
Abstract
Aim:
The aim of this study was to test the hypothesis that body mass index (BMI) and waist circumference (WC) associate to a comparable degree with insulin resistance and cardiometabolic risk factors in South Asians.
Methods:
We measured blood pressure and fasting glucose, insulin, triglyceride, high-density lipoprotein cholesterol (HDL-C), high-sensitivity C-reactive protein (hs-CRP), and fibrinogen and calculated the homeostasis model assessment of insulin resistance (HOMA-IR) in a community-based sample of 923 nondiabetic South Asians.
Results:
BMI and WC were highly correlated in both genders (r = 0.82 and 0.87). The relationship between BMI and values of blood pressure, glucose, insulin, HOMA-IR, triglyceride, HDL-C, hs-CRP, and fibrinogen was comparable to that between WC and these variables. Fasting insulin and HOMA-IR correlated most strongly with BMI (r = 0.49 to 0.56) and WC (r = 0.52 to 0.59).
Conclusion:
These results show that BMI and WC associate to a comparable degree with estimates of insulin resistance and related metabolic abnormalities in South Asians.
Introduction
The notion that differences in abdominal obesity, as determined by waist circumference (WC), is the index of excess adiposity that best predicts the presence of insulin resistance and associated metabolic abnormalities has received considerable support over the years.1–3 More recently, in a publication 4 presenting ‘a single global definition’ of the metabolic syndrome, it was concluded that ‘insulin resistance continues to explain most if not all of the metabolic syndrome’ and that ‘the metabolic syndrome all begins with central adiposity.’ This view of the fundamental importance of abdominal obesity might be of particular relevance to South Asians, who have an increased prevalence of insulin resistance, hyperinsulinemia, and high triglyceride (TG) and low high-density lipoprotein cholesterol (HDL-C) concentrations,5–7 and in whom it has been suggested that abdominal obesity accounts for these metabolic abnormalities and increased risk of cardiovascular disease.8–10 We have addressed this issue in a recent publication 11 demonstrating that insulin resistance in South Asian women was significantly associated with a higher plasma TG and lower HDL-C concentrations, independent of differences in abdominal obesity as estimated by waist circumference (WC). The current study extends these earlier observations of the relationship between WC, insulin resistance, and dyslipidemia to a much larger group of South Asians. In particular, we wished to test the hypothesis that the association between body mass index (BMI), an index of overall obesity, and estimates of insulin resistance and cardiometabolic risk factors was comparable to that seen with WC, an index of abdominal obesity, in a population of apparently healthy South Asian women and men.
Methods
Study subjects
Our study sample consisted of 414 women and 509 men, part of a larger group of individuals (n = 4797), who had volunteered to be screened for cardiovascular disease risk factors at the South Asian Heart Center, a not-for-profit organization in Mountain View, California, that provides cardiovascular disease risk assessment and counseling to South Asians in the San Francisco Bay Area. The Institutional Review Board of El Camino Hospital, Mountain View, California, approved the study. The study participants were in general good health and older than 18 years. We excluded individuals who were taking glucose or lipid lowering medications, were not fasting for longer than 10 h, and had fasting glucose concentration ≥ 7.0 mmol/l. We did not perform oral glucose tolerance tests (OGTT), so our study sample included subjects who might have met criteria for a diagnosis of type 2 diabetes or impaired glucose tolerance (IGT) on the basis of the OGTT.
Anthropometric measurements
We performed the medical interview and physical examination at the South Asian Heart Center. We measured height and weight with subjects in light clothing and without shoes and calculated BMI by dividing weight (in kilograms) by height (in meters squared). We recorded WC according to the National Health and Nutrition Examination Survey III protocol during normal minimal respiration by placing a measuring tape around the waist just above the uppermost lateral border of the iliac crest. 12 We measured blood pressure and heart rate with an automatic blood pressure recorder (Dinamap XL vital signs monitor) using an appropriately sized cuff. During the measurements, subjects sat in a chair with feet on the floor and arm supported at heart level.
Laboratory measurements
After an overnight fast, we drew blood samples for the measurement of plasma glucose, insulin, TG, and HDL-C, high-sensitivity C-reactive protein (hs-CRP), and fibrinogen concentrations. The Berkeley HeartLab performed the laboratory analyses. 13 Specifically, glucose concentrations were measured by enzymatic rate reaction; insulin by electrochemiluminescence immunoassay; TG by blanked enzymatic method; HDL-C by a homogeneous direct assay; hs-CRP by particle-enhanced immunoturbidimetric assay; and fibrinogen (mass) by immunoturbidimetric assay. The insulin assay had 100% cross-reactivity with human insulin and 5% with human pro-insulin. The total and within-run precisions (%) of the laboratory assays were as follows: glucose (2.03, 0.82); insulin (2.67, 1.35); TG (2.43, 0.90); HDL-C (3.25, 0.98); hs-CRP (1.96, 0.52); and fibrinogen (2.88, 0.97).
Statistical analysis
We employed statistical software R version 2.10.1 (The R Foundation for Statistical Computing) to perform statistical analyses. We present summary statistics as mean ± SD. We calculated the homeostasis model assessment of insulin resistance (HOMA-IR) from fasting glucose and insulin concentrations using the formula: ([fasting insulin (microunits per milliliter)]*[fasting glucose (mmol per liter)])/22.5. 14 We log transformed values of insulin, HOMA-IR, TG, HDL-C, and hs-CRP and calculated Pearson correlation coefficients (with 95% confidence intervals) among variables of interest.
Results
The demographic and metabolic characteristics of the 923 South Asians are shown in Table 1. These data indicate that WC was greater in men, whereas values for BMI were comparable in the two genders. Men had higher blood pressure and TG and lower HDL-C, hs-CRP, and fibrinogen concentrations, but the values for the other metabolic variables seemed reasonably comparable in the two groups.
Demographic and metabolic characteristics of the 923 study participants.
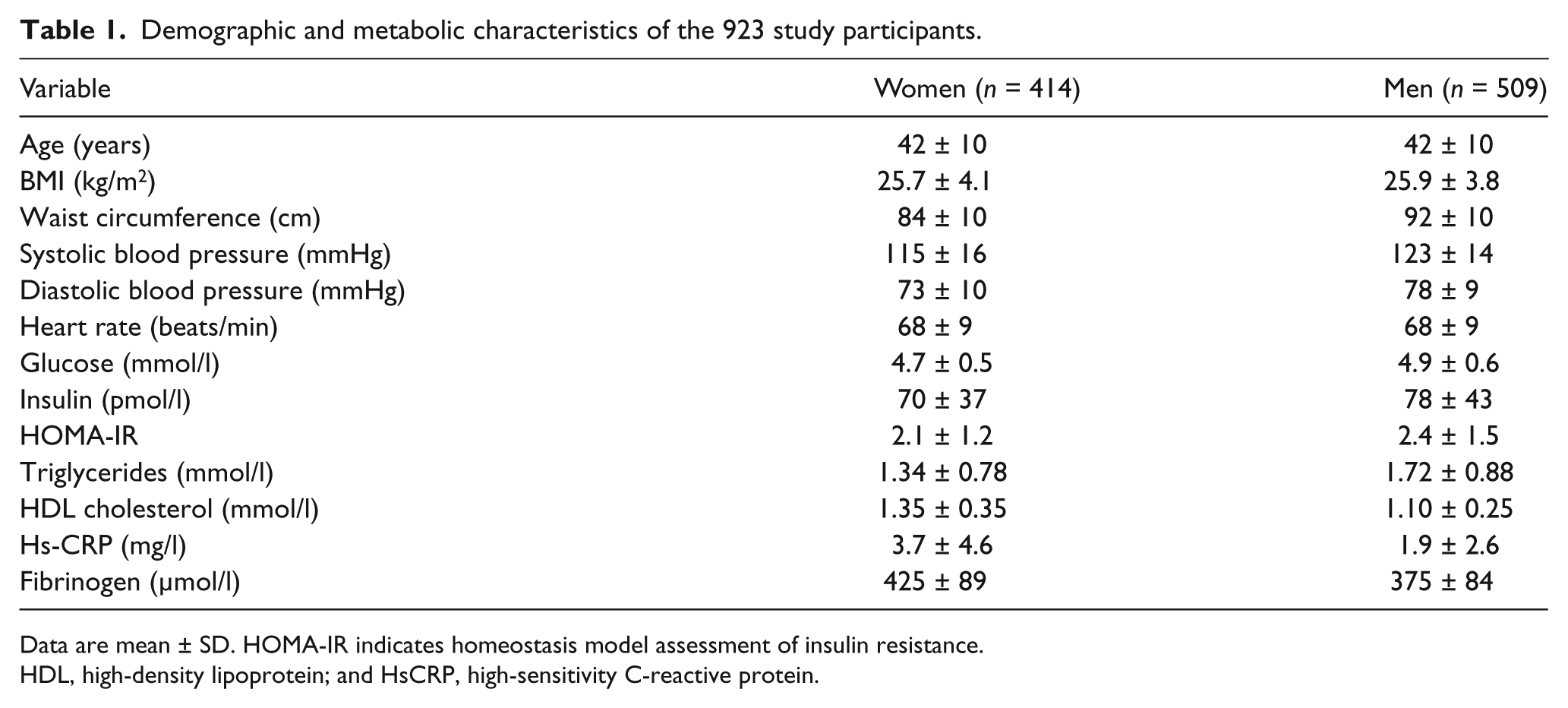
Data are mean ± SD. HOMA-IR indicates homeostasis model assessment of insulin resistance. HDL, high-density lipoprotein; and HsCRP, high-sensitivity C-reactive protein.
Body mass index and WC were highly correlated (p < 0.001), with r-values of 0.82 (0.79–0.86) and 0.87 (0.84–0.89) in women and men, respectively.
Correlation coefficients (r-values) among the two indices of adiposity and the individual metabolic variables are shown in Table 2. Although the actual r-values differed considerably as a function of metabolic variable, certain generalizations seemed to emerge. Firstly, r-values between individual metabolic variable and the two indices of adiposity were reasonably comparable in both women and men. Secondly, the magnitude of the relationship between BMI and WC and each metabolic variable was highest with insulin concentration and HOMA-IR and lowest with glucose concentration, and this was true in both women and men. However, there did appear to be a few gender differences in that the strengths of the relationship of BMI and WC with TG and HDL-C concentrations were somewhat greater in women than in men, whereas the correlations of BMI and WC with fibrinogen concentrations were somewhat stronger in men than in women.
Relationship of body mass index and waist circumference with cardiometabolic risk factors in South Asian women and men.
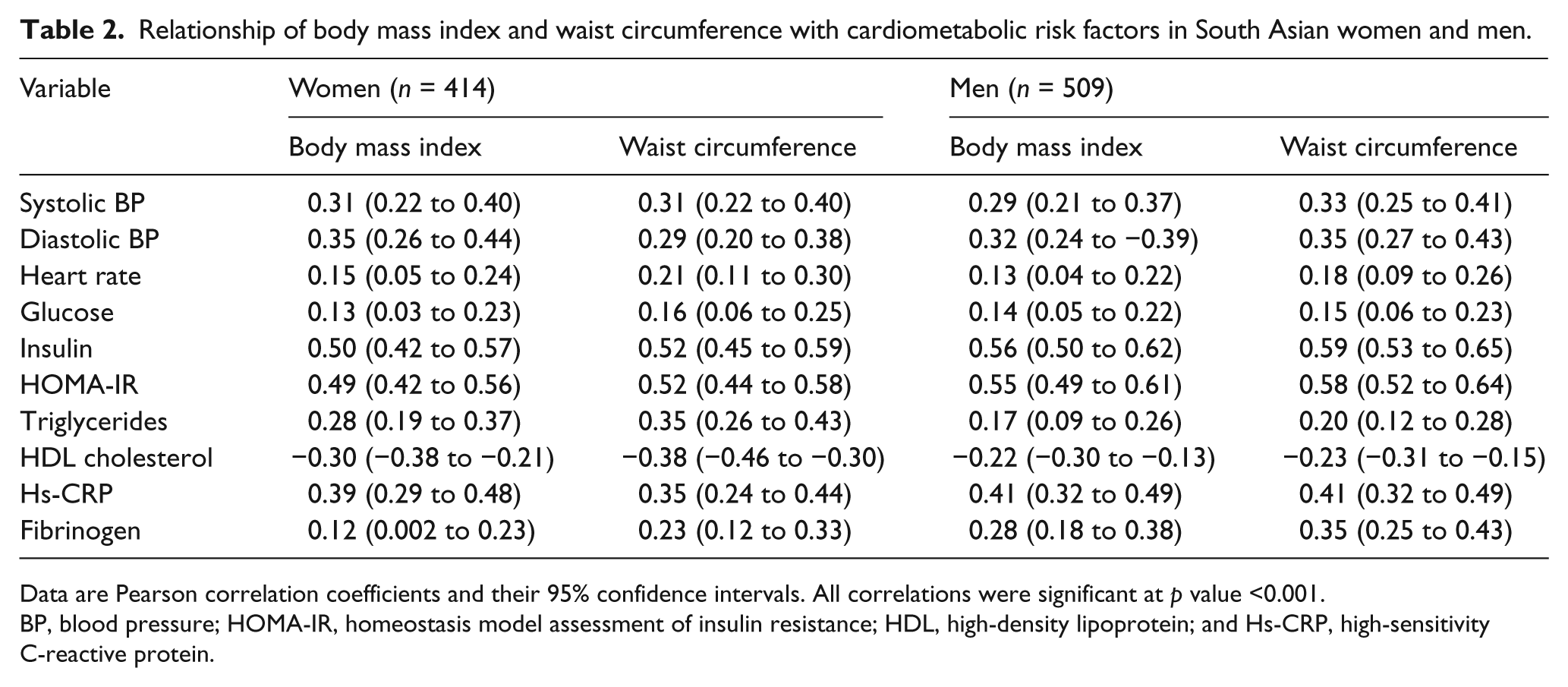
Data are Pearson correlation coefficients and their 95% confidence intervals. All correlations were significant at p value <0.001. BP, blood pressure; HOMA-IR, homeostasis model assessment of insulin resistance; HDL, high-density lipoprotein; and Hs-CRP, high-sensitivity C-reactive protein.
Discussion
The results presented demonstrate that the relationship between BMI and both insulin resistance and cardiometabolic risk factors is almost identical to that between WC and these variables. As such, these findings support our hypothesis that BMI and WC associate to a comparable degree with insulin resistance and related metabolic variables in South Asian women and men. Furthermore, differences in BMI or WC were most closely related to differences in estimates of insulin resistance, whether fasting plasma insulin or HOMA-IR was used as the surrogate estimate of insulin resistance.
Our demonstration that measurements of BMI and WC are comparable in their association with estimates of insulin resistance and related cardiometabolic risk factors in South Asians is of particular interest in light of the recent analysis by The Emerging Risk Factors Collaboration of data from 58 prospective cohort studies (221,934 people) in which the authors showed that BMI, WC, and waist-to-hip ratio were comparable in their ability to predict incident cardiovascular disease. 15 They also concluded that knowledge of these indices of adiposity did not improve cardiovascular disease risk prediction when information was available concerning history of diabetes, systolic blood pressure, or lipid measurements. Because the analyses of The Emerging Risk Factors Collaboration are based on populations in western Europe or the United States, 16 our findings in South Asians, a group in which abdominal obesity has been considered to play a central role in the development of insulin resistance, dyslipidemia and cardiovascular disease, complement their conclusions that BMI and WC provide essentially identical information concerning cardiovascular disease risk.
Turning now to the magnitude of the relationships between BMI and WC and the metabolic risk factors, the weakest correlation was between increases in values of each adiposity measure and fasting plasma glucose concentration. This finding should not be surprising because patients with type 2 diabetes were excluded from the analysis and the mean plasma glucose concentrations in both women (4.7 mmol/l) and men (4.9 mmol/l) were <5.0 mmol/l. Indeed, these findings are quite similar to a previous report showing in 208 nondiabetic individuals, with a mean fasting plasma glucose of 4.8 mmol/l, who were primarily of European ancestry (~75 %), that the correlation coefficient (r-value) between fasting plasma glucose concentration and insulin-mediated glucose disposal was 0.20. 17
The strength of the relationship between adiposity index and lipid measurements in South Asians was intermediate to that between estimates of insulin resistance and glucose concentration, and there appeared to be a gender difference in this instance. Specifically, in women, r-values were approximately 1.6-fold higher for the relationship of either BMI or WC with TG or HDL-C concentrations. However, even in this situation, the magnitude of the difference was modest. For example, in the case of TG concentration, the relationship between BMI and TG concentration could account for ~8% of the variance in TG concentration, whereas 12% of the variance was explained when WC was the index of adiposity. Similarly, in the case of HDL-C, ~9% and ~14% of the variability could be accounted for by differences in BMI and WC, respectively.
Our study has certain weaknesses. To begin with, it is cross-sectional in nature. In addition, surrogate estimates of insulin resistance were used. However, both fasting plasma insulin concentration (r = 0.69) and HOMA-IR (r = 0.62) have been shown to be significantly related (p < 0.001) to a direct measure of insulin-mediated glucose disposal.18,19 Finally, we did not quantify visceral fat content, and it has been argued that an excess of visceral fat is the crucial determinant of insulin resistance, dyslipidemia, and cardiovascular disease risk in South Asians.8–10 Thus, any conclusions to be drawn from the present study are only applicable to anthropometric assessments of excess adiposity and do not address the magnitude of the relationship between direct measures of visceral fat, as assessed by computerized tomography, and CVD risk factors. On the other hand, clinical estimates of regional fat distribution are almost universally based on anthropometric measurements; and, for purposes of clinical evaluation, our data suggest that BMI performs as well as WC as a correlate of insulin resistance and associated metabolic abnormities. Furthermore, results of a study 3 in which anthropometric values were compared to regional fat areas quantified by computer tomography have shown that visceral fat area is correlated to a comparable degree with BMI and WC in both women (0.84 vs. 0.87) and men (0.74 vs. 0.77).
The greatest strength of our findings is in the relatively large number of apparently healthy South Asian women (n = 414) and men (n = 509) studied. Our results indicate that although the magnitude of the relationship between either BMI or WC and individual metabolic variables varies substantially, there is relatively little variability between the association of any given metabolic variable with BMI or WC in South Asians. Finally, these conclusions should not be too surprising given the evidence of how closely BMI and WC are related to each other.
Conclusion
Measurements of BMI and WC were highly correlated in the 923 apparently healthy South Asians in this study, and the two indices were related to a comparable degree to both insulin resistance and associated cardiovascular disease risk factors. These data do not support the view 4 that, at least in South Asians, ‘the metabolic syndrome all begins with central adiposity’.
Footnotes
Acknowledgements
We thank El Camino Hospital and the Community Benefit Council of El Camino Hospital District for their generous support. We also extend our thanks to the study participants who volunteered for our study.
Funding
The South Asian Heart Center is funded by the Community Benefit Council of El Camino Hospital District and El Camino Hospital, 2480 Grant Road, Mountain View, CA 94040-4333, USA. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that they have no competing interests. The funding source played no role in the study design; collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.