents like teriparatide and insulin therapy were also excluded.
Patients were asked questions based on a standard proforma regarding co-morbidities pertaining to metabolic syndrome. They underwent anthropometric measurements, including height using a stadiometer, weight using an electronic balance. BMI was calculated as weight (kilograms) divided by height squared (square meters). A detailed general, physical and systemic evaluation was also carried out, including measurement of blood pressure using a sphygmomanometer. Blood pressure was recorded every 3 minutes, and an average of 3 readings was taken along with systemic examination. Waist circumference was calculated as the abdominal circumference at the midpoint between the coastal margin and anterior superior iliac spine. Blood samples were drawn for assessment of fasting plasma glucose, fasting lipid profile, osteocalcin, liver function tests, renal function tests.
Methods of Sample Collection and Analysis
Blood sample collection and analysis
Blood sample was collected by venipuncture from peripheral veins under aseptic precautions.
The first sample was collected after an overnight 8 to 10 hours of fasting in the morning for measurement of fasting plasma glucose, osteocalcin, HbA1C, fasting lipid profile, renal & liver function tests. Analysis of osteocalcin and insulin was done in the serum.
Serum was separated after blood had clotted using a centrifuge. This was done at room temperature and stored in −200°C immediately and −700°C for long-term storage before analysis of osteocalcin and fasting insulin.
Osteocalcin ELISA methodology
Immunoenzymetric assay for the in vitro quantitative measurement of intact human osteocalcin in serum.
Principles of the method: OC ELISA is a solid phase enzyme amplified sensitivity immunoassay. Monoclonal antibodies which are directed against specific epitopes of human OC were used. Bound enzyme-labeled antibody was measured through a chromogenic reaction. A calibration curve was plotted, and the OC was determined by interpolation from this calibration curve.
Statistical analysis
The analysis was done using SPSS software version 23.0. Mean with standard deviation was used for normally distributed data. Median with interquartile range was used for skewed data. Categorical data were expressed as a percentage. Mann-Whitney U and Kruskal Wallis test was used when serum OC levels were compared between groups. Continuous variables which were normally distributed were correlated using Pearson’s correlation. Continuous variables which were not normally distributed were correlated using Spearman rank correlation. A P value <.05 was considered statistically significant.
Results
This study has been done to establish a relationship between serum OC and insulin resistance in patients with metabolic syndrome. The various parameters of metabolic syndrome, namely fasting blood glucose, hypertension, high-density lipoprotein, triglycerides, and waist circumference, were also correlated with serum Osteocalcin levels.
A total of 115 subjects were evaluated, N = 115. The mean age of the subjects in the study was 54.7 ± 11.2 years. There were 55 males (47.9%) and 60 females (52.1%) in the study.
The baseline anthropometric measurements of the patients are detailed in Table 1.
Anthropometric measurements of the participants.

Out of the 55 male subjects, 48 males had an abnormal waist circumference (>90 cm).
Out of the 60 female subjects, only one female had a waist circumference (>80 cm).
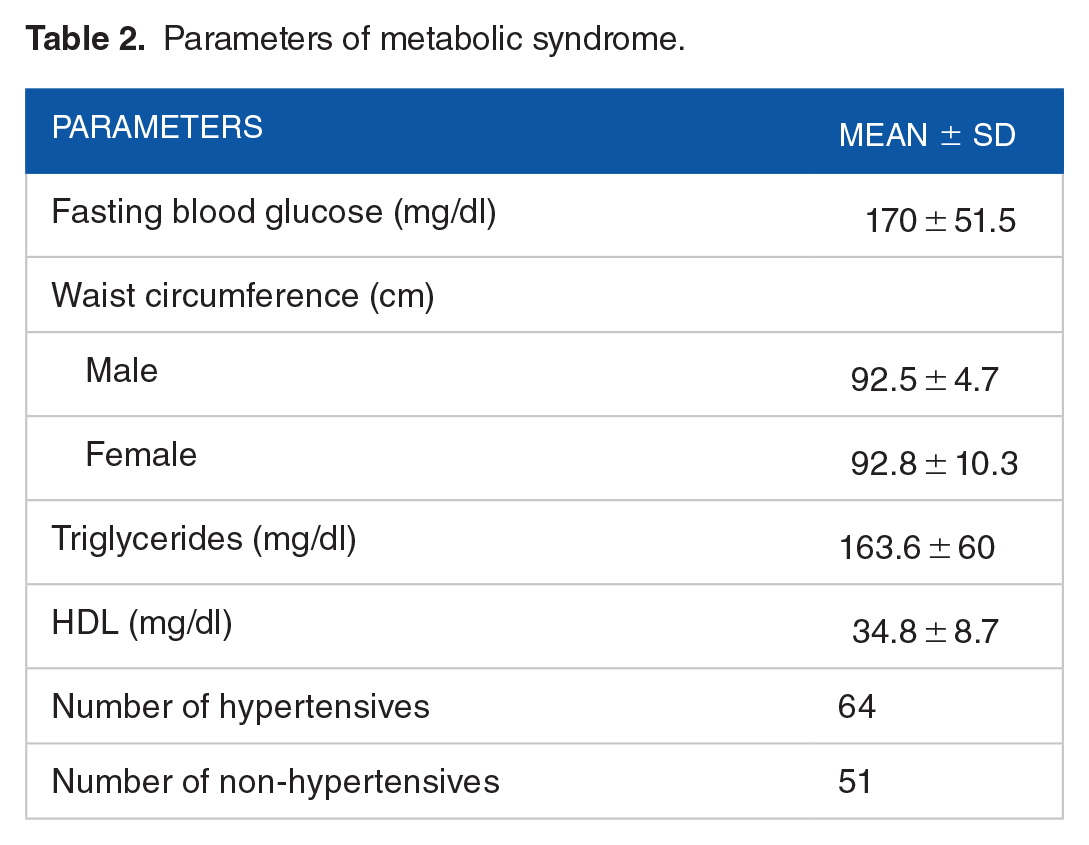
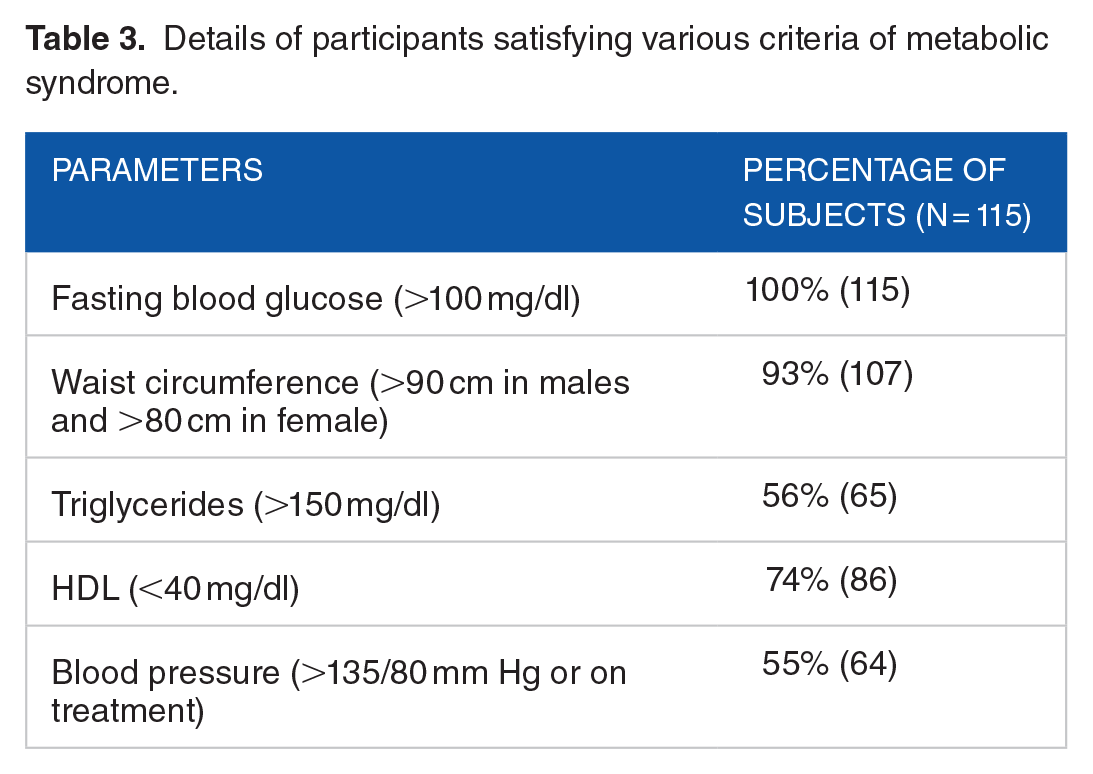
The baseline values of the parameters of metabolic syndrome are shown in Table 2. The details of the participants satisfying various criteria of metabolic syndrome are mentioned in Table 3 and Figure 1.
Parameters of metabolic syndrome.
Details of participants satisfying various criteria of metabolic syndrome.

Representation of baseline parameters of metabolic syndrome.
All patients included in our study were diabetics. A major percentage of patients with metabolic syndrome taken in this study had diabetes and abnormal waist circumference.
Correlation between serum OC and anthropometric measurements
OC and BMI
As seen earlier, the mean BMI in both males and females in this study was in the obese range. The association between Serum osteocalcin and BMI is shown in the Figure 2.

Scatter plot showing the correlation between serum osteocalcin and BMI.
Serum osteocalcin levels which were correlated with BMI of the study subjects showed that BMI decreased with increased serum osteocalcin. Though there was a trend, this correlation was nofind and t found to be statistically significant. (r = −.057, P = .54).
OC and waist circumference
Waist circumference cut-off was taken as 80 cm in females and 90 cm in males. Mean waist circumference in both males and females was higher than the normal cutoff indicating that many of the study subjects were obese.
Serum OC was correlated with waist circumference in males and females individually. This is represented in Figures 3 and 4. No significant correlation was found between serum OC and waist circumference in both males and females in this study (r = .063, P = .62 in males and r = .045, P = .73 in females).

Scatterplot showing the correlation of serum osteocalcin with waist circumference in females.
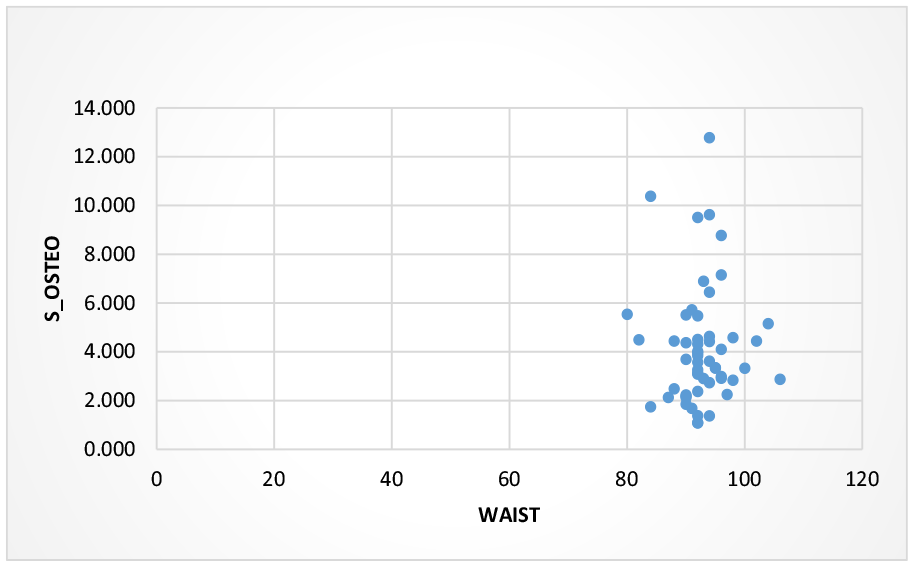
Scatterplot showing the correlation of serum osteocalcin and waist circumference in males.
Correlation between serum OC and blood pressure
Sixty-four hypertensives and 51 non-hypertensives were present in the study. Table 4 shows the median OC levels among the hypertensive and the non-hypertensive patients in the study population. The median OC was found to be higher in hypertensives when compared to hypertensives. However, this correlation was found to be statistically insignificant (P = .427).
Number of hypertensives with median osteocalcin values.

Correlation of serum OC and biochemical parameters of metabolic syndrome
OC and fasting blood glucose
Fasting blood sample was used to measure fasting blood glucose in the 115 subjects, and the FBS was correlated with the OC levels and shown in Figure 5. A significant decrease in fasting blood sugar with an increase in serum OC was observed. (r = −.748, P < .05).

Scatter plot showing the correlation of fasting blood glucose with serum osteocalcin.
Correlation of serum OC with HDL and triglycerides
One hundred fifteen subjects with metabolic syndrome were taken for this study. HDL and triglycerides contribute to 2 out of the 5 components in metabolic syndrome. The correlation of OC with HDL and TG has been depicted in Figures 6 and 7 respectively. As serum OC increased there was a significant increase in HDL levels (r = .617, P < .01). As serum OC increased, a decrease was observed in serum triglycerides, but this correlation was not found to be statistically significant (r = −.110, P = .24).

Scatter plot of the correlation of osteocalcin and HDL.

Scatterplot showing correlation between serum osteocalcin and triglycerides.
Correlation of serum OC with a number of components of metabolic syndrome
A correlation was established between the serum OC levels with the number of components of metabolic syndrome to see if there was a decrease in serum OC with a rise in number of components of the metabolic syndrome. Figure 8 shows the correlation between OC and the components of metabolic syndrome.

Boxplot showing the correlation between serum osteocalcin and components of metabolic syndrome.
Discussion
OC, which was previously considered to have limited use, has recently been considered a pathophysiological link in insulin resistance, insulin secretion and glucose metabolism. 1 Initial studies done on animal-based models proved helpful in finding a connection between glucose metabolism and the levels of serum OC. 2 Initial studies on humans also showed similar results. 3 OC and its association with conditions including hyperglycemia, dyslipidemia and central obesity has been noted and its strong association with insulin resistance also has been reported. 4 In view of this association between serum osteocalcin and glucose metabolism as well as insulin resistance, many studies were done to look for a relationship between the levels of this bone-derived protein and its effect on glucose homeostasis. 5 This study was conducted to establish an extension of this correlation of OC in patients who were diagnosed with metabolic syndrome.
Serum OC with BMI
Obesity has been associated with increased circulating levels of leptin and a decrease in adiponectin which contribute to the presence of higher levels of insulin resistance in these individuals.6,7 Though there has been heterogenicity in the findings of various studies depicting the relationship between serum OC and BMI, a majority of them showed a negative correlation between the two.
An Egyptian study conducted by El-Eshmawy and Abdel Aal on a total of 100 obese-overweight individuals showed a negative correlation between serum OC and body mass index (r = .21, P = .03) in 50 obese as well as 50 overweight individuals. 8 This was consistent with findings from another study conducted by Caglar et al in non-diabetic post-menopausal women, where serum OC was significantly lower in women who were found to be obese (BMI > 30 Kg/m2) (P = .03). 9
Though many studies showed a similar result, a study by Fernandez et al on 45 south Indian women showed no significant relationship between serum OC and BMI in those individuals. 10 Another Indian study by Singh et al also showed a similar result. 11
In our study, though the levels of serum OC were lower in subjects with a higher BMI in the present study, the correlation was found to be statistically insignificant. This concordance in findings compared to the other international studies could be due to population research design, sampling parameters, and methodology differences in these studies.
Serum OC and waist circumference
Central obesity is one of the components in metabolic syndrome. An increased waist circumference is associated with a higher degree of insulin resistance. 12
In a large population-based study by Yeap et al in 4263 men, a significant inverse relationship was established between serum OC and waist circumference (P < .001). 13 They also hypothesized that OC may lie in the causal pathway between central adiposity and insulin resistance.
Another study conducted by Bador et al with 90 subjects showed no significant correlation between serum OC and waist circumference. 14 This discrepancy could be attributed to the smaller sample size in this study. Even in our study, no correlation was established between serum OC and waist circumference.
Serum OC and blood pressure
A lot of varied results were observed when it comes to a correlation of serum OC with blood pressure.
A large Chinese study by Xu et al consisting of 2241 individuals showed that male hypertensives had lower serum OC than the normotensive males (P = .039). An inverse relationship was also observed between serum OC and systolic blood pressure in men (P = .004). But there was no association found between serum OC and blood pressure in females. 15 Sanchez-Enriquez et al studied 140 hypertensives (70 diabetics and 70 non-diabetics) and found that there was increased serum OC in the diabetics with high diastolic blood pressure. There was no correlation found between serum OC and systolic blood pressure. 16 Our study also showed no association was found between serum OC and blood pressure (both systolic and diastolic). This could be due to the continued use of anti-hypertensive drugs which could have normalized the blood pressure in these individuals and hence been a confounding factor in the results.
Serum OC and fasting blood sugar
Serum OC is also known to promote beta cell function, thereby promoting insulin secretion, which leads to better glycemic control. A study conducted by Hussein evaluated 40 individuals (20 diabetics and 20 non-diabetics). The diabetic patients had significantly lower serum OC (P <= .001) and lower serum OC was also specifically associated with higher fasting blood glucose (P = .07). 17 A case-control study on elderly subjects from Sweden by Kindblom et al showed that serum OC was inversely related to fasting plasma glucose (P < .001) in both diabetic and non-diabetic subjects. 18
A study by Sarkar and Choudhury showed that in 56 Indian subjects, serum OC in patients with controlled blood sugar was higher than when compared to subjects with uncontrolled fasting blood sugar after adjusting for age and BMI (P < .05). 19
Consistent with both Indian and international studies, our study also showed a significant decrease in fasting blood glucose levels with an increase in serum OC levels in diabetics as well as patients with metabolic syndrome (r = −.748, P < .05). This pointed toward the protective role of serum OC toward blood sugar levels.
This association is explained by Wang et al who suggested that elevated glucose levels significantly affect osteoblastic cell growth, thereby suppressing the expression of OC. 20 Hyperglycemia could also be toxic to osteoblasts, thereby impeding the production of OC as explained by Hamada et al . 21 Therefore, it can be concurred that OC is a part of the feedback loop, regulating the glucose metabolism by its effect on insulin secretion as well as peripheral insulin resistance. However, the exact mechanisms that orchestrate the OC effect on blood glucose and insulin sensitivity are yet to be elucidated.
Serum OC and fasting lipid profile
There is a well-documented effect of serum OC on lipid metabolism. OC is known to influence white adipocytes to increase secretion of adiponectin.
A large study conducted by Saleem et al showed that 2493 patients (bio-ethnic cohort) with higher levels of serum OC were found to have significantly lower triglyceride levels (r = −.19, P < .05). They were also found to have a higher level of HDL(r = .03), but this relation was not found to be statistically significant. 3
A smaller study conducted Riquelme-Gallego et al in 235 individuals showed a significant increase in HDL in patients with raised serum OC (r = .281, P < .001) while there was no correlation found between serum OC and triglycerides. 22
Coming to the Indian data, a study conducted by Almas and Vanitha on 90 subjects (45 with metabolic syndrome and 45 without) showed that as serum OC increased, a significant increase was noted in HDL (r = .964, P < .001) and a significant decrease in triglycerides (r = −.684, P < .001). 23
The results of our study concurred with the available literature, which showed an increased HDL (r = .617, P < .05) and a decrease in triglycerides (r = −.110, P = .24) in patients with raised serum OC. Serum OC and adiponectin levels alters insulin resistance by potentiating the fatty acid metabolism in the muscles, inhibiting gluconeogenesis, decreasing triglyceride levels and plasma fatty acid levels. 24 OC exercises its effect on the adipocytes via adiponectin. This suggests that OC can be explored to improve lipid profile in diabetics with metabolic syndrome owing to its dual effect on both the glycemic and lipid parameters.
Serum OC and components of metabolic syndrome
In a study of 181 Chinese men by Bao et al, it was found that serum OC was significantly lower in patients as the number of components of metabolic syndrome increased. (P < .01). Significant lower serum OC concentrations were found in subjects with 3, 4 and 5 components [16·93 (12·00-24·11) ng/ml, 15·36 (12·81-18·01) ng/ml and 14·74 (10·78-18·64) ng/ml, respectively] . 25 In their study in postmenopausal women, Dumitru et al, also concluded that low serum osteocalcin was a risk factor for metabolic syndrome and was independent of the presence of diabetes. 26 Similarly, in our study, individuals with fewer components of metabolic syndrome were found to have a significantly higher serum OC when compared to individuals with more components of metabolic syndrome. This association of OC with the metabolic syndrome supports the reciprocal regulation of bone on energy metabolism, implicating that OC might be a novel target for the treatment of metabolic and cardiovascular disorders in the future.
Another randomized clinical trial in Germany done on patients with Metabolic syndrome with lifestyle-induced weight loss, showed that OC was independently associated with C-reactive protein thereby indicating that weight loss triggered high OC levels were associated with decreased inflammation. This indicates that OC could have potential roles far beyond metabolic components or BMI. 27 In a Turkish study on post- menopausal women, it was found that OC levels were lower in the group with metabolic syndrome. Further, there was a negative correlation noted with OC and metabolic parameters like fasting blood glucose, body weight, and BMI. Therefore, OC has been noted to display a close association between glucose and lipid metabolism. 28
Strengths and limitations
The strength of this study is that it attempts to analyze OC which is a relatively newer and lesser understood hormone in the interplay of metabolic syndrome. This study has also attempted to understand the interaction between OC and anthropometric, glycemic and lipid parameters. However, this study was limited in its sample size and as this was a cross-sectional study, we were not able to follow-up the study participants long term. as this study was limited by its number, the strength of the study is limited to its novelty and a follow-up study with a larger sample size is required to demonstrate the benefits of the results obtained herer. We also did not assess HOMA-IR, which could have been a useful indicator of insulin resistance in this study. Though OC exists in both carboxylated and uncarboxylated forms, our study did not measure them separately but measured only the total OC levels in our patients.
Conclusion
As serum OC increased, there was a significant decrease in fasting blood glucose levels and increase in HDL levels which showed a protective metabolic role for OC. This translated into higher OC levels having fewer components of metabolic syndrome. These conclusions supported the recent concept that OC has an endocrine function, as the bone has close interactions with energy metabolism that could dictate the onset and severity of metabolic syndrome and may be a therapeutic target in the future.