
Abstract
Background:
Diabetic foot ulcers (DFUs) are debilitating to the patient and costly for the healthcare system. We set up the Diabetic Rapid Evaluation and lower limb Amputation Management (DREAM) clinic with the aim of providing early directed specialist care to patients with DFUs. With early management, we hope to treat DFUs in its early stages, reducing the need for and associated morbidity of major and minor lower limb amputations.
Objectives:
We evaluated the outcomes of the fast-access DREAM clinic with multi-disciplinary evaluation for patients with DFUs. Outcomes include time from the point of referral to DREAM clinic evaluation, amputation rates and wound healing rates.
Design;
Patients presenting with DFU to the DREAM clinic were enrolled. A podiatrist made the first assessment, followed by immediate specialist consultation with Endocrinologists, Vascular surgeons or Orthopaedic surgeons as required.
Methods:
Data on baseline demographics and DFU characteristics were collected. Outcomes evaluated were wound healing at 12 weeks, wound salvage rates, time to DREAM clinic access and time to specialist referral.
Results:
Sixty-eight patients were enrolled, with 57.3% males, and mean age of 63 ± 13.0 years. Majority of ulcers were classified as neuropathic (41.3%) and located at the digits (40%). At 12-weeks follow-up, 1 had undergone major amputation, 9 minor amputations and 4 surgical debridements. The median time to DREAM clinic evaluation from first presentation was 3 days (IQR 7). Eleven (16.2%) required >1 specialist consult. Twenty (29.4%) were hospitalised for treatment. Twelve underwent revascularisation within 4 days (IQR 3.5). Twenty-four patients (35.3%) continued podiatry follow-up, having 28 DFUs in which 20 (71.4%) healed within 12 weeks.
Conclusion:
The fast-access multidisciplinary DREAM clinic shows promising outcomes with lower major amputation rates and exemplary DFU healing outcomes.
Introduction
Diabetes mellitus (DM) has an estimated prevalence of 537 million in 2021 and is projected to increase further to 784 million in 2045. 1 Diabetic foot complications are one of the many sequelae of diabetes.
Diabetic foot complications are characterised by the presentation of ulceration on the foot, and is often associated with neuropathy, and peripheral arterial disease (Figure 1). A poorly managed DFU may lead to lower limb amputation when the foot becomes non-functional and severely infected.

Algorithm for determining aetiology of wound (with permission from Yazdanpanah et al 2 ).
In terms of prevalence, DFUs affect 25% of people with diabetes in their lifetime, 3 with the United Kingdom reporting an annual incidence of 2.2% in 2002. 3 In Singapore, where DM prevalence has increased from 8.2% in 2004 to 11.3% in 2010 4 and is projected to increase further to 15% in 2050, 5 it is estimated that 20% of people with diabetes will develop a DFU in their lifetime. 6
DFUs affect the quality of life7,8 with high morbidity and mortality. 9 Patients with DFUs have a 2.5-fold increased 5-year mortality rate when compared to the general population. 10 There is a high prevalence of anxiety and depression, 11 due to limitations to the activities of daily living, 12 which in turn is associated with impaired healing and an increased risk of recurrent ulcers.13,14 Poor healing of DFU may lead to infection with approximately 84% eventually needing amputation. 3 The 1-year mortality for patients who underwent amputation ranges from 11.3% to 50.2%,15 -18 whilst 5-year mortality stands at more than 70%. 3 In Singapore, the minor and major lower limb amputation rate has increased from 21.8 per 100 000 in 2008 to 27.2 per 100 000 in 2013. 19 Singapore also has one of the highest rates of lower limb amputations globally. 6 Data from Singapore’s largest tertiary hospital suggests that 3.2% of patients with diabetes will undergo a lower limb amputation in their lifetime. 20
DFUs present a significant burden to healthcare cost. The United States of America estimates a total annual expenditure for diabetes care of $176 billion.21,22 whilst that of treating an infected DFU resulting in below knee amputation estimated at $190 000 in 2012 in the US. 23 In the UK, the cost of treating a DFU averages at €10 000 and €17 000 for a non-infected and infected ulcer respectively. 24 In Singapore, the annual direct cost for minor amputations was SGD $5161, and for major amputations SGD $9695. 25
There is strong evidence that decreased lower limb amputation rates can be achieved with prompt and coordinated care by a multidisciplinary team for DFUs.26,27. Delay in treatment has repeatedly demonstrated adverse DFU outcomes of delayed healing28,29 and higher risks of lower limb amputations. 30 We aim to optimise the management of DFUs in patients with the multidisciplinary Diabetic Rapid Evaluation and lower limb Amputation Management (DREAM) clinic in our hospital. This also enables fast access to required specialists for early treatment of DFUs with the aim of minimising the need for lower limb amputations.
Materials and Methods
The DREAM clinic was set up in our hospital’s Medical Centre in 2018 to provide a fast-access outpatient multidisciplinary approach to diabetic foot complications. We sited ourselves for fast-access referrals for DFUs.
Inclusion criteria to the DREAM clinic and therefore our study are: adults >21 years old, known diagnosis of DM and presence of foot ulcer (defined as below ankle ulcer). Exclusion criteria are: haemodynamic instability or sepsis.
The DREAM clinic operated daily on weekdays based on a workflow as shown in Figure 2. Podiatrists were the first point of contact in the clinic for accurate triage to determine one or more appropriate specialty reviews required from endocrinology, vascular surgery and orthopaedic surgery. Those with poor glycaemic control defined by a glycated haemoglobin (HbA1c) level of more than 8.0% (64 mmol/mol) at presentation were optimised by the endocrinologist to stem the root cause.

Overview of DREAM workflow.
Podiatrists first assessed the patient’s diabetes history, lower limb vascular flow and neurological status, as well as examined the wound in particular for infection. Additional tests such as radiographs, arterial or venous duplex scans and wound tissue cultures were arranged after discussion with the specialist. Subsequent outpatient management were with the podiatrist and relevant specialists on a case-to-case basis. Those needing urgent inpatient intervention were admitted with predetermined care plans to initiate timely treatment.
De-identified case data was collected between August 2018 and September 2021 including baseline demographics, source of referral and wound characteristics. Outcome data collected included time from initial presentation to first specialist review, type of wound treatment received, as well as foot and wound outcomes. Wound outcomes encompassed major and minor amputations, other surgical procedures as well as wound healing rates. In our study, we defined limb salvage as patients not requiring major amputation. Data on the specialties referred were also collected.
Data was processed using Microsoft Excel spreadsheet 2016 version. Descriptive statistics were used to describe patient demographics and wound characteristics. Percentages and frequencies were calculated for categorical variables. The variability of continuous variables was assessed by their confidence intervals, taking account of the mean and standard deviation (SD) in the calculation.
Institutional Review Board (IRB) approval was sought, and permission was granted to go ahead with no further ethics review required. Written informed consent was deemed not required by IRB as this is a clinical service and patient details were de-identified (IRB reference number 2019/2087).
Results
Baseline demographics are shown in Table 1.
Baseline demographics of participants in DREAM clinic.
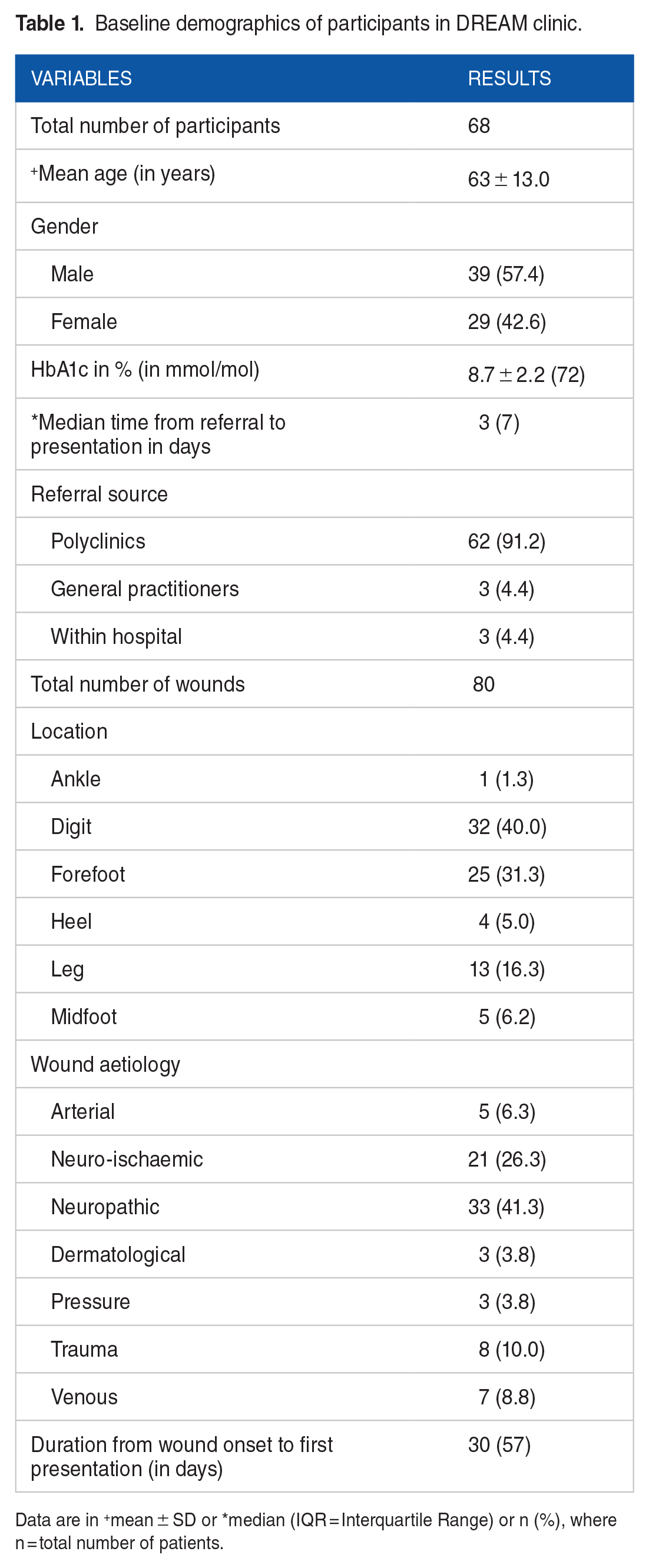
Data are in +mean ± SD or *median (IQR = Interquartile Range) or n (%), where n = total number of patients.
Sixty-eight participants were seen in the DREAM clinic from August 2018 to September 2021. Thirty-nine (57.3%) were males whilst 29 were females and a mean age of 63 ± 13.0 years. Sixty-two (95.6%) were referred from primary care whilst 3 (4.4%) were referred from within the institution. All the participants had DM at presentation with a mean HbA1c of 8.7 ± 2.2% (72 mmol/mol).
There were 80 DFUs in 68 participants. The most common aetiologies of the DFUs were neuropathic and neuro-ischaemic ulcers, making up 33 (41.2%) and 21 (26.3%) of wounds, respectively.
Outcome data is presented in Table 2.
Referral specialis discipline at week 0 and outcomes at week 4 and week 12.

From participants on podiatrist follow-up.
Data are reported as n (%), * with respect to the total number of participants and +with respect to the number of wounds on follow-up.
Included participants who underwent amputation and debridement.
The median time from date of referral to first DREAM clinic review was 3 (IQR 7) days. Of the 68 participants, 57 (83.8%) were evaluated by 1 specialist during the DREAM clinic visit while the other 11 (16.2%) required more than 1 specialist consult during the initial visit. Out of the 68 participants, 20 (29.4%) had DFUs which were managed inpatient in admission; 4 were offered admission but declined. The other 44 participants were deemed suitable for outpatient DFU management.
At 12-weeks follow-up, 1 (1.4%) had undergone major amputation, 9 (13.2%) required minor amputation, 4 (5.7%) underwent surgical debridement. Twelve (17.6%) underwent revascularisation. The other 47 (69.1%) did not require surgical management of their DFU. The only one who underwent the major amputation had osteomyelitis at first presentation to DREAM clinic. Hence, the limb was deemed unsalvageable at the outset. No attempt was made to salvage the limb as major amputation was determined to be as the most appropriate immediate intervention.
We report a 100% limb salvage rate for the remaining 67 patients for the duration of the 12-week follow-up period.
Of the 47 patients who did not require any surgical management, 24 were followed-up by the podiatrist and received specialised wound treatment, with wound care and offloading advice. These 24 patients had 28 DFUs in total, with 20 DFUs (71.4%) having healed at the 12-week follow up mark. The mean healing duration was 8.9 ± 7.5 weeks. Of the unhealed DFUs at the 12-week mark, 2 out of the 8 wounds (25%) eventually healed spontaneously with a mean wound healing duration of 37.4 ± 21 weeks. For the remaining 6 unhealed DFUs, 1 was lost to follow-up, 1 remained unhealed on Podiatry review, 2 required minor amputation and 2 required debridement. For the 4 DFUs that required surgery subsequently, the DFUs healed at a mean duration of 22.4 ± 9.6 weeks post-surgical intervention.
Healing outcomes were poorer for wounds in patients with multiple DFUs. In Table 3, wounds in patients with multiple DFUs show a 50% healing rate, compared to 83.3% healing rate for wounds in patients with a single DFU.
Wound healing outcomes at week 12 for wounds in patients with single versus multiple DFUs.

Data are reported as n (%) with respect to the number of wounds on follow-up.
Discussion
DFUs are managed through a three-tiered approach:
(I) Primary prevention through optimal glycaemic control and management of comorbidities,
(II) Secondary prevention through early detection of an at-risk foot with prompt referral to tertiary centres, and
(III) Prompt management of diabetic foot ulcers to prevent amputation.
Our DREAM clinic targets level (III) by managing pre-existing DFUs to stem disease progression requiring amputation. In recognising the effect of delayed treatment on delaying healing and high lower limb amputations rates, considerable efforts were aimed to reduce the time taken from point of referral to specialist consult.
From our data, 62 patients (95.6%) were solely referred to our DREAM clinic from primary care with no direct referral to specialists. The median time from primary care referral to DREAM clinic specialist consultation was 3 (IQR 7) days, compared to 10.1 days in another local study 31 . The median time from wound onset to presentation in DREAM clinic is 30 days (IQR 57). Smith-Strom et al reported that wounds presenting 52 days or more after the onset of ulcer had a 58% (SHR 0.42, CI 0.18-0.98) reduced rate of healing compared to wounds referred earlier. 29 This further emphasises the importance for DFU to be seen as soon as possible for initiating adequate appropriate treatment.
Based on IWGDF guidelines, it is recommended that an interdisciplinary foot care team comprising of a diabetologist, orthopaedic surgeon, vascular specialist, infectious disease specialist, podiatrist, diabetes specialist nurse, prosthetist and orthotist working together within the same centre is the most ideal for best limb salvage rates. Of the patients seen in the outpatient DREAM clinic, 11 (22.9%) required more than 1 specialist consult during the initial visit, demonstrating complex medical profiles necessitating multi-specialist management. A multidisciplinary team clinic is therefore beneficial by allowing patients access to multiple specialists during the same visit. A study in Singapore reported decreased minor (10% vs 23%, P < .05) and major amputations (5% vs 11%) with the set-up of a fast-access outpatient multidisciplinary team comprising of vascular surgeons, endocrinologists, podiatrists and wound nurses for DFUs with a background of peripheral vascular disease. 31 This is comparable to our findings whereby 9 patients (11.3%) required minor amputation, and 1 (2.5%) underwent major amputation. Another Singaporean study by Nather et al 32 demonstrated a reduction of major amputation rate by 33% and length of hospital stay from 20.36 days to 12.20 days after adoption of an inpatient multidisciplinary team.
Internationally, similar outcomes were reported. In China, Wang et al 33 proposed a detailed guide for diabetic foot management, which included the formation of a multidisciplinary team for diabetic foot management. They reported a decline in major amputation rate from 9.5% to <5% after a team-based approach to diabetic foot care was introduced. 34 This was similar to studies by Anichini et al 35 where major amputation rate reduced from 10.7 per 100 000 to 6.24 per 100 000 after 5 years of implementing a multidisciplinary team in Italy. Krishnan et al 36 had a 62% reduction in major amputation rate over 11 years with similar service in the UK.
In our study, 20 out of 28 DFU wounds (71.4%) healed with conservative management after 12 weeks with regular podiatry review, dressing and offloading, compared to 33.6% in a sister public tertiary hospital without the set-up of DREAM clinic. These findings highlight the role of the podiatrists as part of the multidisciplinary healthcare team in DFU care.
Singapore has well-established guidelines for both diabetes management and annual screening for diabetic foot complications for primary prevention of DFUs as shown in Figure 3, which represent levels (I) and (II). Those identified to be high risk will be reviewed more frequently with onwards referral to Podiatry if any foot complications are identified. This is corroborated by the literature reporting reduced major and minor amputations with screening and treatment protocols.37,38 Traditionally for more severe findings such as an infected ulcer or gangrenous foot, the patient will need to be referred from primary care to a hospital specialist or emergency department for further management. Additional waiting time is then required to engage the relevant foot specialist for review depending on the level of urgency. This stepwise workflow results in unwarranted delays and may also discourage patients from seeking further management of their DFUs, hence reducing the likelihood of limb salvage.

Workflow for diabetic foot screening (adapted from Ministry of Health Singapore 39 ).
The management of DFUs may vary between healthcare professionals, influenced by experience and institutional or professional guidelines such as the IWGDF, American Diabetes Association and NICE guidelines. Having a multidisciplinary approach to DFU management not only helps to hasten and streamline the process for patients, but also allow for opportunities for healthcare professionals in different fields to collaborate for establishing high quality standard care.
To our knowledge, our study is one of the few globally and the first in Southeast Asia to have a multidisciplinary DFU team where podiatry serves as the patient’s first point of contact. We find this approach empowers podiatrists to accurately triage a patient with DFU and guide the patient to the relevant specialists as required. This triage allows accurate selection of specialist referrals, keeping costs low for the patient and healthcare system. For instance, patients seen in the DREAM clinic requiring surgical specialist input are often seen by either the vascular or orthopaedic surgeon after the initial podiatric assessment, rarely by both.
Our study is not without limitations. Firstly, we lack data on the cost effectiveness of this arrangement. Though we postulate that the accurate triage and referral of patients would bring about significant cost reductions, the health economics and cost-effectiveness of this arrangement requires further evaluation. Qualitative aspects of this experience also needs to be investigated from the parties involved to explore challenges in collaboration and streamline workflow.
Secondly, the data analysed in this study were from our first 68 patients enrolled in the DREAM clinic with the opening of our hospital. This poses 2 inherent and important limitations. First of all is the lack of a control group for comparison as all DFUs referred to our hospital from the outset were directed to the DREAM clinic, with no concurrent or pre-existing non-multidisciplinary DFU clinic. The second limitation is that sample size power analysis was not performed for this study. Therefore, we are unable to conclude the statistical significance of reduction in amputation rates and improvement in outcomes within the same institution. We were only able to compare our outcomes with other studies with published data on DFU management outcomes.
The third limitation pertains to the short duration of follow-up. In September 2021, the last of these 68 patients reached the 12-week follow-up visit. While promising results have been achieved, we are continuing to keep track of our patients’ outcomes in the DREAM clinic.
Conclusion
DFUs and their attendant complications are not only costly to manage but also debilitating to patients. Early multidisciplinary care is essential to prevent untoward downstream effects. Our new approach of a fast-access multidisciplinary clinic with initial podiatric assessment has shown promising outcomes. Further studies evaluating the cost-effectiveness and long-term benefits of this approach are necessary to support its feasibility for widespread implementation.
Footnotes
Acknowledgements
We would like to acknowledge Dr Anandakumar Vellasamy, Dr Loh Jiashen, Mr Jackie Tey and staff of Sengkang General Hospital, in particular the Department of Podiatry, Department of Endocrinology, Department of Orthopaedic Surgery, and Singapore General Hospital Department of Podiatry, who were critical for the inception and piloting of this project to its current stage.