
Abstract
The COVID-19 pandemic has changed many aspects of people’s lives, including not only individual social behavior, healthcare procedures, and altered physiological and pathophysiological responses. As a result, some medical studies may be influenced by one or more hidden factors brought about by the COVID-19 pandemic. Using the literature review method, we are briefly discussing the studies that are confounded by COVID-19 and facemask-induced partiality and how these factors can be further complicated with other confounding variables. Facemask wearing has been reported to produce partiality in studies of ophthalmology (particularly dry eye and related ocular diseases), sleep studies, cognitive studies (such as emotion-recognition accuracy research, etc.), and gender-influenced studies, to mention a few. There is a possibility that some other COVID-19 related influences remain unrecognized in medical research. To account for heterogeneity, current and future studies need to consider the severity of the initial illness (such as diabetes, other endocrine disorders), and COVID-19 infection, the timing of analysis, or the presence of a control group. Face mask-induced influences may confound the results of diabetes studies in many ways.
Introduction
Coronavirus, an RNA virus from the Coronaviridae family is the responsible agent for the COVID-19 pandemic. 1 An epigenetic change influences the immunological response to infections, including COVID-19. The gender-based influence has been observed in several respiratory and autoimmune disorders. 2 The propensity of mortality rate due to COVID-19 was significantly higher in females than in males. Notably, social norms, financial and non-financial barriers to women’s access to healthcare have proposed to negatively impact women’s testing for COVID-19 and access to adequate care, resulting in underreporting of female cases and deaths due to COVID-19. 3 It has been suggested that sex differences in immunopathogenesis may be suggestive of mechanisms of COVID-19 based on the available sex-disaggregated epidemiological data from the COVID-19 pandemic. This could help identify points for improved vaccine design and therapeutics to increase the efficacy of the vaccine.
The spread of COVID-19 has changed many aspects of people’s lives, including individual social behavior,4-6 and healthcare procedures.7,8 It has also altered physiological,4,6,9-13 as well as pathophysiological responses.14,15 There is a possibility that some medical studies may be influenced by one or more hidden powers brought about by the COVID-19 pandemic.
Individuals with diabetes are more prone to Coronavirus infection. 1 Type I diabetes (TDM) is associated with higher COVID-19 mortality, 16 and pre-existing diagnoses of diabetes have a negative impact on mortality in patients infected with COVID-19. 17 It influences other diabetes-related conditions, thereby creating some multiple hidden confounding factors. On the other hand, cardiac complications such as heart failure, myocardial damage, and arrhythmias are common in patients infected with COVID-19, regardless of diabetes. 18 This situation can lead to subtle interactions between variables. The type of drug or vaccine17,19 may be another confounding factor further complicating results and interpretations. For example, the results derived from a randomized clinical trial showed that prescribing reparixin (allosterically binds to CXCR1 and prevents it’s activation by binding to it’s ligands IL-8/CXCL8) to patients at high risk of in-hospital mortality improved survival by inhibiting CXCL8 activity without increasing the risk of infection. 20 It is easily comprehended from this study that how such, seemingly superficial association can be crucial in the context of treatment options for COVID-19 patients e.g., an association between COVID-19 with hypertension and acute kidney injury (AKI). AKI is a frequent side effect among Asian COVID-19 patients, and it has been linked to a higher rate of COVID-19 related mortality in Asian patients. 21 In these investigations, careful handling of data is a must. The fact that access to healthcare of the same degree and caliber was not universal before, during, and after the COVID-19 pandemic is one of many important considerations that must be taken into account.22,23 Different occupational and sociodemographic risk factors were linked to SARS-CoV-2 infection. 24 In other words, there is a complex nexus of factors that interact with one another in diverse ways to produce various outcomes.
Coronavirus effected endocrine system specially glands such as the hypothalamus, pineal gland, pituitary, adrenal gland, testis, ovary, pancreas, thymus, and thyroid gland (Figure 1).
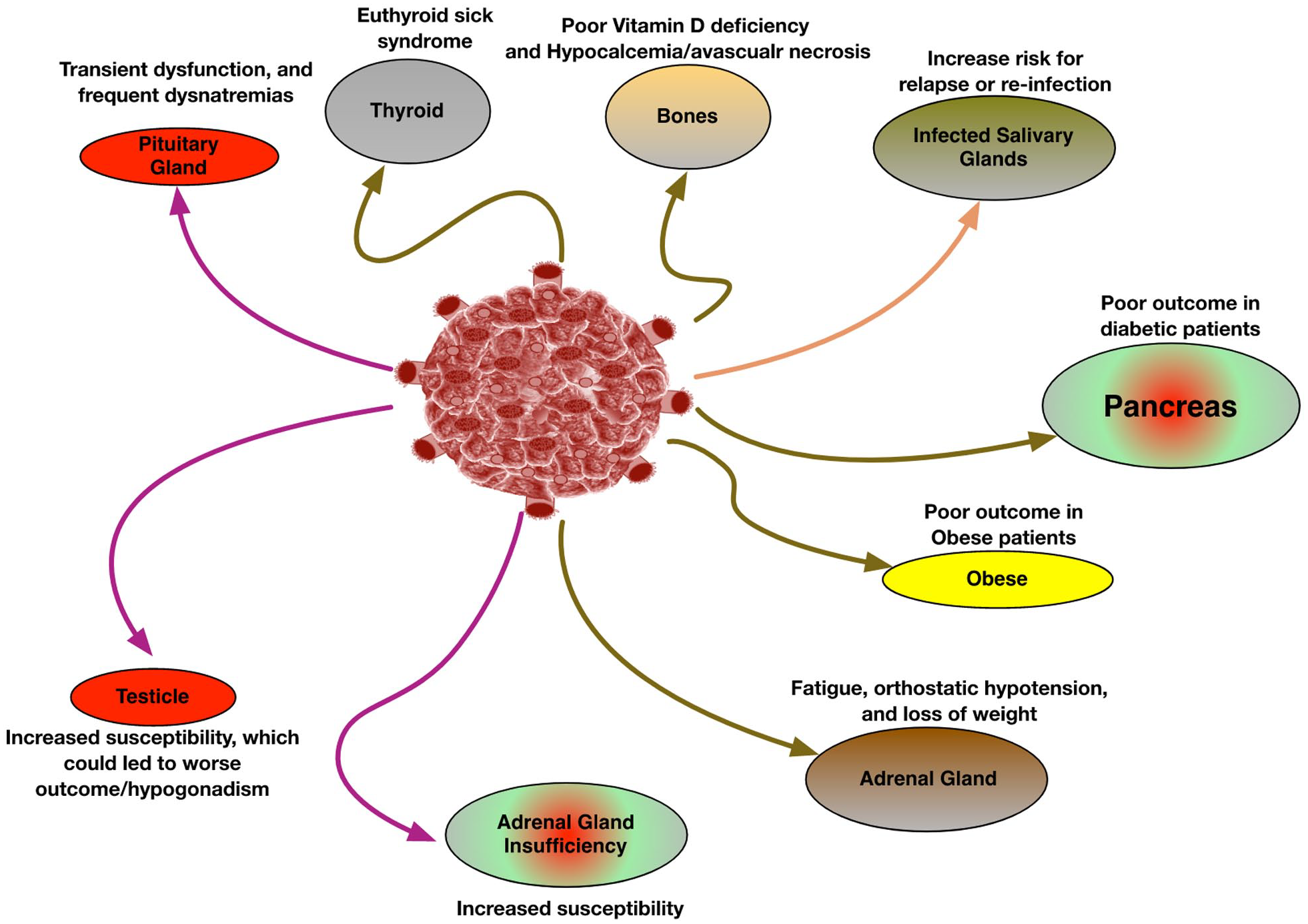
SARS-CoV-2 infection and association with different components of the endocrine system including glands such as pituitary, adrenal, and thyroid glands.
Healthcare workers were forced to wear masks and respirators in addition to personal protective equipment (PPE) during the COVID-19 pandemic. Face mask usage is a significant element in this circumstance. N95 and Medical masks can protect against SARS-CoV-2. Medical masks defend from large respiratory droplets, but N95 masks protect against microscopic airborne particles, including aerosols. 25 This is the main distinction between the 2 types of masks. The surgical masks are not intended to offer users respiratory protection because they can not efficiently filter minute airborne particles. 26 In N95/FFP2 respirators and surgical/medical masks, the particle penetration rates are ~5%, and 30%-70%, respectively. 27 The major distinction between respirators with the “N” (N95, N100) versus “P” designations (P100) is that the former are more susceptible to oils. N, R, and P, which stand for non-oil resistant, slightly oil-resistant, and strongly oil-resistant/oil-proof, are the 3 main varieties of facepiece filters, respectively.28,29
In healthy individuals, wearing a face mask during exercise can have a small negative impact on a variety of physiological and psychological variables, including pulmonary function, gas exchange, and subjective discomfort.30,31 However, other systematic reviews and meta-analyses have revealed that the use of masks by a healthy adult population during physical exercise may exert negligible effects on the physiological, perceived, and cardiorespiratory responses. 32 Diabetic patients already have impaired pulmonary function 33 so this problem only makes the situation more complicated. In both COVID-19 and non-COVID-19 young adult pneumonia patients; there is a significant gas-exchange deficit and systemic hypoperfusion; in contrast to COVID-19 unrelated pneumonia, the outcome of COVID-19 pneumonia appears to be more strictly correlated to the extent of lung damage rather than to the systemic circulatory and metabolic abnormalities typical of sepsis. 34 The quantitive analysis of the PaO2/FiO2 ratio is another problem. While it has been reported that relying on a single evaluation of PaO2/FiO2 ratio, especially at high FiO2, could be misleading in COVID-19, the majority of the reported studies had used one. 35
Other undetectable sources of power exist, but are frequently disregarded or ignored. The interpretation of metabolic profiling of urine requires normalization considering which variation in urinary dilution is a good example.36,37 Commonly used in metabolomics, probabilistic quotient normalization is vulnerable to systematic variation that is observed in >50% of the spectral profile. 36 To account for this, Correia et al developed a novel method. They claimed that before determining the normalization coefficient, proteinuria, a frequent but underappreciated cause of influence in 1H NMR (Nuclear magnetic resonance) metabolic profile studies, can be successfully controlled using Small Molecule Enhancement SpectroscopY that is, SMolESY or other macromolecular signal suppression methods. 38
For methodological reasons, the interpretation of clinical results, methodological procedures, and comparative research, both pre- and post-pandemic, depend on the acquisition of these hidden influences. In this review, we are providing literature-based evidence reporting the COVID-19 influence on endocrine and diabetes research, with the hope that the scientific community will gain an overall understanding of various forms of influence/partiality/power that might arise during the data collection, analysis, interpretation and comparison in cross-sectional and explorative questionnaire research addressing the incidence, prevalence, severity of endocrine illnesses. Additionally, the influence imposed by COVID-19 affects deep learning, artificial intelligence, and many aspects of brain imaging.
We are describing the studies that are confounded by facemask-induced induced influence and COVID-19, as well as how these partialities might be made more complicated by additional confounding variables. For instance, social distance brought on by COVID-19 has had a detrimental effect on a number of mental health outcomes. 39 The results are further complicated by a number of other factors that interact with COVID-19 and facemask-induced partiality. During the COVID-19 pandemic, there were alternations seen in (1) physiology, (2) pathophysiological responses, (3) social changes, and (4) metabolic consequences. It is clear that COVID-19 has a wider influence than just these particular cases and can be applied to other similar situations. In this review, we covered some of the recently completed, and ongoing studies on these aspects.
Alterations in Physiologic Responses
Respiratory responses
In numerous circumstances throughout the COVID-19 era, N95 respirators were utilized often. A significant number of studies discussed issues brought on by the prolonged use of respirators, with mixed results. A recent systematic review and meta-analysis (which was based on 13 studies) was able to determine the effects of the N95 respirator. While oxygen saturation did not change during low- to moderate-intensity physical activity, borderline lower oxygen saturation and higher carbon dioxide partial pressure were noted. According to this study, using N95 respirators while performing high-intensity physical exercise may statistically affect, but not necessarily have a clinically meaningful impact on, the physiological changes in oxygen, and carbon dioxide. The emphasis was on the user’s susceptibility to clinical signs of hypoxia and hypercarbia for the early diagnosis of negative effects of N95 respirators if they had certain medical conditions, such as respiratory issues. 13
To assess the direct relevance of this subject, additional shreds of evidence are required pertaining to the physiological aspect. Although these connections may appear insignificant at first look, they undoubtedly confound the studies and taint the outcomes. When exposed to acute normobaric hypoxia, the blood glucose level in healthy persons remains constant. 40 Additionally, combined resistance and aerobic training in normoxia or normobaric hypoxia have no effect on metabolic control in men with type 1 diabetes 41 ; however, physical training in hypoxic conditions may partially enhance the favorable effects of exercise alone on myocellular insulin sensitivity in obese men with metabolic syndrome through changes in VEGF levels. 42 It’s interesting to note that patients with diabetic foot ulcers (DFU) have an inverse relationship between miR-210 and HIF-1 (hypoxia associated gene) expression, suggesting that miR-210 may control HIF-1 expression. 43 In a recent study, which included 2 groups of tissue samples (control and type 2 diabetes mellitus ie, T2DM with DFU) and three groups of circulation samples (50 in each group of healthy volunteers, T2DM patients, and T2DM patients with DFU), it was discovered that HIF-1 expression decreased in DFU patients while miR-210 expression increased in both tissue biopsies and circulation. In comparison to T2DM patients and healthy controls, the expression of the inflammatory genes TNF- and IL-6 in the blood was higher in DFU. VEGF expression remained unchanged, while anti-apoptotic BCL2 was downregulated and BAX and caspase 3 were elevated in DFU tissues compared to control. 43 We can wonder if the results of the latter study, which was undertaken during the COVID-19 epidemic, would have been the same if it had been done under more typical circumstances, that is, before the pandemic.
During the COVID-19 pandemic, Hajhosseini et al carried out a study in which they proposed that a favorable early reaction to hyperbaric oxygen therapy, that is, improved perfusion, would be an early indicator of eventual response to the treatment, that is, wound healing. They enrolled two groups: patients with chronic wounds (n = 14), and healthy controls without wounds (n = 10). Adults with only one active Wagner grade III diabetic foot ulcer or soft-tissue radionecrosis would were also included. In contrast to their controls (who underwent two consecutive sessions), patients with chronic wounds received 30 to 40 consecutive sessions of hyperbaric oxygen therapy administered once daily, 5-days/week. Before and after the sessions, they performed indocyanine green angiography and examined the perfusion patterns. Healing was determined clinically and defined as full skin epithelialization with no clinical evidence of wound drainage. Unlike unwounded healthy controls, a significant increase (p < .03) in indocyanine green angiography perfusion was seen in chronic-wound patients right after the therapy. A total of 100% of the wounds that demonstrated improved perfusion from sessions 1 to 2 went for healing within 1 month of completion of hyperbaric oxygen therapy, compared with none in the subgroup that did not demonstrate improved perfusion (p < .01). 44 This study indicated a beneficial effect of hyperbaric oxygen therapy on perfusion in chronic wounds through improving angiogenesis and ameliorating hypoxia.
As there is no information available regarding the compliance with facemask wearing among participants of similar studies,13,40-44 the literature review clearly indicates that face mask wearing practice (i.e., type of face mask, duration of wearing a face mask, etc.) can confound the results if proper methodological precautions are not taken.
The research with designs merits the same criticisms. For instance, it has been suggested that aerobic exercise may help older persons with their cognition and cerebrovascular control. Guadagni et al recruited 206 healthy, low-active middle-aged and older individuals (mean SD age 65.9 6.4 years) to participate in a supervised Six-month aerobic exercise intervention in order to test the hypothesis. Patients were evaluated both during and following the intervention. 45 This study used a single-group pre/post-intervention quasi-experimental design. Numerous tests were employed, including transcranial doppler ultrasound and neuropsychological tests, to measure the cerebral blood flow velocity and cognition before and after the intervention. It was determined that improvements in cerebrovascular control and some cognitive areas were linked to the six-month aerobic exercise intervention. In addition, their subsequent investigations revealed a unique relationship between cognitive alterations and adjustments in cerebrovascular control during euoxic hypercapnia and in response to submaximal exercise. 45
The use of a facemask would affect the study’s interest parameters. A crossover design, in which each participant serves as his or her own control, may be a more effective way to learn the influence of such variability given the lack of a validated questionnaire to determine the extent of facemask use. 45
Salivary responses
The rate of salivation and taste degradation are closely related. 46 Changes in eating habits and appetite loss can result from taste impairments, which may have an impact on diabetes and endocrine disorders. 47 The outcome of oral studies in diabetics can be significantly impacted by the significant relationship between COVID-19 and oral diseases, 48 which is mediated by hyposalivation COVID-19-induced, which can in turn drastically impact the results of oral studies in people with diabetes. Researchers hardly ever take note of this subsequent prejudice. As it is not well established that COVID-19 infections can spontaneously lead to severe hyposalivation through direct damage to the salivary glands, it would be interesting to know in future investigations whether any of the patients are/were infected by the coronavirus. 49
Based on the meta-analysis published by Nijakowski et al, 50 almost two-thirds of the COVID-19 patients reported oral symptoms, in particular xerostomia, taste alterations, and ulcerations, 37.58% [95% CI: 26.35%-49.53%], (54.73% [95% CI: 46.28%-63.04%], and 21.43% [95% CI: 13.17%-31.06%], respectively. Due to the potential linkage of other factors, such as individual and/or environmental factors, it is impossible to determine if oral signs of COVID-19 infection are more common. 50 It is crucial to keep in mind that infected patients are not proportionally affected by these symptoms, creating another hidden partiality that may not be adequately addressed by methodological measures like randomization procedures unless a cross-over design is used, which may have its own limitations like the transfer partiality, a long-established and frequently ignored problem of asymmetrical transfer in cross-over designs. 51
Therefore, it’s crucial to distinguish between COVID-19 as a whole and the xerostomia (dry mouth produced by a lack of saliva in the mouth) and/or hyposalivation induced by diabetes. However, there is another unnoticed aspect connected to the practice of wearing face masks. Studies that aim to establish a direct causative link between the duration of diabetes, the degree of hyposalivation and/or xerostomia, and oral issues are one such example.52-54 Mandatory face mask wearing during COVID-19 can physically impede mandibular jaw movement 55 and thereby drastically impair lacrimation and salivation per se de facto, irrespective of diabetes severity and or duration and or glycemic control. 56 Since there is a drastic between-individual difference in terms of face mask wearing, 57 the severity and/or degree of facemask-induced hyposalivation—and thereby concentration of measured salivary variables concentration (or tear film concentration)—would be expected to be different in the study arms. A similar opinion applies to the results of ophthalmologic investigations, due to neurophysiological and anatomical reasons.58-60
Future research is necessary to explore if the randomization procedure was successful and whether major variables that potentially influence the salivary flow rate and lacrimation should be taken into account and analyzed to look for imbalances between study arms. It is fair to mention that masticatory performance was independent of salivary flow or anthropometric parameters in healthy young adults. 61 However, it’s interesting to note that it is not true in the case of abdominal obesity, as it has been noted that among the Japanese population, higher stimulated salivary flow rate, a surrogate marker for mastication ability, is significantly associated with lower prevalence of overweight, abdominal obesity, and elevated skinfold thickness. 62 Irrespective of energy intake and physical activity, the latter scenario might introduce another prejudice into metabolic studies.
It is important to note that after therapy for COVID-19 infection, xerostomia is the most common finding, in the females, 63 who are likely to experience abnormalities associated with taste and smell. 64 When planning any study, these findings must be taken into consideration because they are highly pertinent. The researchers would be interested to learn that there is a sizable regional variation in the prevalence of the taste change symptom before and after the COVID-19. 64 For instance, within the first month of symptom onset, a significant rate of recovery for COVID-19-related olfactory and gustatpry impairment has been documented. In comparison to those infected during the second pandemic wave, the mean recovery time (35.07 ± 4.25 days) for olfactory dysfunction was significantly longer (21.65 ± 2.05 days) in those infected during the first epidemic wave (p = .004). In the case of gustatory impairment, a similar pattern in recovery time was seen (p = .005). 65
Researchers can envision what would occur if a study attempted to, e.g., measure salivary slow, protein composition, and rheology after taste and transient receptor potential channels stimulation in diabetic participants without asking pertinent questions about the history of COVID-19 infection and/or facemask wearing practice.
In research where salivary cortisol reduction is employed as a biomarker to assess the suppression of the hypothalamus-pituitary-adrenal axis (HPA), 66 there are numerous cases that are identical, and scientists can readily generalize the interpretation to more severe scenarios.
Additionally, changes in salivary cortisol immediately prior to 25 minutes after a psychosocial stressor onset have been used to predict memory for affective words. It has been demonstrated that exposure to the acute laboratory stressor (ELS) activates the HPA axis. An increased cortisol reactivity is reported to be correlated with less accurate recognition of negative valence words. Among younger participants exposed to ELS, greater cortisol reactivity to acute stress is correlated with poorer recognition of dysphoric and neutral words. Acute cortisol increases may impede the processing of negatively valenced information, which has ramifications for memory on it’s own. Younger participants who are exposed to high ELS may be specifically vulnerable to the effects of cortisol, which may explain one pathway through which stress leads to psychopathology among at risk youth. 67 We can use these two scenarios53,67 to show how ignorance of this seemingly simple issue can influence the mechanistic physiological and psychological conclusions.
Neurophysiologic responses
Abnormal EEG waves are very commonly seen in COVID-19 patients and survivors.68-70 Face mask wearing practice could create a substantial influence in neurophysiological studies. It is very important to notice the unrecognized role of face mask wearing practice and their potential confounding effect on such studies. Although controversial,71,72 face masks may exert influence through other pathways. 73 For instance, they can further induce hypoxia and hypercapnia, 74 which drastically alters brain EEG patterns, 75 to mention a few. Based on it, one can argue that this very issue can create partiality in many neurophysiological studies carried out during or after the COVID-19 pandemic. For a short mechanistic explanation, see Rastmanesh. 73
One might wonder how these issues interact with endocrine research. Based on the literature-based evidence, one can find a connection after a short critical appraisal, in a scenario if the study is/was to be conducted during the COVID-19 pandemic:
Obstructive sleep apnea is a risk factor for insulin resistance in non-diabetic adults 76
Longer or short-term sleep deprivation may negatively affect glucose homeostasis 77
The salivary microbiome is altered in the presence of a high salivary glucose concentration 78
Hyperglycemia is associated with simultaneous alterations in electrical brain activity in youths with type 1 diabetes mellitus 79
Melatonin synthesis impairment as a new deleterious outcome of diabetes-derived hyperglycemia 80
We also suggest that threshold-free cluster enhancement and polysomnography methods be urgently reviewed in settings and events whenever/wherever yawning behavior is altered for any reason, including but not limited to wearing a face mask, in order to control this type of confounding effect.
The COVID-19 pandemic has led to changes in many aspects of our daily lives, including the widespread use of face masks. While it is difficult to predict exactly how the abandonment of face mask wearing will impact sleep EEG signatures or other measures in patients with COVID-19, it is possible that there could be some changes in the post-pandemic period. It is important for future studies to carefully consider any potential confounding factors that may arise due to changes in behavior or other factors related to the pandemic. This may include adjusting study design or analysis methods to account for any differences that may be present between pre- and post-pandemic periods.
Pathophysiologic responses
Pathophysiologically, COVID-19 infection has been associated with altered male reproduction, 81 olfactory dysfunctions, 82 abnormal liver function tests, 83 neurologic conditions, 84 cerebrovascular events, 85 hypovitaminosis D, 86 dysgeusia, 87 obesity, 88 and perturbations in energy homeostasis 89 just to mention a few. For instance, high-energy expenditure driven by a high metabolic state induced by the host response may quickly lead to depletion of the micronutrient. This deficiency, in turn, can result in alterations in free radical damage, normal energy homeostasis, and immune system derangement. 90 If pertinent influences have been overlooked, such observations can be easily misinterpreted. Another illustration is the renin-angiotensin system (RAS), which has drawn a lot of attention because, in addition to it’s effects on blood pressure, fluid, cellular growth and development, and electrolyte balance, it may also play an important role in maintaining energy homeostasis. The angiotensin-converting enzyme (ACE) - angiotensin II pathway is activated in metabolically-related organs like the liver, skeletal muscle, pancreas, and adipose tissue, where it affects insulin secretion, fat distribution, glucose transport, the production of, adipokines. The insulin signaling pathway, inflammation, stress state, local microcirculation, and structure remolding can all be improved by activating the ACE2-angiotensin (1-7) pathway, which has the opposite role in the ACE pathway. 91 The protective RAS arm can significantly boost brown adipose tissue. As a result, increased ATP synthesis occurs less often and more energy is expended as heat instead of regular.
A systematic review and dose-response meta-analysis showed that high admission blood glucose independently predicts poor prognosis in COVID-19 patients. 92 Furthermore, the infectious power of COVID-19 (and other coronaviruses) is directly dependent on cholesterol present in the membranes of cells, 93 which is, in turn, a function of many different variables including diet, physical activity, and genetics. In completed and ongoing studies, one can consider the confounding effect of commonly prescribed statins and other possible cholesterol-chelating agents (like methyl-β-cyclodextrin).
Another meta-analysis is currently underway to evaluate the association between different digestive symptoms and the severity and mortality of patients infected with COVID-19. 94 The potential mechanistic links between obesity and worsening COVID-19 from altered physiology, underlying diseases, metabolism, immunity, cytokine storm, and thrombosis have been reviewed elsewhere and readers can see.95-99
In many cases, the magnitude of clinical and methodological heterogeneities and the hidden influences precluded conducting meta-analyses and establishing a connection between a higher body mass index (BMI) and the prognosis of COVID-19 infection in many studies. 100 Here, it is worth reminding that the main complications of COVID-19 infected death include energy-related diseases, such as T2DM. 92 The majority of the studies were susceptible to bias due to confounding caused by indications of comorbidities, which ultimately results in a greater death rate. As an example, in the case of acromegaly pituitary gland have hyper-secretion of growth hormone. 101 Also, patients with pituitary abnormalities should have their systemic comorbidities, such as diabetes mellitus, hypertension, obesity, and fractures, well managed in order to prevent SARS-CoV-2 infection and catastrophic outcomes due to COVID-19. These circumstances might also have a negative impact on COVID-19 results. 102 One major issue in different studies was the lack of a control group with non-COVID pneumonia or acute respiratory distress syndrome of comparable severity to evaluate the role of the endocrine system in COVID specificity. 103
Conclusion
The severity of the original illness (including COVID-19 infection, diabetes, and endocrine disorders), the timing of the analysis, or the availability of a control group must all be taken into account in current and future studies to account for heterogeneity. In many ways, face mask-induced bias might skew diabetes study findings. When analyzing data in an effort to distinguish between symptoms that are truly caused by the endocrine system and those that are confused by wearing a facemask, this partiality may have interaction and/or modification effects in various circumstances, differentially. Therefore, it is essential to distinguish between various diseases with appropriate clinical precautions; as a first step, it is important to gauge the extent of this partiality to make the necessary statistical adjustments, and take the necessary actions to prevent incorrect interpretation of clinical and epidemiological data. The length of time spent wearing, the frequency with which it is changed, the thickness, kind, sealing, and tightness of the face mask are a few independent variables that may influence the degree of confounding factors brought on by face masks. We spoke briefly about the potential causes and processes for this prejudice. The actual method by which wearing a face mask might subtly change diabetes research could be dyspnea, hypercapnia, hypoxia, and/or headache thereafter.
If it proves that the magnitude of confounding factors due to face mask wearing is high, it will be a transition confounder. For example, it would be expected that the effectiveness of clinical trials and other interventions intended to improve glycemic control would be underestimated or attenuated; on the other hand, it would be expected that the severity, incidence, and prevalence of some medical conditions in diabetic patients would be artificially overestimated. This influence has significant effects on current clinical trials, including the extrapolation of retrospective/prospective data in various settings, systematic review criteria, and meta-analyses (pre-COVID-19 vs post-COVID-19), but more importantly, the re-interpretation of prior findings and comparative studies. Overall, a number of aspects connected to the COVID-19 pandemic were extremely important for endocrine research. According to evidence from numerous studies, we must consider confounding variables related to COVID-19 prior versus post-COVID-19 scenarios while planning any investigation. Further, a guideline for future study designs is required which would depend on many different characteristics of the question of interest, the study design, the population of the study, the sampling methods, the statistical plan, and the involvement of good control in the study.