
Abstract
Background:
Diabetic retinopathy (DR) is an important microvascular consequence of long-term type 2 diabetes mellitus (T2DM), and it can lead to blindness if not properly diagnosed and managed. Nailfold video capillaroscopy (NVC) is a non-invasive technique for observing capillary microvasculature.
Aim:
We aimed to evaluate the nail folds capillaroscopic alterations in patients with T2DM by NVC and correlated the results to DR, and their relation to disease duration and hemoglobin A1c (HbA1c).
Methods:
This cross-sectional study enrolled 62 cases with T2DM (as per the American Diabetes Association criteria). All patients were subjected to NVC and ophthalmological assessment.
Results:
NVC revealed that Patients with DR showed significantly higher frequencies of tortuous capillaries, branched capillaries and precapillary edema versus non-DR patients with P < .05. The DR patients with longer disease duration (15-20) years had significantly higher frequencies of branched capillaries, tortuous capillaries, microhemorrhages, and dilated apical capillaries. The frequency of tortuosity and precapillary edema were significantly higher in patients with poor glycemic control. The increased capillary width and branched capillaries were detected as predictors of DR in multivariate analysis.
Conclusion:
NVC is a cost-effective, quick, safe, simple, non-invasive, and newly emerging tool to assess the capillaroscopic alterations in diabetic patients as an indicator of severity of DR.
Keywords
Introduction
Capillaroscopy had been innovated to evaluate microvascular morphological and functional problems in systemic illness that affects the capillaries for decades. It was designated as a “standard investigation” in rheumatologic management due to its high sensitivity and specificity, lack of invasiveness, ease of procedure, and rapid execution time at a cheap cost.1-4
The nailfold capillaroscopy (NVC) consists of a digital video camera and an optical microscope that are both connected to a computer that calibrates the data and records capillary measurements 5. It provides information on morphological and hemodynamic factors such as extension predictive value, gravity, and illness prognosis, among others.5,6
Microvascular consequences of type 2 diabetes mellitus (T2DM), such as diabetic retinopathy (DR), have been well established as a result of alterations in endothelial cells and vessel walls, as well as smooth muscle due to disturbances in glucose metabolism. Neovascularization associated with DR is linked to proliferative diabetic retinopathy (PDR).7,8 The majority of patients had no symptoms until late in the disease’s progression, when it dramatically worsened; this emphasizes the importance of NVC in determining the disease’s prognosis. 9
Despite the fact that no characteristic diabetic pattern has been encoded on NVC, morphological manifestations of microangiopathy, such as a uniform increase in capillary diameter, can be seen. 10 In a few investigations, capillaroscopic changes have been linked to the presence or absence of diabetic retinopathy. 11 So, we aimed to assess the nail fold’s capillaroscopic changes in patients with T2DM using NVC and correlated the results to the microvascular complications of the retina (DR) and their relation to disease duration and HbA1c.
Subjects and Methods
Technical design: Our study was a cross-sectional observational study that included about 62 patients with T2DM. All patients were above 18 years who fulfilled the diagnosis criteria of the American diabetes association. 12 All patients were randomly selected from Internal Medicine outpatient clinics and inpatient departments at Ain Shams University hospitals using a simple sampling approach during period from August 2019 to August 2020. Patients with rheumatic disease, known retinal diseases or with ocular media opacity precluding good fundus visualization were excluded.
Methods: All patients were subjected to full history taking and thorough clinical examination. Nailfold video capillaroscopy (NVC) was done in the rheumatology unit of Ain Shams University. All patients were acclimatized for 15 minutes before the procedure. The room temperature was adjusted between 20°C and 23°C. Then, a drop of oil was applied for better visualization.13,14 Examining 5 or 4 fingers in the hand means that 10 or 8 fingers were examined, and 4 shots were taken for each finger to evaluate the capillaries.2,15 The updated Maricq criteria were used to assess capillary distribution, density, and morphology in the nail fold capillary system. 16 Abnormal capillaroscopic outcomes were identified as tortuosity, neoangiogenesis, microhemorrhage, extravasation, avascular areas, bizarre capillary, ectatic capillaries or megacapillary.17,18 All patients underwent full ophthalmological assessment. The classification was done in accordance with the Early Treatment of Diabetic Retinopathy (ETDRS) classification. 19 Patients with new blood vessels formation are considered proliferative diabetic retinopathy (PDR), and patients with other retinal microvascular changes are classified as non-proliferative diabetic retinopathy (NPDR). Accordingly, our patients are classified into 3 groups: non-DR (36) patients, NPDR (22) patients, and PDR (4) patients. Laboratory workup included hemoglobin A1c (HbA1c) (%): with optimal control below 7%. 1
Administrative considerations: This work was accepted by the local ethical committee of Ain Shams University, Egypt, FWA 000017585 and was conducted according to the World Medical Association Declaration of Helsinki. A written informed consent was obtained from every participant after describing the study objectives clearly and briefly. All data collected remained confidential and were used for research only.
Statistical Analysis
The obtained data were coded, revised, introduced, and tabulated to a PC and statistically analyzed by a statistical package of social science) Software program, version 25 (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp). For quantitative data, mean ± standard deviation (SD) was used; for qualitative variables, frequency (n) and percentage (%) were used. To ensure that all quantitative variables were normal, the Kolmogorov–Smirnov test was used. For qualitative variables, the Chi-square or Fisher exact tests were used, while for quantitative variables, the independent sample t-test or one-way analysis of variance (ANOVA) test was used (if the data were regularly distributed), or the Mann Whitney or Kruskal Wallis test was used (if skewed data). The discriminating abilities of capillaroscopic abnormalities in distinguishing patients with diabetic retinopathy were investigated using receiver operating characteristic (ROC) curve analysis. A value of P < .05 was considered to be statistically significant.
Results
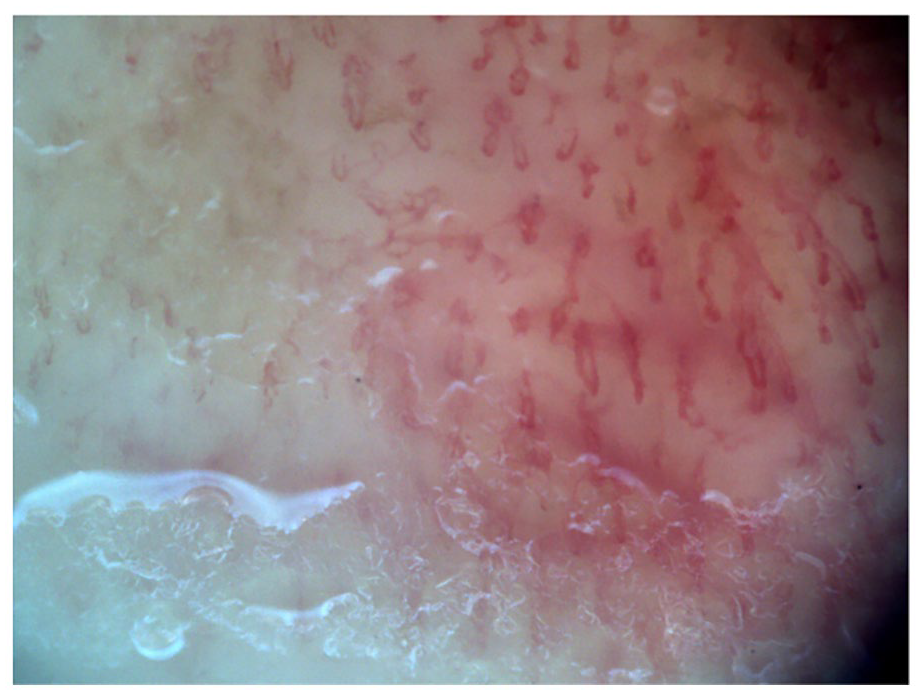
NVC results in our patients were as follows: All patients had a normal capillary density, which lies between 9 and 12 capillaries in 1 linear millimeter. Thirty-one (50%) patients had a more tortuous pattern, 31 (50%) patients had neovascularization and branched capillaries, 34 (54.8%) patients had microhemorrhages in the nail fold capillaries, and dilated apical capillary was present in only 5 (8.1%) patients. The capillary length mean ± SD was 142.73 ± 20.28 µm, and elongated capillaries were found in 46 patients. The capillary width mean ± SD was 24.97 ± 4.99 µm with 48 (77.4%) patients had dilated capillaries, and 8 (12.9%) patients presented with mega capillaries. The 62 Patients with T2DM were analyzed based on their HbA1c levels (>7.0% or <7.0%), reflecting their glycemic control. Abnormal NVC outcomes were more commonly seen in those with poor glycemic control, as the frequency of tortuosity and precapillary edema were significantly higher in patients with HbA1c levels >7.0% than those with HbA1c levels <7.0%, 29 (58%) versus 2 (16.7%) with P-value = .010 and 19 (38%) versus 0 (0%) with P-value = .012 respectively. Then the patients were divided into 2 groups after ophthalmological assessment, the first group: Diabetic patients with DR, and the second group diabetic patients with non- DR. The duration of DM in DR patients of 13 ± 5.61 years was significantly longer than 8 ± 4.65 years in non-DR patients, with P = .000. Furthermore, HbA1c was significantly higher in DR patients (9.72 ± 1.94%) than non- DR patients 8.65 ± 2.1% with P = .046. Regarding the NVC results, the frequencies of significantly increased NVC abnormalities in DR patients versus non-DR patients are shown in Table 1. The diabetic patients with detected tortuous capillaries, precapillary edema and dilated apical capillaries had significantly longer diabetes duration than those devoid of them, on further analysis, patients with DR showing most of the detected NVC abnormalities had significantly longer diabetes years duration than patients with non-DR as shown in Table 2. After further dividing the group of DR patients according to funduscopic results into 2 groups of PDR patients and NPDR patients, we compared the NVC outcomes in the 3 groups and the frequencies of NVC abnormalities are shown in Table 3. We applied multivariate regression analysis that included all the NVC pathological alterations and found out that branched capillaries and abnormal capillary width were significantly associated with DR (Table 4). Regarding diagnostic test estimates for significant NVC outcomes for DR detection, 27.8 µm capillary width discriminated patients with DR from non-DR patients (Table 5). NVC revealed abnormal capillary findings in our study as shown in Figures 1–3.
Comparison between patients with DR and non-DR patients regarding the frequencies of NVC variables using Chi-square test for qualitative variables.

Abbreviations: NVC, nail-fold capillaroscopy; DR, diabetic retinopathy.
Comparison of disease duration in diabetic patients with versus without significant NVC outcomes and comparison of disease duration in patients with DR versus non-DR patients regarding significant NVC outcomes using Chi-square test or Fisher exact tests.
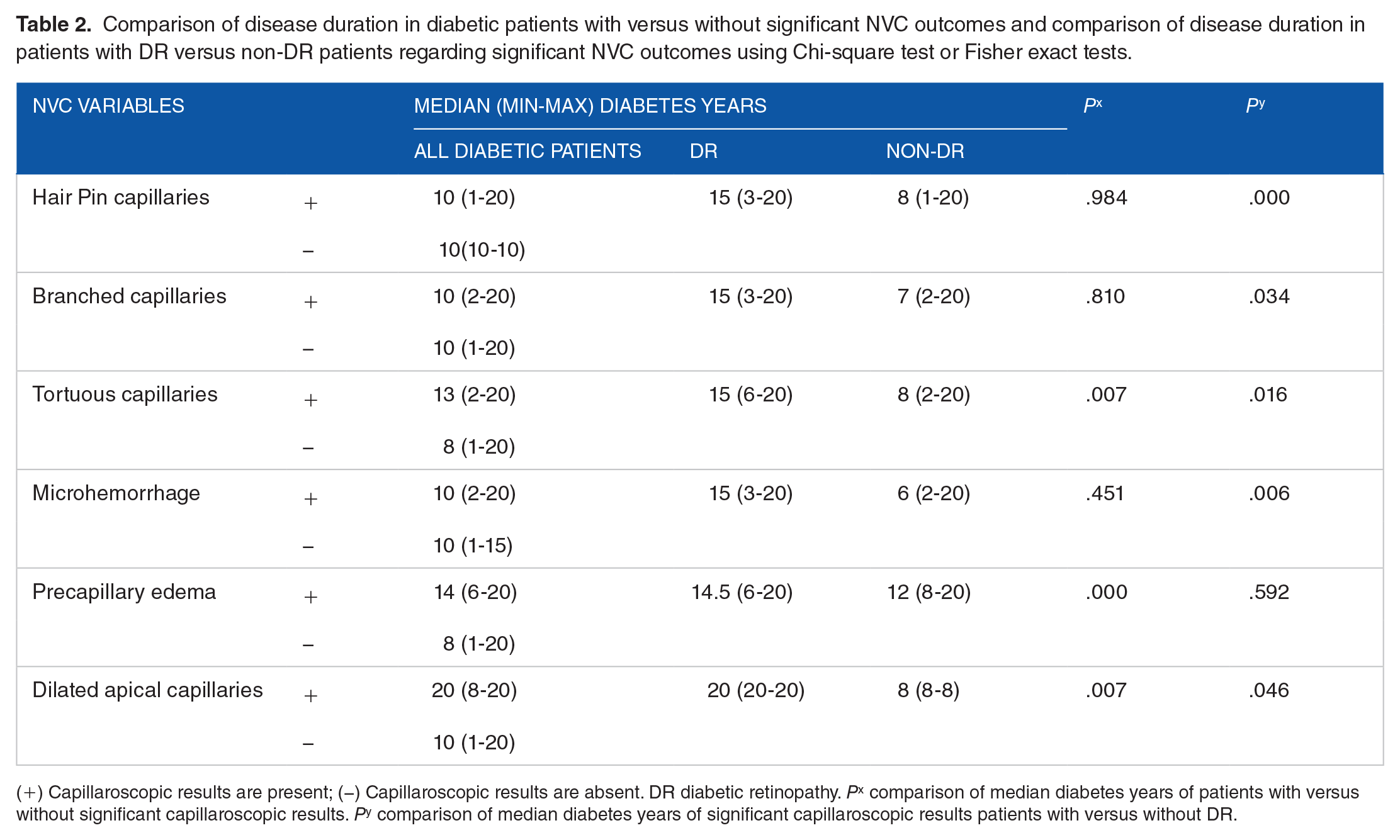
(+) Capillaroscopic results are present; (−) Capillaroscopic results are absent. DR diabetic retinopathy. Px comparison of median diabetes years of patients with versus without significant capillaroscopic results. Py comparison of median diabetes years of significant capillaroscopic results patients with versus without DR.
Comparison between patients with NPDR and patients with PDR and patients with non-DR regarding the NVC variables using Mann Whitney test for the capillary width and length and Chi-square test for qualitative variables.

Abbreviations: NPDR, non proliferative diabetic retinopathy; PDR, proliferative diabetic retinopathy.
Multivariate logistic regression analysis of significant pathological NVC outcomes to predict DR.

ROC curve analysis of capillary width for DR detection.

Abbreviations: (ROC) curve analysis: receiver operating characteristic; AUC, area under the curve; CI, confidence interval.

Tortuous capillaries.
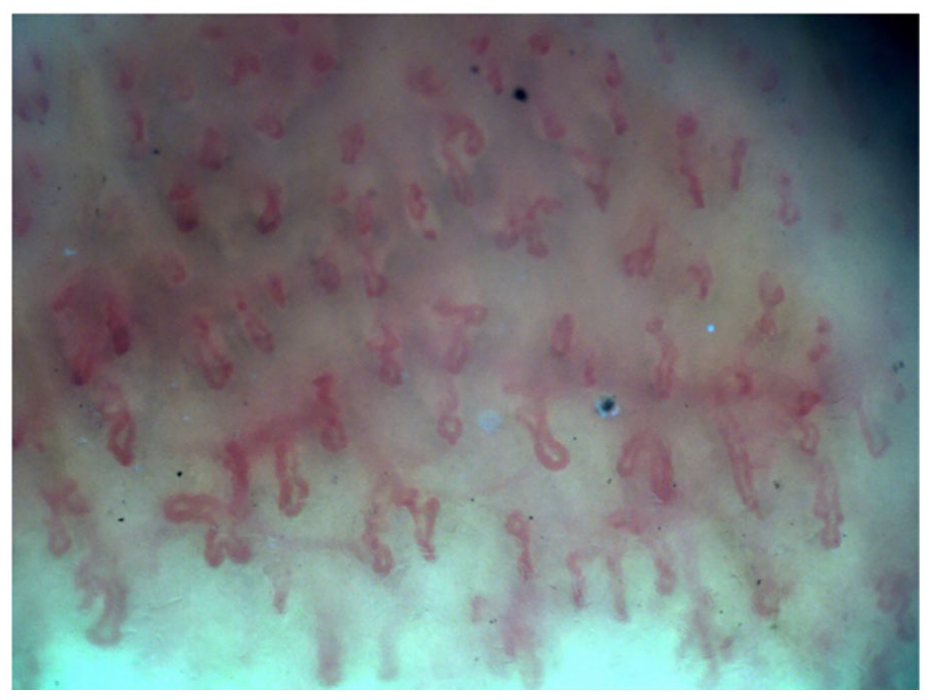
Branched capillaries with precapillary edema.
Microhemorrhages.
Discussion
There is a growing demand for a simple technique that can diagnose microvascular problems in patients with diabetes as DR. 9 NVC can be used to assess DM-related complications in the capillaries of the fingers. 20 Pathological changes include large capillaries, neogenesis, tortuous capillaries, and capillary bleeding, which can be linked to illness severity levels of mild, moderate, or severe. 4 Therefore, we aimed in our study to detect the NVC abnormalities in patients with T2DM and correlated the results with retinal microvascular complications and detected if they were related to disease duration and HbA1c.
Regarding NVC outcomes, our study demonstrated that more than 50% of all our diabetic patients had a tortuous pattern, neovascularization, and branched capillaries, microhemorrhages in the nail fold capillaries, also elongated and wider capillaries. There was a significantly longer disease duration and significantly higher HbA1c7% in patients with DR versus patients with non-DR. Also, we compared the NVC outcomes in patients with T2DM according to their HbA1c level. The results detected that the frequencies of tortuosity and precapillary edema were increased significantly in the patients with HbA1c ⩾ 7% compared to patients with HbA1c < 7%, and most of these patients were with DR. The results showed that nail fold capillary abnormalities were linked to vascular damage in patients with T2DM and poor glycemic control. We demonstrated significantly wider capillaries and significantly higher frequencies of branched, tortuous capillaries, precapillary edema, higher frequencies of microhemorrhages and dilated apical capillaries in patients with DR than patients with non-DR. These findings were consistent with the Hsu et al Uyar et al and, Rajaei et al studies which identified mega capillaries, aberrant loops, changed capillary densities, increased tortuosity and neoangiogenesis as frequent changes in patients with diabetes with a long duration and a high HbA1c.5,20,21
On the other hand, Bakirci et al and Jakhar et al stated that tortuosity, meandering capillaries, capillary dilation, microhemorrhages, and evidence of neoangiogenesis were common capillaroscopic alterations in T2DM patients. However, on comparing results between the DR patients and non-DR patients, the increased structural changes did not reach statistical significance. Jakhar et al attributed this to the smaller number of patients with DR included in their study. They also reported that the level of HbA1c could not be correlated to nail fold capillaroscopy outcomes, which is inconsistent with our study results. They stated that it could be due to HbA1c reflecting the glycemic control over 3 or 4 months, not for a long period.22,23
NVC abnormalities such as tortuosity and branching capillary were substantially greater in patients with NPDR than in patients with PDR and without DR, according to a subgroup study of DR patients to evaluate severity. Those with PDR had considerably more mega capillaries and dilated apical capillaries than patients with NPDR or no DR. These findings imply that T2DM includes a microvascular component that is linked to DR and severity, and that NVC can detect changes in the nail fold capillaries accurately. Chang et al and Maldonado et al observed cross-linked capillaries with reduced density, characteristic tortuous pattern, avascular area, and dilatations that collaborated with the diabetes abnormalities in the retina, while these changes were associated with the severity of diabetic retinopathy in Chang et al study while the researchers in Maldonado et al study made no correlation between the results and the severity of DR.24,25
According to Mohanty et al and Uyar et al patients with PDR were more likely to have poor glycemic control. Abnormal nail capillaroscopic outcomes were more frequently observed in PDR patients than in NPDR patients or people without DR.20,26 The contradictions with our data may be related to the small number of patients with PDR included in our analysis. As for diabetes years, patients with NVC abnormalities had longer disease duration than diabetic patients without these characteristics. On comparing the median diabetes years of patients with significantly present NVC abnormalities in relation to DR, we found that DR patients with abnormal nail capillaroscopic outcomes had significantly longer diabetes years than patients without DR. Chang et al and Uyar et al also noted a positive significant connection between capillaroscopic abnormalities and diabetes duration which was also significantly longer in patients with DR than patients with non-DR showing theses NVC abnormalities.20,24 Whereas Barchetta et al stated that NVC abnormalities were not related to diabetes duration. 6
Multivariate analysis was conducted to explore the predictors of DR regarding the NVC pathological outcomes and found out that branched capillaries and increased capillary width are the variants with the statistical significance regarding DR results. Upon diagnostic test estimation for DR detection, increased capillary width was the most valuable NVC finding. However, the study of Uyar et al stated the capillary tortuosity is the most valuable NVC abnormality in the regression analysis though it cannot be utilized as a diagnostic tool. 20 The main limitation remains in the small sample size; a larger sample size with more patients in all groups could have allowed us to draw more definitive conclusions.
Conclusion and Recommendations
In our study, NVC outcomes showed a higher frequency of tortuous capillaries, branched capillaries, precapillary edema, and increased capillary width together with longer disease duration and higher values of HbA1c, which influenced the development of these structural alterations in T2DM patients with DR. We assume that increased capillary width might be the most essential NVC abnormality for the detection of early DR. Because the NVC is a cost-effective, quick, safe, simple technique, and non-invasive, it is regarded as a helpful newly emerging tool to assess the capillaroscopic alterations in diabetic patients as an indicator and a severity assessment tool for DR. Further studies are needed to demonstrate the details of this issue regarding its importance for physicians and patients.