
Abstract
The ever-increasing prevalence of obesity and Type 2 diabetes has necessitated the development of newer and more effective approaches for achieving efficient glycemic control and weight loss. Conventional treatment methods often result in weight gain, further deteriorating the already impaired metabolic control in people with obesity/Type 2 diabetes. Alleviation of obesity and diabetes achieved after bariatric surgeries highlight the therapeutic importance of gut-brain axis and entails development of more patient-friendly approaches replicating the positive metabolic effects of bariatric surgery. Given the potential involvement of several gut hormones in the success of bariatric surgery, the therapeutic importance of synergistic interaction between these hormones for improved metabolism cannot be ignored. Many unimolecular multiagonist peptides are in preclinical and clinical trials as they maximize the combinatorial metabolic efficacy by concurrent activation of multiple gut hormone receptors. This review summarizes the ongoing developments of multiagonist peptides as novel therapeutic approaches against obesity-diabetes.
Keywords
Introduction
The increasing prevalence and morbidity have made diabetes one of the biggest health care challenges of the 21st century. 1 Both environmental (sedentary lifestyle, excessive calorie intake) and genetic factors contribute to this global epidemic. 2 Therefore, lifestyle and pharmacological interventions are needed for management of diabetes and delaying progression of its related metabolic comorbidities. The undesirable side effects associated with oral glucose lowering medications 3 and the progressive nature of Type 2 diabetes 4 exacerbate the need for new treatment options with improved therapeutic profile. Although incretin mimetic drugs offer a broad range of benefits by targeting multiple tissues, 5 their gastrointestinal side effects can limit clinical efficacy. In addition, the magnitude of antidiabetic efficacy demonstrated in preclinical trials has not fully translated to the clinical setting. 6 Roux-en-Y gastric bypass (RYGB) surgery is now being regarded as the gold standard technique for obesity and diabetes treatment, resulting in approximately 88% diabetes remission, subsequent weight loss, and superior metabolic control than conventional pharmacological treatments.7-9 Ongoing research highlights the key role of gut hormones in improving metabolic dysfunction post bariatric surgeries.10,11 Therefore, it is suggested that synergistic manipulation of multiple gut hormone signalling pathways may offer similar therapeutic efficacy as surgical procedures, in turn providing obvious respite across several aspects of the metabolic syndrome.
Gut Hormones Interplay Post Bariatric Surgeries
Type 2 diabetes remission following bariatric surgery is independent of weight loss and includes mechanisms such as enhanced glycemic control, 8 improved insulin sensitivity, 12 augmented pancreatic beta-cell function, 13 restored first-phase insulin secretion, 14 and decreased truncal fat deposition. 15 Altered secretion and action of gut-derived hormones such as peptide YY (PYY), glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic peptide (GIP), oxyntomodulin (OXM), cholecystokinin (CCK), and ghrelin after metabolic surgery is now being linked to Type 2 diabetes remission.11,16,17 This suggests that superior metabolic improvement post bariatric surgery is a result of interplay between gut hormones and subsequent re-programming of neuroendocrine signals. Despite these advantages, bariatric surgeries are invasive to patients, costly, and may result in complications such as kidney stones, abdominal pain, reduction of bone density, and vitamin deficiencies. 18 Thus, non-invasive and novel antidiabetic therapies that target similar peptide hormone pathways, either through individual peptide analogue administration or more interestingly via a hybrid peptide approach, have distinct therapeutic utility for Type 2 diabetes. Indeed, coadministration of different gut hormones, such as GLP-1, GIP, PYY, and CCK alone and in combination with insulin, has previously been reported to maintain normoglycemia and metabolic homeostasis in diabetes.19-22 The clinical success of combined insulin and GLP-1 therapy (IDegLira) as a single-drug formulation in Type 1 diabetes patients further point to the importance of activating multiple signal transduction pathways for improved treatment outcomes. 23
Unimolecular Poly-Agonist Approach
To combat reduced physiological concentrations of GLP-1 in Type 2 diabetes, 24 various GLP-1 mimetics are currently clinically available. 25 However, these mimetics target a single specific pathway and as such fail to achieve the superior glucose homeostasis, enhanced satiety and increased weight loss associated with bariatric surgeries, that are known to target numerous gut peptide–related cellular pathways.26,27 Therefore, strategies that can augment the antidiabetic actions of GLP-1 drugs are of key interest. In line with this, coadministration of various gut hormones with GLP-119-23 have shown therapeutic promise; however, their clinical application is often restricted due to dissimilar pharmacokinetic properties of the constituents and unwanted peptide–peptide interactions. 28 Recent years have seen remarkable progress in the development of multitargeting peptides by combining the key bioactive domains of gastrointestinal hormones into a single molecule. These multifunctional molecules exhibit a single pharmacokinetic profile together with synergistic pharmacological action (Figure 1). Owing to its well-established mechanistic pathways, most of these multiagonists have centered their structures around GLP-1.29-31 In addition, knowledge of truncated bioactive forms32-34 of gut-derived peptides has also facilitated the cost-effective generation of hybrid peptides.

This scheme demonstrates how peptide/peptide multiagonist approaches offer beneficial metabolic profile by targeting multiple receptor pathways and can be harnessed as obesity and diabetes therapeutics. CCK indicates cholecystokinin; GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like-peptide-1.
Dual-agonist peptides
GLP-1/glucagon
GLP-1/glucagon hybrid peptides have been generated to incorporate the glycemic and appetite suppressive effects of GLP-135,36 with lipolytic and thermogenic properties of glucagon.37,38 In keeping with this, various GLP-1/glucagon coagonists have been reported to normalize body weights, improve glucose tolerance, lipid profile and liver steatosis in rodents and non-human primates.39-42 Furthermore, when given in combination with PEGylated-leptin, a GLP-1/glucagon hybrid synergistically lowered body weight by restoring leptin sensitivity in diet-induced obese (DIO) mice. 43 Given their translational potential, several GLP-1/glucagon agonists with optimized pharmacokinetic profile are currently being evaluated in clinical trials. 44 A recent success story is MEDI0382, a balanced GLP-1 and glucagon receptor dual-agonist that improved glycemic control and induced significantly higher reductions of bodyweight in obese patients with Type 2 diabetes when compared to placebo group (−3.8 kg mean for MEDI0382 vs −1.7 kg mean for placebo). 45 More recently, SAR425899, another GLP-1/glucagon agonist, was reported to significantly reduce fasting glucose and HbA1c levels in patients with Type 2 diabetes. SAR425899 not only was well-tolerated but also promoted body weight reductions in healthy volunteers and in patients with Type 2 diabetes. 46 In addition, GLP-1/glucagon agonism has also shown therapeutic potential in non-alcoholic steatohepatitis and liver regeneration in preclinical research. 47 This indicates that by targeting multiorgan receptors, these peptides offer a more comprehensive beneficial profile in metabolic dysregulation.
GLP-1/GIP
Both GIP and GLP-1 are incretin hormones released postprandially to regulate blood glucose levels. 48 Type 2 diabetes patients have an inherent incretin defect arising from decreased GLP-1 secretion and reduced insulinotropic action of GIP. 49 It is primarily this reason that GIP analogues have been discounted as Type 2 diabetes therapy. 48 In addition, the discrepancies seen in preclinical genetic knockout models and in the use of GIP receptor agonism or antagonism for metabolic regulation 50 have further undermined the clinical utility of GIP analogues. In this regard, polypharmacy may help in unveiling the therapeutic potential of this rather ambiguous GIP system, as was seen previously with beneficial synergistic effects of GIP and GLP-1 coadministration. 20 Glucagon-like-peptide-1/glucose-dependent insulinotropic polypeptide hybrid peptides activate both arms of the incretin axis (hence termed as Twincretins) 28 and synergistically target the main hallmarks of metabolic syndrome including obesity, hyperglycemia, and dyslipidemia.28,51,52 Of mention is RG7697 (also known as NNC0090-2746), which was well-tolerated in Type 2 diabetes patients and displayed improved glycemic control and greater body weight reductions than placebo group.51,53 Another long-acting GIPR/GLP-1R agonist—LY3298176 (another name tirzepatide)—offers once-weekly administration and has been reported to concentration-dependently reduce HbA1c levels, body weight, fasting, and postprandial plasma glucose in Type 2 diabetes patients54,55 and has now progressed to long-term clinical safety trials. Interestingly, LY3298176 displayed a broader therapeutic window than that of a selective GLP-1 receptor agonist, as only the highest dose of LY3298176 (15 mg) showed greater gastrointestinal adverse events than dulaglutide (1.5 mg), and doses of 10 mg and less were not significantly different. 55 In addition to regulating body weight and glucose metabolism, GLP-1/GIP coagonism with a single hybrid peptide improved memory function in DIO mice 56 and displayed neuroprotective effects in animal models of brain injury, Parkinson and Alzheimer disease,57-59 further accentuating the superior metabolic profile associated with dual-receptor activation. Taken together, the strategy of harnessing synergistic antidiabetic effects of both arms of the incretin axis would help to sustain metabolic control by mimicking the native physiological incretin response.
GLP-1/CCK
CCK is an anorexigenic hormone secreted from enteroendocrine I-cells. 60 CCK-8 is the major circulating form in plasma and inhibits food intake by binding to CCK-A receptors. 60 In addition, benefits of GLP-1 at the level of the beta-cell have been suggested to be linked to a GLP-1/CCK intraislet loop. 61 The combined treatment of CCK with GLP-1 analogues in rodent models significantly lowered circulating glucose levels, improved glucose tolerance, and induced greater weight loss and appetite suppressive effects when compared with individual treatments.62,63 In keeping with such evidence of synergistic metabolic actions, the potential of a novel hybrid peptide that incorporates the key bioactive regions of (pGlu-Gln)-CCK-8 and exendin-4 was investigated. 31 By simultaneous activation of both GLP-1 and CCK-A receptors, this coagonist outperformed exendin-4 in terms of satiety and body weight reductions in DIO mice. 31 Other beneficial effects of (pGluGln)-CCK-8/exendin-4 included prominent glucose homeostasis and reduced HbA1c and triglyceride levels, as well as improvements of insulin action and glucose disposal. 31 In a recent study by Hornigold et al, 64 another hybrid peptide, named C2816 generated by combining stabilized GLP-1R agonist (AC3174) and a CCK-AR-selective agonist (AC170222), exhibited superior weight reductions when compared with combined administration of the parent peptides in DIO mice. Although these initial observations clearly highlight the synergistic metabolic benefits of unimolecular approach, further preclinical studies are necessary for comprehensive functional characterization of these GLP-1/CCK coagonists, particularly the combined effects of GLP-1 and CCK on the gallbladder would need to be carefully evaluated. 65
GLP-1/gastrin
Gastrin, a CCK homologous peptide, is secreted from gastric G-cells and binds to CCK-B receptors, with a potential role in beta-cell regeneration. 66 Coadministration of gastrin and GLP-1 resulted in improved beta-cell mass and survival in non-obese diabetic mice, 67 paving way for a GLP-1 and CCK-B receptor dual-agonist, ZP3022. 68 ZP3022 reduced body weight, improved glucose tolerance, and increased beta-cell mass in db/db mice and Zucker diabetic fatty (ZDF) rats.68,69 While further studies are necessary to harness its potential as an antidiabetic pharmacotherapy, initial observations are encouraging.
GLP-1/xenin or GIP/xenin
Xenin is a 25-amino acid peptide hormone secreted into the bloodstream from the intestinal K-cells in response to food intake. 70 Given the reduced insulinotropic effect of GIP, xenin is of key therapeutic significance for potentially overcoming GIP resistance in Type 2 diabetes patients.71,72 Indeed, glycemic normalization has been shown to restore GIP insulin-secretory function in Type 2 diabetes.73,74 GLP-1/xenin and GIP/xenin hybrids were generated by incorporating the key amino acid sequences of exendin-4 or (DAla)2 GIP with xenin-8-Gln,75,76 where xenin-8-Gln represents a stabilized fragment peptide of xenin that recapitulates the major biological functions of the parent peptide. 77 Subchronic treatment with both xenin-based hybrid peptides displayed robust insulin secretory activity, improved glucose homeostasis, insulin sensitivity, and glucose tolerance in DIO mice.75,76 Notably, both hybrids augmented the biological response to native GIP in line with xenin’s GIP potentiating capabilities.75,76 Together with efficient glucose homeostasis, the superior efficacy of both hybrids was also evident from the improved lipid profile 75 and preserved pancreatic islet architecture. 76 It is suggested that xenin-mediated effects occur via activation of neuronal signalling 69 ; therefore, further studies are still required to disentangle the contribution of individual components of gut-brain axis for these observed metabolic effects. Although both activation and inhibition of GIP is postulated as a possible treatment option for Type 2 diabetes and obesity,50,78-81 it is suggested from these studies that novel treatment options aimed at overcoming GIP resistance in Type 2 diabetes may have therapeutic potential.
GLP-1/amylin
The GLP-1/amylin hybrid peptide was engineered to combine the pronounced antidiabetic therapeutic capacity of GLP-1 mimetic-exendin-4, 82 with the satiety and weight-lowering properties of stable amylin analogue, davalintide, 83 within a single compound. These coagonists exhibited similar glycemic control as exenatide-treated group; however, their effects on body weight lowering were superior to exenatide or davalintide monotherapies in ob/ob mice and DIO rats. 84 In a separate study, a PEGylated version of this hybrid with extended in vivo half-life showed enhanced glucose lowering and weight loss in rodents. 85
Multiagonist peptides
The preclinical and clinical success of coagonist peptides discussed above has led to the development of novel triple-acting hybrids to achieve sustained metabolic improvements. One such example is GLP-1/Glucagon/GIP tri-agonists, where the main rationale was to incorporate the glucose lowering, insulinotropic, weight lowering and appetite suppressive effects of incretins with beneficial effects of glucagon on energy expenditure and lipid metabolism.37,38,48 The sequence similarities between the glucagon family of peptides and receptors 86 led to development of triple agonist peptides, namely YAG/glucagon, [DAla2]GIP/Oxm, and [DAla2]GLP-1/glucagon hybrids.30,87,88 Using receptor transfected cells, receptor antagonists, and incretin receptor knockout mice, all 3 hybrids were reported to activate GLP-1, GIP, and glucagon-signalling pathways.30,87,88 Subchronic treatment with all 3 hybrid peptides displayed glucose lowering, improved glucose tolerance, and insulinotropic effects in DIO mice,30,87,88 but only [DAla2]GIP/Oxm and [DAla2]GLP-1/glucagon hybrids caused body weight reduction. [DAla2]GLP-1/glucagon also improved insulin sensitivity in DIO mice. 87
Similarly, another novel GLP-1/GIP/Glucagon hybrid was engineered based on the antidiabetic benefits of a previously validated GLP-1R/GIPR coagonist 28 together with the notable metabolic advantages evoked through incorporation of a glucagon component. This triple-acting peptide retained balanced GLP-1, GIP, and glucagon receptor activity in rodent beta-cells, adipocytes, and hepatocytes, respectively, suggesting simultaneous multiorgan receptor agonism. 29 Although clear reductions in body weight and hepatic steatosis were evident in DIO mice, this was not the case in lean mice, implicating that tri-agonist exerts benefits only when coupled with metabolic dysregulation. 29 Treatment with GLP-1/GIP/Glucagon triagonist also reduced pancreatic alpha-cell invasion to the islet core, thereby preserving the islet cyto-architecture in ZDF rats and db/db mice. 29 Notably, every other day treatment of HM15211, a long-acting tri-agonist peptide conjugated to the human aglycosylate Fc fragment, reduced body weight and glycemia and was more effective than daily administration of liraglutide in increasing energy expenditure in rodent models. 89 Meanwhile, HM15211 and another triagonist, MAR423, have now entered phase 1 clinical trials.
To overcome the inherent GIP resistance in Type 2 diabetes condition, a triple agonist peptide was engineered by combining a previously characterized exendin-4/gastrin dual-agonist 68 with xenin-8-Gln. Twice daily administration of exendin-4/gastrin/xenin-8-Gln decreased circulating glucose, increased plasma insulin, reduced body fat mass, and improved glucose tolerance, insulin sensitivity, lipid profile, and metabolic response to GIP in DIO mice. 90 Moreover, a stable and long-acting fatty acid-derivatized form, namely exendin-4/gastrin/xenin-8-Gln-Lys 27 PAL, was developed to extend its bioactive profile for up to 12 hours; however, the fatty acid acylation did not impart any additional therapeutic benefits as first hoped for. 91
Taken together, the use of multitargeting hybrid peptides that incorporate a GLP-1 backbone structure, linked to the bioactive region(s) of various other regulatory hormones, have shown remarkable therapeutic efficacy and offer viable alternative to bariatric surgery. In addition, given the nexus of PYY in diabetes remission post bariatric surgeries 92 and the success of PYY, GLP-1, and/or OXM coadministration,12,93 PYY/GLP-1-based coagonists may also be evaluated as a potent non-surgical therapy for diabetes and obesity.
Although these preclinical studies highlight the efficacy of multiagonist peptides, there is often insufficient evidence as to whether the purported efficacy is being fractionally contributed by more than one component. Therefore, a major requirement for preclinical studies is to scrutinize balanced activity at individual key receptors, necessary for quantifying selective agonism and averting any off-target adverse events. In addition, the animal studies cannot capture the heterogeneity of human disease and such safety is difficult to predict and must be established in large, diverse chronic human studies. Indeed, despite their pharmacological benefits, the reports of pancreatitis and thyroid cancer post incretin mimetic treatments have raised safety concerns for their clinical use.94,95 The US Food and Drug Administration (FDA) and European Medicines Agency (EMA) have since independently reviewed several clinical safety databases, pancreatic toxicology studies, and cardiovascular outcome trials, and both agencies continue to investigate the pancreatic safety associated with incretin-based drugs; however, in light of the current knowledge, these concerns have now been allayed.96,97 Therefore, an appropriate balance between potency and long-term safety must be established in clinical trials, before these multiaction peptides can be seriously considered as registered antidiabetic drugs.
Future Directions
Single-molecule drugs targeting 2 or more gut-derived peptide hormone receptors have shown tremendous therapeutic potential, but the macromolecular nature of these drugs raises the concerns of immunogenicity. 98 Therefore, more extensive preclinical assessment of these unimolecular multiagonists is essential to establish their translational efficiency to clinical settings. While animal studies are indispensable for optimizing novel drug candidates and to ascertain their human translational potential, there have been several incidences where drugs with promising preclinical data have failed in clinical trials, 99 hence a cautious interpretation of preclinical studies is required to ensure bench-to-bedside translation. A major challenge for translation of hybrid peptides from animal models to humans is the associated risk of cross-reactivity with other receptors leading to off-target effects. 98 In this regard, receptor affinity studies in different aetiologies of diabetes are required to decipher the complete metabolic efficacy and safety profile of these multitargeting hybrid peptides. Although various chemical modifications are being used to increase receptor binding, specificity, solubility, and protracted action, further chemical optimizations are still needed to achieve a more desirable pharmacokinetic and pharmacodynamic profile of these multiacting peptides. Mechanistic and receptor balance studies are necessary to help fine tune the most potent synergistic effects in vivo. Despite these cautions, the concurrent activation of multiple receptors by single-molecular entities has shown superior or equivalent efficacy compared to single-peptide agonists (Table 1); however, species-specific receptor affinity and chronic safety need to be carefully evaluated before considering this multiple-targeting peptide strategy a viable therapeutic option for Type 2 diabetes.
Summary of multireceptor agonists currently in preclinical and clinical trials and their effect on metabolic regulation.
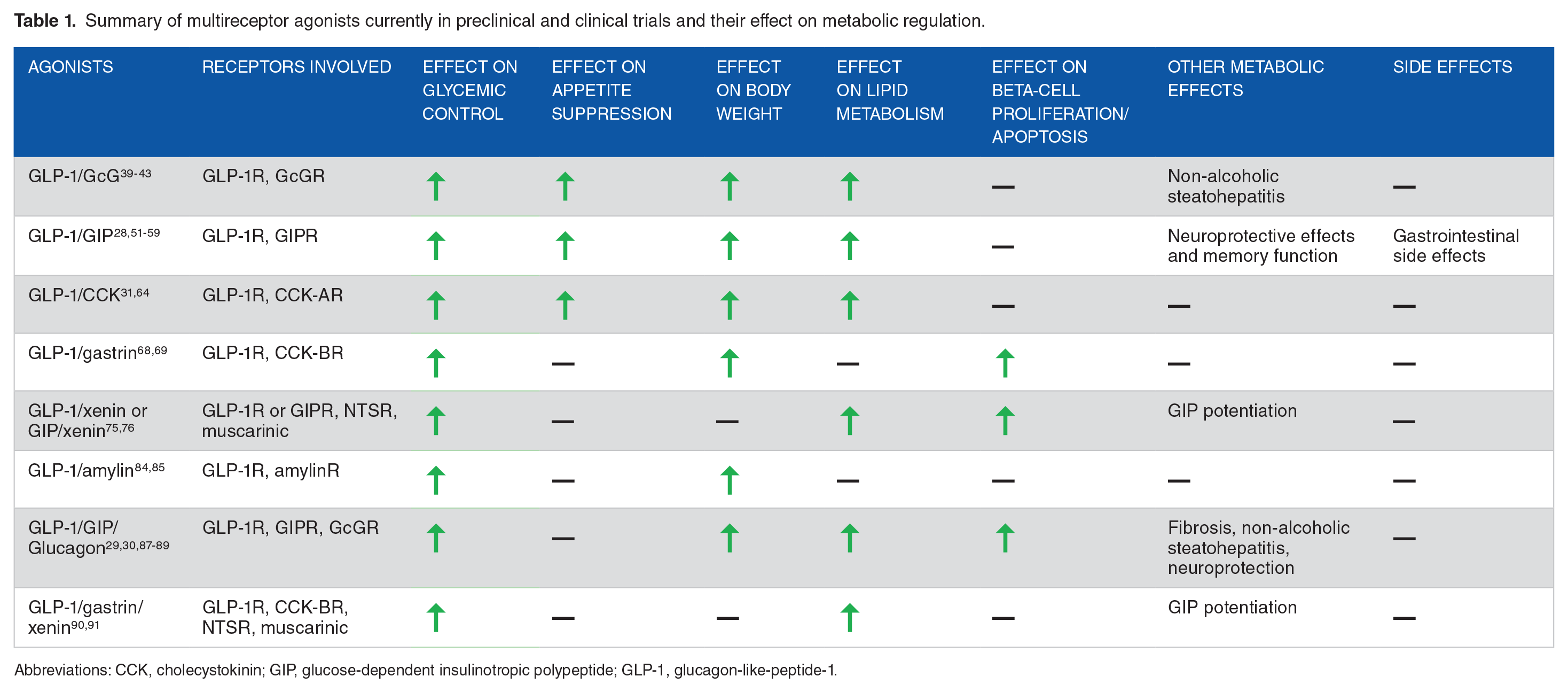
Abbreviations: CCK, cholecystokinin; GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like-peptide-1.
Conclusion
The importance of combined actions of various regulatory peptide hormones for control of metabolism is slowly beginning to come to light, particularly given recent knowledge gained from certain types of bariatric surgeries. While unimolecular peptide approach seems to offer superior therapeutic efficacy, possibly reduced adverse effects, low dosage regimen when compared to individual peptide analogue administration, is patient friendly and may overcome the difficulties associated with solubility and dosage formulation of a mixture of 2 or more peptides when administered by single injection. However, careful outpatient clinical studies are still required to determine the sustainability, safety, and translational potential of these multiagonist drugs as novel class of antidiabetic and antiobesity medications. Nevertheless, regulation of energy balance is a complex process involving multiple central and systemic tissues, and these unimolecular peptides may offer a more patient-centric non-surgical breakthrough for the treatment of obesity-linked metabolic disorders.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AH: developed the structure of paper, wrote the manuscript, reviewed and approved the final manuscript.