
Abstract
Background:
Antihypertensive drug therapies have been reported to be associated with new onset of type 2 diabetes mellitus in some hypertensive patients after prolonged use. Angiotensin converting enzyme (ACE) gene has been found to affect essential hypertension, response of antihypertensive therapies, and glycemic disturbances. Therefore, ACE gene I/D polymorphism may be associated with risk of new onset of type 2 diabetes via metabolic disturbances, glycemic dysregulation, and insulin resistance.
Aim:
To assess the correlation between ACE gene I/D polymorphism and glycemic disturbance under influence of diuretic and other antihypertensive drug therapies.
Materials and methods:
We recruited 270 normotensive patients as control (150 men and 120 women), 270 hypertensive patients (95 men and 175 women), and 240 hypertensive with new onset of diabetes patients (80 men and 160 women). All samples were genotyped for ACE gene polymorphic alleles and relationship between different genotypes and anthropometric and clinical parameters along with drug therapies was established and analyzed.
Results:
Baseline clinical (systolic blood pressure, diastolic blood pressure, and fasting blood glucose level) and anthropometric parameters (height, weight, waist circumference, hip circumference, waist-hip ratio, and body mass index) of study populations were found highly statistically significant (P < .05) when compared among study groups. Furthermore, genotype wise comparison of all these parameters in essential hypertensive (EH) and essential hypertensive with onset of diabetes (EHNOD) patients found most of them nonsignificant and no variation was found with respect to different genotypes of ACE gene. The genotype wise comparison of clinical parameters among different antihypertensive drug therapy was found statistically nonsignificant in both EH and EHNOD patients.
Discussion:
Anthropometric parameters can be taken as the risk indicator factors for hypertension and diabetes. However, ACE gene polymorphism may not be a risk factor for development of diabetes in hypertensive patients.
Conclusion:
The present study suggested that ACE gene polymorphism did not show any significant association with the risk of new onset of diabetes in EH patients and more detailed studies with large population size are needed.

Keywords
Introduction
Essential hypertension and diabetes are among such lifestyle diseases which are the leading causes of premature deaths around the globe, due to their cardiovascular and kidney disease complications, if remains untreated. 1 These 2 interrelated diseases are spreading at a fast pace with the change in the lifestyle pattern. One disease increases the probability of the other disease in same patient. Hypertension is an independent risk factor for cardiovascular complications including coronary heart disease, angina pectoris, stroke, ischemia, and atherosclerosis and it is linked with cardiovascular morbidity and mortality.2,3 Hypertension and diabetes are associated comorbid diseases which share common metabolic pathways such as obesity, insulin resistance, oxidative stress, inflammation, and genetics. 4 An estimate of World Health Organization (WHO) revealed that around 9.4 million of deaths occur per year because of hypertension alone. 5 The Joint National Committee VIII guidelines suggested the first line drug therapy for the treatment of hypertension as angiotensin converting enzyme inhibitors (ACE inhibitors), diuretics, beta blockers (BBs), calcium channel blockers (CCBs), and angiotensin receptor blockers (ARBs). 6 But these first line antihypertensive drug therapies were reported, by different studies, as the risk factor of new onset of type 2 diabetes mellitus in some hypertensive patients on prolonged use.7–11 It was found that the use of antihypertensive medications for 3 to 6 years or more either as a monotherapy or as combination therapy may induce new onset of diabetes in 18% to 25% of patients.12,13 Antihypertensive drugs mainly diuretics, BBs, and ACE inhibitors have been found to be associated with glycemic dysregulation via increasing insulin insensitivity or insulin resistance.14,15 However, many other studies also presented preventive effect of ACE inhibitors on type 2 diabetes reducing the chance of developing diabetes by 15% to 30%.16–18 The metabolic disturbances (glucose turnover) associated with salt sensitivity and insulin resistance under the influence of genes polymorphism may be affected by different antihypertensive drugs such as ACE inhibitors, diuretics, and BBs and induce new onset of diabetes in hypertensive patients. 19
Many candidate genes have been identified which may be involved in insulin insensitivity and insulin resistance which may further be associated with type 2 diabetes mellitus.20,21 Angiotensin converting enzyme is an enzyme of RAAS (renin-angiotensin-aldosterone) which is the key factor in regulating blood pressure and volume homeostasis. Angiotensin converting enzyme gene I/D polymorphism has been found to affect hypertension and the response of antihypertensive therapies. The II allele of ACE gene was found to be linked with higher reduction in mean arterial pressure as compared with DD genotype when patient was treated with diuretics. 22 The diabetic patients with DD genotype was found to be glucose intolerant as compared with other genotypes. 23 The metabolic disturbances have been found linked with elevated ACE level in the blood. The D genotype of ACE I/D polymorphism was found to be linked with higher ACE level which further leads to increased angiotensin II level and metabolic disturbance. These metabolic disturbances may be responsible for disturbed glucose homeostasis after antihypertensive treatment leading to insulin resistance and ultimately diabetes.24–26 Also D allele of ACE gene I/D polymorphism is associated with insulin resistance in hypertensive families which may be associated with glucose dysregulation and NOD. 27 Expression of different alleles of ACE gene affects antihypertensive drug’s physiological response by varying ACE activity. Higher ACE level is associated with insulin resistance and metabolic disturbances. These genotypes-based physiological disturbances influence the outcome of antihypertensive therapy and may result in adverse events like glucose intolerance or glucose dysregulation. Therefore, in the present study, we attempted to access the role of IRS-1 gene polymorphism in antihypertensive therapy induced new onset of diabetes.
Material and Methods
Methods
Ethics
The study was approved (IEC/670) by the Institutional Ethics Committee of M. M. University and written consent was obtained from all the participants.
Study design and sample size
The study was carried out on the basis of cross-sectional survey by M. M. Institute of Medical Science & Research, Mullana (Haryana); there are around 38 500 inhabitants residing in 17 villages of this rural area. The survey recorded a total of 2672 individuals afflicted with essential hypertension. These patients will be referred to as hypertensive with a disease prevalence of 6.94%. Out of 2672 patients, we have selected 510 patients who visited regularly in hospital OPD. A sample size of 164 patients will be sufficient to represent the hypertensive population residing in the rural area under investigation with a power of 80% and a P value of .05. Patients who agree to participate were explained the nature and the objectives of the study, and informed consent was obtained individually. The information about patient’s identity was not included with other data and only consulting physician had the access to this information.
Study population
In the present investigation, the subjects under study (n = 510) were divided into 2 groups with age and sex matched: (1) essential hypertensive (EH) and (2) essential hypertensive with onset of diabetes (EHNOD). The first group comprised 270 hypertensive patients (95 men and 175 women). The second group consisted of 240 hypertensive with diabetes patients, out of which 80 were men and 160 were women. To make a comparison with normal individuals, we have selected age and sex matched normal individuals from the same place and denoted as normotensive group. This third group had 270 normotensive patients (150 men and 120 women). Various parameters like age, sex, body mass index (BMI), blood pressure, education, and family history were recorded in a given questionnaire. The information about patient’s identity was not included with other data and only physician had the access to this information.
Inclusion criteria
Patients residing in rural area of Haryana for more than 2 generations were recruited. They were the age of 18 to 75 years with an average blood pressure limits >140 mm Hg systolic blood pressure (SBP) and >90 mm Hg diastolic blood pressure (DBP) on 3 separate occasions.
For EH group: Only those patients who had essential hypertension and were treated with selective antihypertensive medication (diuretics, BBs, CCBs) for about 3 years or more than that in monotherapy or combination therapy.
For EHNOD group: Only those patients who had EH (as per above criteria) with onset of diabetes mellitus (diagnosed according to WHO criteria as either a fasting plasma glucose >7.0 mmol/L and/or random [nonfasting] blood glucose > 11.1 mmol/L) and were treated with selective antihypertensive medication (diuretics, BBs, CCBs) for about 3 years or more in monotherapy and combination therapy.
Normotensives (NT): Those who were residing in rural area of Haryana without any history of hypertension or diabetes between the ages of 18 to 75 years.
Exclusion criteria
All individuals with the age less than 18 years or above 75 years were excluded. Essential hypertensive patients, who are taking drugs for other than diuretics, BBs, and CCBs alone or in combination, were also excluded. Pregnant and lactating mothers were excluded from the study.
Genotyping for ACE gene
Blood samples were collected28–29 from all the study group individuals and DNA was isolated by the standard modified inorganic method as described by Miller et al, 30 and quantified following standard spectrophotometric analysis. The isolated DNA samples were stored at −20°C till further analysis. Angiotensin converting enzyme gene I/D polymorphism (Gene bank accession number GQ449380, GQ449383) was first identified by Rigat et al. 31 Polymorphism in intron 16 of ACE gene positioned on chromosome at 17th position causes I/D polymorphism due to 287 bp Alu sequence. Presence of the 287 bp Alu sequence is termed as insertion (I allele) while absence is deletion (D allele). It forms 3 genotypes, that is, DD homozygous, II homozygous, and ID heterozygous resulting in inter individual variations in plasma ACE level which is further related to variations in other physiological parameters.25,31 The ACE gene I/D polymorphism is detected by polymerase chain reaction by primer flanking of 287 bp Alu sequence using ACE gene primer pairs as used in previous studies.29,31 After initial amplification, all samples were identified as DD genotype which was reconfirmed by amplifying again using insertion specific forward primer.
The polymerase chain reaction was carried out in thermal cycler (Bio-Rad, Japan) in total volume of 25 µL in 0.2 mL PCR tubes containing 2 µL (40 ng) of template DNA, 5.5 µL master mix (containing Taq polymerase, loading dye, dNTPs, MgCl2, and buffer 10X), 1 μL (forward primer and reverse primer), and 16.5 μL nuclease free water. Initial denaturation was carried out at 94°C for 3 minutes followed by 35 amplification cycles at 94°C for 30 seconds, primer annealing at 58°C for 20 seconds, initial extension at 72°C for 20°seconds and final extension step at 72°C for 3 minutes. The amplified segment of the gene was resolved on 0.8% agarose gel using gel electrophoresis process and visualized under UV photo documentation. Appearance of 490 bp band was identified as DD genotype, 190 bp bands as II genotype, and appearance of both bands (490 bp as well as 190 bp) was identified as ID genotype. 29
Statistical analysis
Data analysis was done with the help of an SPSS version 14.5. Continuous variables are expressed as means ± SD. Intergroup comparisons are made using students t test. Allele frequencies were calculated from genotype frequencies and were compared using chi-square (χ2) statistics. P value ⩽ .05 was considered statistically significant.
Results
Study population and baseline characteristics
A total of 270 EH patients and 240 EHNOD patients treated with antihypertensive therapy were included in the study. Female patients were more in number than male patients in both the groups. Out of 270 EH patients, 175 were women and 95 were men; in the case of EHNOD, there were 160 women and 80 men.
As per baseline parameters (Table 1), the study groups were statistically significantly different with respect to various anthropometric and clinical parameters. Age was extremely significant between normotensive and EHNOD patients at p2 and p4 values. The SBP and DBP were statistically higher significant at all P values. The average fasting blood glucose (FBG) levels were 207.29 ± 81.02 mg/dL in EHNOD and 107.20 ± 7.85 mg/dL in EH. It was statistically higher significant in all P values. All other anthropometric parameters such as BMI, waist circumference (WC), waist-hip ratio (W/H), and hip circumference (HC) showed higher statistical significance (P < .0001) between all the groups except height. The average duration of hypertension in both the groups (EH and EHNOD) was 4.70 ± 4.11 and 7.91 ± 4.52 years, respectively, and total duration of diabetes after treatment of antihypertensive therapy was 5.72 ± 4.32 years in EHNOD patients.
Comparison of baseline parameters of different groups in overall population.

Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; EH: essential hypertension; EHNOD, essential hypertensive with onset of diabetes; FBG, fasting blood glucose; HC, hip circumference; HTN, hypertension; p1, normal vs EH; p2, normal vs EHNOD; p3, EH vs EHNOD; p4, normal vs EH vs EHNOD; SBP, systolic blood pressure; WC, waist circumference; W/H, waist-hip.
The gel picture (Figure 1) represented the different genotypes of ACE gene. Table 5 represented genotype and the allelic distribution of EH vs normotensive group.
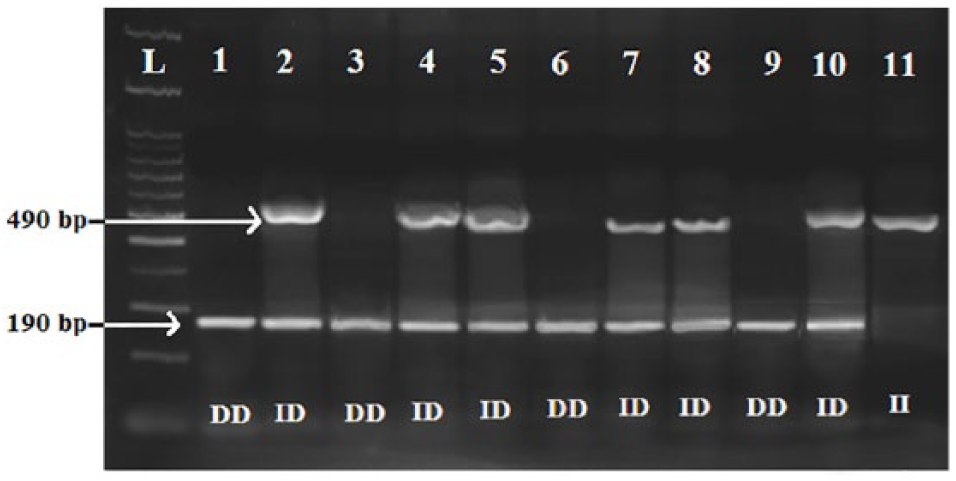
An agarose gel photo plate of PCR product representing the amplification of ACE I/D polymorphism. Lane L represents the 100 bp DNA ladder for band comparison. Lanes 1, 3, 6, and 9 represented homozygous DD genotype; lanes 2, 4, 5, 7, 8, and 10 represented heterozygous ID genotype; and lane 11 represented homozygous II genotype. ACE indicates angiotensin converting enzyme.
The percentage frequency of ID heterozygote was higher followed by DD and then II genotypes in both the groups (EH and NT). All frequencies were in Hardy-Weinberg equilibrium but statistically nonsignificant for patients and control. Frequency of D allele was 0.520 and that of I allele was 0.480 of EH group. Similarly for EHNOD patients, it was statistically nonsignificant. The frequency of D allele was 0.377 and I allele was 0.623 in EHNOD whereas in normotensive group, the D allele was 0.519 and I allele was 0.481 (Table 2).
Distribution of allelic and genotypic frequencies of ACE I/D polymorphism among overall populations of EH and EHNOD patients compared with normotensive individuals.

Abbreviations: ACE, angiotensin converting enzyme; EH: essential hypertension; EHNOD, essential hypertensive with onset of diabetes. χ2 based on allele frequency (df = 2), EH vs normotensive = 0.600, P = .740, and EHNOD vs normotensive = 11.72; P = .002.
Table 3 represented the distribution of different genotypes of ACE gene with respect to various clinical and anthropometric parameters of overall EH patients.
Comparison of various baseline anthropometric and clinical parameters in overall population of EH patients among different genotypes of ACE gene I/D polymorphism.

Abbreviations: ACE, angiotensin converting enzyme; BMI, body mass index; DBP, diastolic blood pressure; EH: essential hypertension; FBG, fasting blood glucose; HC, hip circumference; p1, DD vs ID; p2, DD vs II; p3, ID vs II; p4, DD vs ID vs II; SBP, systolic blood pressure; WC, waist circumference; W/H, waist-hip.
In overall EH patients, various anthropometric and clinical parameters were compared among different genotypes of ACE gene to evaluate the effects of different genotypes on these parameters. The mean values of given baseline parameters were almost similar in all genotypes and were statistically nonsignificant. The mean value of duration of EH was slightly higher in DD genotype as compared with ID and II genotypes but it was statistically nonsignificant for all P values. Therefore, these parameters were compared sex-wise in male and female populations of EH patients separately and similar results were obtained.
In overall population of EHNOD patients, the genotype-wise comparison revealed that the mean values of all parameters were almost similar among the different genotypes and were statistically nonsignificant. Although a higher mean value of FBG level in ID genotype was observed as compared with DD and II genotypes, it was statistically nonsignificant. However, the mean value of height was significantly higher in DD and ID genotypes as compared with II genotype (p3 = 0.0231 and p4 = 0.0442). Similarly, the mean value of W/H ratio parameter was significantly higher in II genotype as compared with DD and ID genotypes when compared in ID vs II genotypes (p3 = 0.0093) and in DD vs ID vs II genotypes (p4 = 0.0224). The mean values of duration of EH and duration of diabetes were almost similar and it was statistical nonsignificant for all P values (Table 4).
Comparison of various baseline anthropometric and clinical parameters in overall population of EHNOD patients among different genotypes of ACE gene I/D polymorphism.
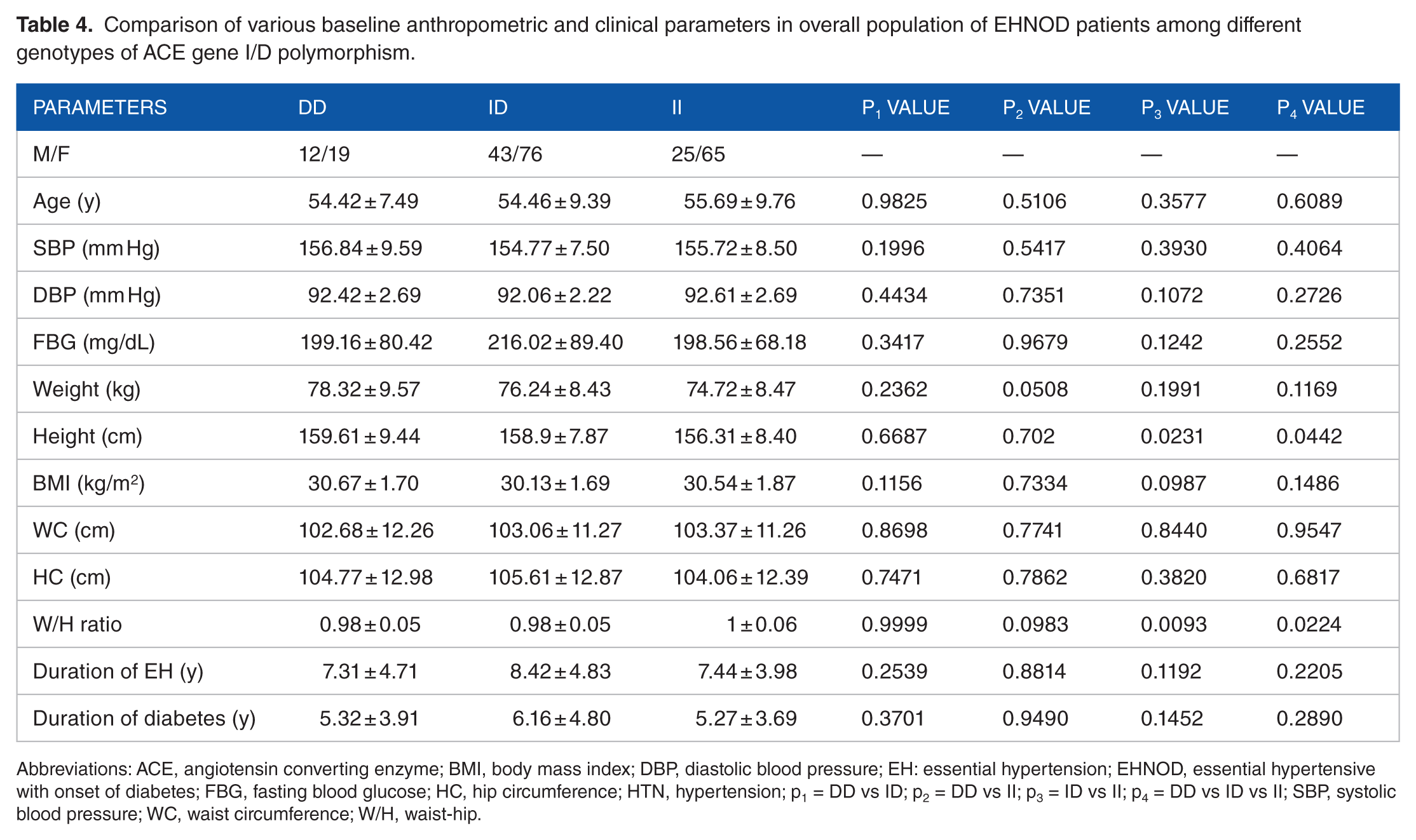
Abbreviations: ACE, angiotensin converting enzyme; BMI, body mass index; DBP, diastolic blood pressure; EH: essential hypertension; EHNOD, essential hypertensive with onset of diabetes; FBG, fasting blood glucose; HC, hip circumference; HTN, hypertension; p1 = DD vs ID; p2 = DD vs II; p3 = ID vs II; p4 = DD vs ID vs II; SBP, systolic blood pressure; WC, waist circumference; W/H, waist-hip.
Similarly, data were studied for male and female populations separately (data not shown) and no significant difference was observed in clinical and anthropometric parameters among different genotypes.
Table 5 represented the genotype distribution with respect to drug therapy in male and female population of EH patients. In male population, the difference in mean value of DBP was statistically significant (P = .0216) but the mean values of SBP and FBG level were nonsignificant at baseline readings among 3 genotypes. After 1 year of the antihypertensive treatment, the mean values of SBP, DBP, and FBG among different genotypes of ACE gene were statistically nonsignificant with all drug therapies (either as monotherapy or combination therapy). In case of blood pressure, more reduction in mean values of SBP and DBP from the baseline values was observed with combination therapy as compared with monotherapy. In monotherapy, diuretics and CCBs were more effective than BBs. The FBG level was found somewhat elevated and within prediabetic range in ID genotype as compared with DD and II genotypes with BBs and diuretics therapy but it was nonsignificant. In the female population of EH patients, same trend was followed as that of men.
Distribution of genotypes with respect to various parameters in men and women of essential hypertensive patients before and after drug treatment.

Abbreviations: BB, beta blocker; CCB, calcium channel blocker; DBP, diastolic blood pressure; FBG, fasting blood glucose; SBP, systolic blood pressure.
Similarly, in male and female populations of EHNOD patients (data not shown), the mean values of SBP, DBP, and FBG level were statistically nonsignificant among different genotypes of ACE gene. After 1 year of drug therapy, the effect of BBs monotherapy could not be evaluated due to lack of sufficient number of patients in different genotypes. Among other drugs, CCBs were more effective in controlling SBP and DBP than diuretics. FBG level was slightly higher in II genotypes with diuretic therapy but was statistically nonsignificant.
The average change in the FBG level in EH patients (Figure 2A) after treatment with different antihypertensive drugs as compared with initial readings revealed that a combination of diuretics with CCBs showed maximum fall FBG level in II genotype as compared with DD and ID genotypes whereas with the combination of BB with diuretics and monotherapy of CCBs, the average fall in FBG level was observed in DD genotype but in II and ID genotypes almost equal effect was shown. All drug therapies were also showing preventive action on FBG level; however, monotherapies of BBs and diuretics were less preventive in case of FBG level. No rise in the FBG level was observed with any drug therapy in any genotype. Similarly, the average change in FBG level in EHNOD patients (Figure 2B) shows almost equal reduction in FBG level in all genotypes with all drug therapies. But BBs and CCBs as monotherapy were less effective in DD genotype than II and ID genotypes.

(A) Average change in fasting blood glucose level in EH patients among different genotypes after different antihypertensive therapies treatment after 1 year. (B) Average change in fasting blood glucose level in EHNOD patients among different genotypes after different antihypertensive therapies treatment after 1 year. BB indicates beta blocker; CCB, calcium channel blocker; FBG, fasting blood glucose; EH: essential hypertension; EHNOD, essential hypertensive with onset of diabetes.
Discussion
The present study aimed to evaluate the genotypic association of polymorphic alleles of ACE gene with antihypertensive therapy induced new onset of diabetes in EH patients in rural population of Haryana. Previous studies reported around 40% prevalence of EH in the given population32,33 which indicated that suitable number of patients were available in this area to conduct the present study. The baseline parameters (clinical and anthropometric) mutually compared among normotensive, EH, and EHNOD patients (Table 1) showed a higher statistical significance (P < .0001) in all p values (p1, p2, p3, and p4) for different anthropometric parameters showing these parameters as the indicative of risk factors for EH in both EH and EHNOD groups when compared with normal population. However, age and height were not significant for all comparisons and could not be taken as the indicator of risk factor for EH. A higher D allele frequency than I allele among EH patients and normotensive individuals were observed similar to the previous studies in Sikhs 34 and South Indian population35,36; however, some studies reported opposite results showing higher I allele frequency in Haryana, Himachal Pradesh, Uttaranchal, and Assam. 34 The ID genotype was found most frequent than DD and II genotypes which is similar to previous studies that included North Indian,29,34 South Indian, 37 and East Indian 38 populations. However among EHNOD patients, our study reported statistically significant (P = .002) higher frequency of I allele than D allele in comparison with normotensive individuals. Similar results were reported in the previous study by Vamsi et al 39 suggesting higher frequency of I allele and identified it as the risk factor for EH and diabetes. A statistically nonsignificant variation in the different baseline anthropometric and clinical parameters was observed in both EH and EHNOD patients (Table 3) when compared among different genotypes of ACE gene. Furthermore, the effect of different antihypertensive drugs on SBP, DBP, and FBG level among different genotypes of ACE gene in both male and female EH patients and EHNOD patients separately was evaluated which was statistically nonsignificant (Table 5) along with the average change in the FBG level after 1 year of the antihypertensive therapies (Figure 2).
From our findings, we may conclude that among EHNOD patients, I allele may be positively associated with rise in FBG level. However, no significant difference was observed in different parameters with respect to different genotypes of ACE gene. Similarly, the effect of different antihypertensive drugs on FBG level with respect to different genotypes of ACE gene gave nonsignificant results for all drug therapies.
Conclusions
In our study, we did not find any association of ACE gene polymorphism with the risk of new onset of diabetes in EH patients of Haryanvi population. Results are confusing and more studies with large sample and longer duration of time are needed to evaluate the exact role of ACE gene polymorphism in antihypertensive therapy induced type 2 diabetes mellitus.
Footnotes
Acknowledgements
We would like to acknowledge the team of doctors and volunteers at M. M. Institute of Medical Science and Research, M. M. University, Mullana, Ambala, India, for their help in collecting the data and blood samples during the study. We would also appreciate HOD, Department of Biotechnology, IIT, Roorkee, for analyzing the samples for genotypic studies.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceived and designed the experiments: SG, VJ. Analyzed the data: VJ. Wrote the first draft of the manuscript: VJ. Contributed to the writing of the manuscript: VJ. Agree with manuscript results and conclusions: SG. Jointly developed the structure an arguments for the paper: SG, VJ. Made critical revisions and approved final version: SG. All authors reviewed and approved of the final manuscript VJ, SG, PR, BKG, VS.