
Abstract
Background/objectives:
In the current era of modern technology and the development of smart devices such as the flash glucose monitoring (FGM) systems, patients can easily monitor their glucose levels more frequently without any inconvenience. In this study, we evaluate the effect of FreeStyle Libre FGM system on glycemic control, hypoglycemia, health-related quality of life (QoL), and the fear of hypoglycemia (FOH) among children and young people with type 1 diabetes (T1D).
Design and methods:
A prospective study was conducted at the Diabetes Treatment Center, Prince Sultan Military Medical City, Riyadh, Saudi Arabia, between January 2017 and May 2017 on 47 (aged 13-19 years) registered patients with T1D who used conventional finger-pricking method for self-testing the glucose. At baseline visit, the FGM sensors were placed on each participant by a trained diabetes educator. The data collected from the sensors were computed to generate the respective ambulatory glucose profiles so as to determine the total number of scans conducted during the study period. At the baseline and at 3 months of the experiment, a trained interviewer administered the questionnaire Hypoglycemia Fear Survey-Child Version (HFS-C) and PedsQL 3.0 (QoL questionnaire) to each patient. The age, sex, weight, height, adjusted body mass index, duration of diabetes, treatment modality, and glycosylated hemoglobin A1c (HbA1c) levels of each patient were recorded.
Results:
As compared with the baseline, a significant improvement was noted in the behavior of FOH (P = .0001), worry (P = .0001), QoL (P = .002), HbA1c level (P = .008), and hypoglycemia (P = .023) at 3 months. Significant improvement was noted in the behavior (P = .0001), worry (P = .0001), QoL (P = .003), HbA1c level (P = .014), and hypoglycemia (P = .001) among the multiple-dose insulin injection–treated patients as compared with baseline. Significant improvement was noted in the behavior (P = .0001), worry (P = .0001), and hypoglycemia (P = .001) among the insulin pump–treated patients as compared with baseline. A positive correlation was recorded in the behavior (r = .47; P < .001), QoL (r = .70; P < .001), and the mean number of FGM scans. A negative correlation was recorded in the worry (r = −.43; P = .002), HbA1c level (r = −.58; P < .001), hypoglycemia (r = −.65; P < .001), and the mean number of FGM scans.
Conclusions:
The frequent use of FGM scanning reduced the frequency of hypoglycemia, HbA1c level, and worry and increased the behavior and QoL. As compared with self-testing by the conventional finger-pricking method, the use of FGM increased the frequency of self-testing and thus diabetes control.
Keywords
Introduction
Despite being noncurable, diabetes can be managed effectively by regular evaluation of the blood glucose level. Self-monitoring of blood glucose is considered to be an effective tool for this purpose, especially for patients with type 1 diabetes (T1D). 1 Several studies have reported that children or adolescents with T1D, who are required to maintain their glycemic control, do not opt for self-monitoring because of the fear of needles.2,3 For several other patients, who are both newly diagnosed and are managing their diabetes over a long period of time, the self-testing process itself is often the cause of a huge distress that decreases their quality of life (QoL). However, unlike children with other chronic childhood diseases, children with T1D must accept needles as a part of their daily lives. 3 In fact, one of the most significant factors that affect diabetes management and negatively affects the diabetes treatment outcome is the fear of needles and its perceived relationship with pain.3,4 In this regard, many researchers have reported that the fear of blood and being injured are directly associated with less frequent self-testing and poor glycemic control. Nevertheless, self-testing is important to minimize the risk of diabetes, such as hypoglycemia, which can lead to considerable discomfort and the risk of developing serious complications in future. 5
With the advancement in scientific technologies, much effort has been made to facilitate convenient self-testing processes in diabetes by means of modern technology. In addition, as patients have themselves become more technologically savvy and devices have become more easily available, the advent of new technologies has been materialized, and a range of smart self-testing strategies have been developed.6–8 In response to overcoming the fear of finger pricking in the conventional self-testing processes, a new technology known as the flash glucose monitoring (FGM) system (FreeStyle Libre [FL]; Abbott Diabetes Care, Witney, UK) has evolved. The FGM system mechanically reads and continuously measures the glucose concentration in the interstitial fluid glucose collected from cells immediately below the skin and produces the corresponding ambulatory glucose profile (AGP) by downloading the glucose measurements from the sensor to the reader; this process eliminates the limitations of frequent and painful finger pricks currently used to monitor glucose levels. 9 As supported by several recent studies, FGMs are precise and well tolerated by patients that effectively reduce glucose variability, increase time in range, and are easy to wear and use.10–13
A few recently published articles have focused on different objectives in relation to FGM, such as the influence of FGM on the hemoglobin A1c (HbA1c) levels and hypoglycemia.14–16 However, to the best of our knowledge, there exists no research that addresses the effects of FGM and its influence on QoL and the fear of hypoglycemia (FOH) among children or adolescents with T1D. Hence, we aimed to determine the impact of FGM system usage on glycemic control, hypoglycemia, QoL levels, and FOH among children and young people with T1D.
Methods
Study design and sampling
We conducted a prospective study at the Diabetes Treatment Center, Prince Sultan Military Medical City (PSMMC), Riyadh, Saudi Arabia, between January 2017 and May 2017 on 47 (aged 13-19 years) registered patients with T1D who used conventional finger-pricking method for self-testing the glucose. The selection of the respondents was deliberate and careful, and the selected suitable patients were assigned with specific identification numbers. Patients diagnosed in the preceding 6 months with any dermatological disorders or changes at the site of sensor application, severe or unstable medical conditions, severe hypoglycemia (such that it requires third-party assistance), diabetic ketoacidosis, or a hyperosmolar-hyperglycemic state were excluded from the study. All participants reserved unconditional or absolute “right” of withdrawal at any point of time in the study without giving any reason or prior notice.
The participants or their parents/caregivers were advised of their roles in this study, and a signed informed consent was obtained from them prior to the recruitment of the subjects. The patients’ demographic data, clinical characteristics, and treatment history (administration of multiple daily injections and insulin pump) were collected at the baseline using a standardized case record form at the first study visit. The study protocol was approved by the Research Ethics Committee of the PSMMC in accordance with the Helsinki Declaration of 1964 (as revised in 2013).
Education about FGM
A comprehensive learning and written instruction about the FGM system, such as asking the patients to hold the reader 1 to 4 cm away from the sensor for 1 second, informing that the sensor can be scanned through clothing, and demonstrating how to change the sensor once every 14 days, were provided to each participant and their parents/guardians before the study commenced. The study participants were instructed to confirm their blood glucose level with a capillary measurement in case of imminent and/or suspected hypoglycemia, rapidly changing glucose levels, or when the symptoms did not match the system’s reading using the blood glucose meter built-in the reader. In addition, all study participants were allowed to meet or contact the educator at any point of time during the study.
After the educational session, the FL sensors were applied at the back of the upper arm of each participant by a trained diabetes educator, who was deemed competent to perform the application and the training procedure. Each participant was subjected to 6 sensors, excluding 2 extra sensors in case of sensor detachment. At the end of the study, the complete data from the sensors were computed to produce the corresponding AGPs so as to determine the total number of scans performed during the study period (90 days). The mean number of scans/day was considered for data interpretation.
Glycosylated hemoglobin and hypoglycemia
The HbA1c level of <7% signifies a good control of the blood glucose level. Hypoglycemia was defined as a confirmed blood glucose value of ≤70 mg/dL. In this study, the HbA1c levels were analyzed using the COBAS INTEGRA 400 plus/800 analyzers at the central laboratory of PSMMC twice: once at the baseline and then at 3 months of the initiation of FGM testing. The frequency of incidence of hypoglycemic episodes was also collected from the device reports.
Survey of hypoglycemia fear
We employed the Hypoglycemia Fear Survey-Child (HFS-C) version to estimate the level of worries in child subjects and their behaviors in relation to hypoglycemia.17,18 The HFS-C is a 32-item survey questionnaire that comprises a 10-item behavior subscale (HFS-B), a 15-item worry subscale (HFS-W), and 7 questions about response to hypoglycemia under special circumstances (the frequency of hypoglycemia episodes was reported on a per month basis). The HFS-W measured the anxiety-provoking aspects of hypoglycemia, whereas the HFS-B measured the specific behaviors adopted by the children to avoid hypoglycemia. The response to each item was rated on a 5-point Likert scale ranging from 1 (never) to 5 (always). Accordingly, higher scores indicated higher FOH, with high levels of internal consistency (α = .86) for the overall score.17,18
PedsQL 3.0 DM questionnaire
The PedsQL 3.0 DM is a modular tool designed to measure QoL in children and adolescents affected by diabetes. The questionnaire is about 5 to 8 minutes long and includes 28 items: 5 dimensional scales that include questions on diabetes symptoms (11 items), treatment barriers (4 items), treatment adherence (7 items), worry (3 items), and communication (3 items). The instructions inquire about the extent of a problem proposed by each item during the past 1 month. The format, instructions, Likert-type response scale, and the scoring method were as follows: 0 = never a problem, 1 = almost never a problem, 2 = sometimes a problem, 3 = often a problem, and 4 = almost always a problem. Items are reverse scored and then linearly transformed to a 0 to 100 scale (wherein, 0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0); therefore, higher scores indicated better QoL or fewer symptoms/problems. The PedsQL 3.0 DM was validated for use in Arabic language.19,20
Statistical analysis
Data analysis was performed using Microsoft Excel 2013 (Microsoft Corporation, Seattle, WA, USA) and the Statistical Package for Social Sciences (version 22; SPSS Inc., Chicago, IL, USA). Two-tailed paired t test was conducted to determine the differences among the sets with respect to the different time points (baseline versus 3 months). Correlation between the total number of scans performed in a day (mean value) and the HbA1c levels, hypoglycemia, FOH, and QoL were performed using the Pearson correlation coefficient. P < .05 was considered to be statistically significant.
Results
Table 1 describes the characteristics of the study population. Most of the study population are in the 17 to 19 years age group (61%), which includes patients with diabetes for ≥10 years (61.7%), those having undergone multiple-dose insulin injection (MDI) treatment (61.7%), and those with body mass index <25 (80.9%).
Baseline characteristics of the study population (n = 47).
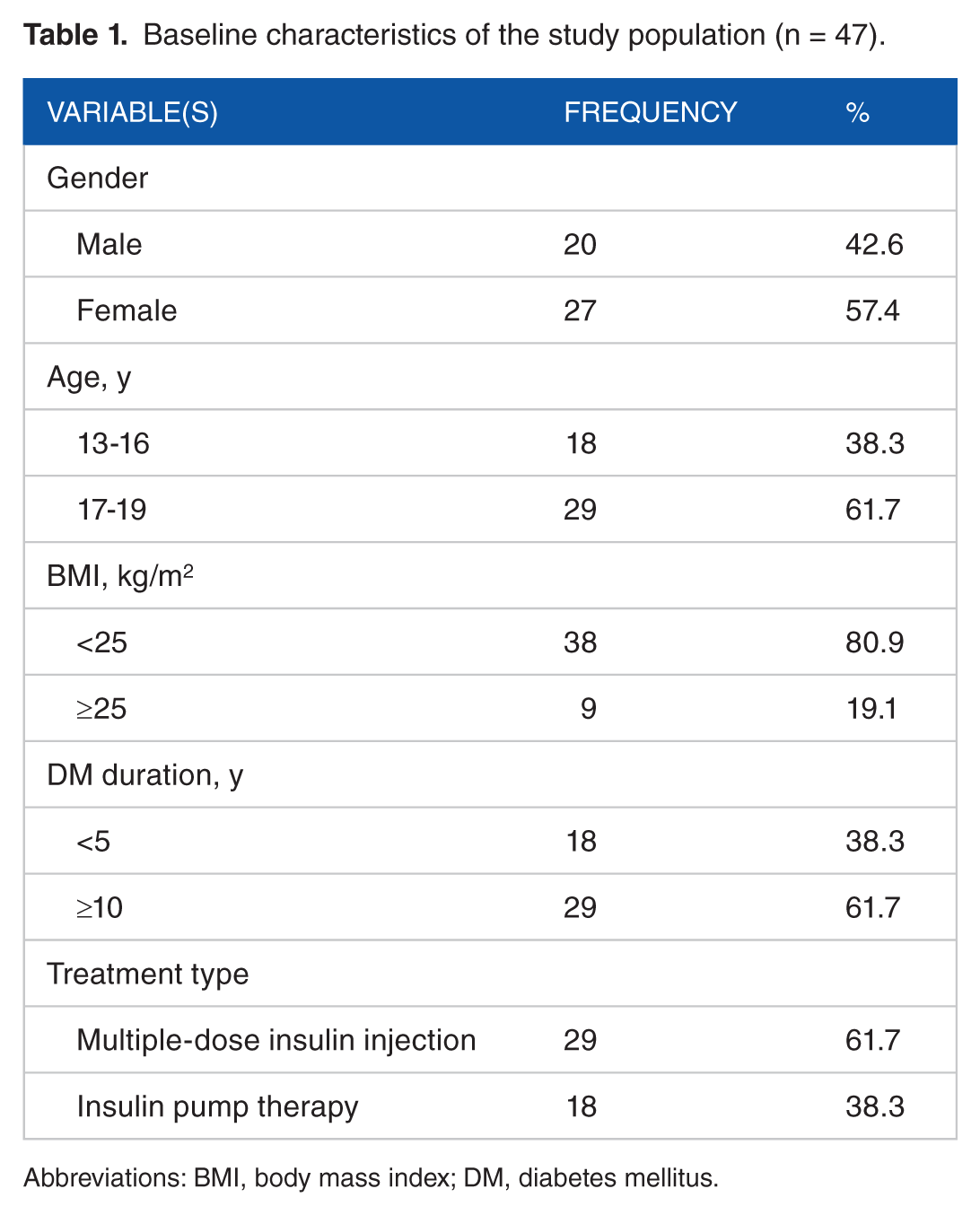
Abbreviations: BMI, body mass index; DM, diabetes mellitus.
Table 2 shows the differences in the behavior, state of worry, QoL, HbA1c levels, and hypoglycemia measured at 3 months after the study. As compared with the baseline level, significant positive differences can be seen in the behavior of FOH (P = .0001), worry (P = .0001), QoL (P = .002), HbA1c level (P = .008), and hypoglycemia (P = .023) at the end of the study.
Comparisons of before (baseline) and after (3 months) use of FreeStyle Libre on fear of hypoglycemia, quality of life, hemoglobin A1c, and hypoglycemia.

Groups compared by 2-tailed paired t test.
P < .05 baseline versus 3 months.
Table 3 depicts the hypoglycemia history among the study population. Most of the patients reported 1 to 2 episodes per month at the baseline level. However, reductions in the frequency of hypoglycemia episodes were reported at 3 months of the study. Similar results were found on blood sugar, such as had a big problem, had passed out due to hypoglycemia, had a hypoglycemic episode while asleep, hypoglycemic episode while awake, had hypoglycemia in front of friends or strangers, and had hypoglycemia at school, among the participants.
Hypoglycemia history among the study population.
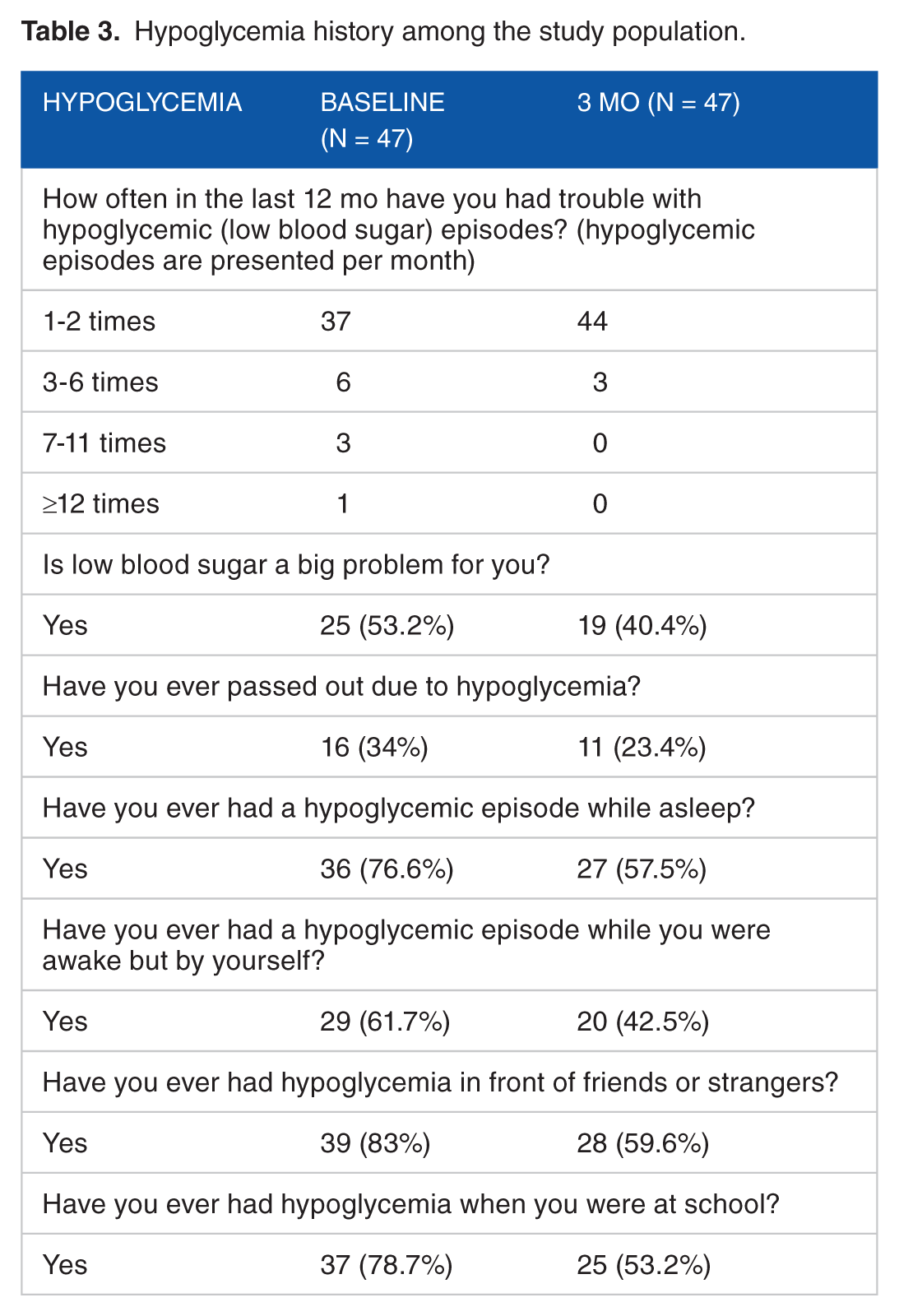
Table 4 gives the differences between MDI and insulin treatment groups on behavior, degree of worry, QoL, HbA1c level, and hypoglycemia at 3 months of the study. Significant improvement was noted in the behavior (P = .0001), worry (P = .0001), QoL (P = .003), HbA1c level (P = .014), and hypoglycemia (P = .001) among the MDI-treated patients as compared with baseline. Significant improvement was noted in the behavior (P = .0001), worry (P = .0001), and hypoglycemia (P = .001) among the insulin pump–treated patients.
Baseline and 3 months comparison of multiple-dose insulin injection and insulin pump–treated patients on fear of hypoglycemia, quality of life, HbA1c, and hypoglycemia.
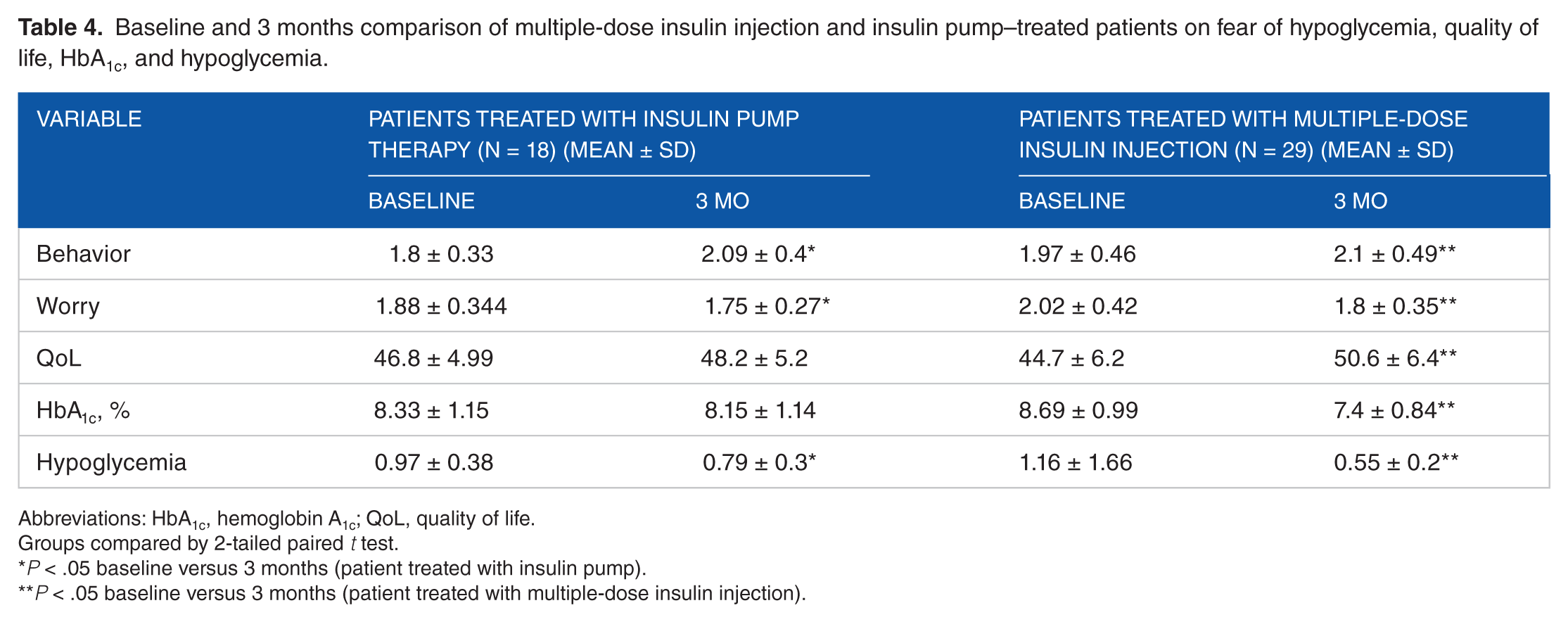
Abbreviations: HbA1c, hemoglobin A1c; QoL, quality of life.
Groups compared by 2-tailed paired t test.
P < .05 baseline versus 3 months (patient treated with insulin pump).
P < .05 baseline versus 3 months (patient treated with multiple-dose insulin injection).
A positive correlation can be seen in the behavior (r = .47; P < .001), QoL (r = .70; P < .001), and the mean number of FGM scans. A negative correlation can be seen in the worry (r = −.43; P = .002), HbA1c level (r = −.58; P < .001), hypoglycemia (r = −.65; P < .001), and the mean number of FGM scans.
Discussion
As per the guidelines of various organizations and previous researches, the blood glucose level should be self-monitored at least 3 times a day by patients with T1D, including both fasting and postprandial glucose measurements.21–25 However, due to painful, inconvenient, and invasive nature of the finger-pricking step involved in the conventional or classic self-testing methods, several patients find it difficult to follow the recommended testing frequency. 17 In the current era of modern technology and the development of smart devices such as the FGM systems, patients can easily monitor their glucose levels more frequently without any inconvenience. 6 To verify this notion, we tested the hypothesis whether FGM usage over a period of time influences the HbA1c level and hypoglycemia in patients with T1D.
According to the findings of this study, the study participants preferred the FGM system over the finger-pricking method and hence used FGM for self-testing more frequently. Notably, the frequency of self-testing among the study population by the finger-pricking method was 0.84 times per day at the baseline, whereas it was 6.76 by FGM scanning (difference of 5.92 times per day), which is 8 times greater than that by self-testing by finger pricking). It has been reported that self-monitoring of blood glucose levels is associated with a modest, statistically significant reduction in the HbA1c levels, regardless of whether the patients are preinformed about how to interpret and use the test results. 26 In addition, studies reported that the frequency of self-monitoring is associated with improved HbA1c levels and decrease in other diabetes-related complications because of the obvious link between daily monitoring and control.27,28 This findings was further confirmed by our results that patients with higher number of daily FGM scans showed significantly improved levels of HbA1c, most probably due to both better insulin adjustment for the consumed food and an improved ability to correct out-of-target glucose values in time. This study also showed that as compared with the baseline, the frequency of hypoglycemia significantly decreased (0.37 frequency/month, P = .034) at 3 months after the 3 months use of FGM; this result is in concordance with similar past ones which reported that early and frequent monitoring of lower glucose values prior to symptomatic hypoglycemia may allow for the correction of diabetes level and decrease the risk of overcorrection and the resultant hyperglycemia.8,27,29 The correlation analysis of this study showed that a negative correlation was found between the HbA1c level (r = −.58; P < .001), hypoglycemia (r = −.65; P < .001), and the total number of FGM scans in the study population. The above findings evidently indicated that frequent FGM scanning can efficiently reduce the frequency of hypoglycemia and HbA1c levels.
To determine the cofactors that create barriers in self-testing, we examined the effect of FGM and its influences on FOH and QoL. Some previous studies have reported that because of the aversive nature of hypoglycemic episodes and the associated risk for harm thereof, individuals with T1D can develop a significant FOH, which can negatively affect their QoL.17,30 Although some extent of fear can be considered appropriate and adaptive given the potential risk of hypoglycemia, it may become life-threatening and challenging for some patients. For these patients, FOH may cause great anxiety about diabetes management, obsessive self-monitoring, deliberate maintenance of high blood glucose levels, co-dependency, feelings of guilt and frustration, a perceived sense of loss of control, embarrassment, relationship stress, and avoidant behavior. 31 We found significant positive differences in the in the behavior of FOH (P = .0001), worry (P = .0001), QoL (P = .002), HbA1c level (P = .008), and hypoglycemia (P = .023) at 3 months for the study population by means of univariate analysis. In addition, we noted a positive correlation in the behavior (r = .47; P < .001) and QoL (r = .70; P < .001) as well as in the total number of scans performed at 3 months in comparison with those at the baseline. These results clearly support that the higher frequency of FGM scan positively correlates with the behavior and QoL of patients with diabetes.
Self-testing is known to be effective in enhancing the degree of self-care in patients with diabetes. It heightens the feeling of empowerment in patients with diabetes by helping them accurately estimate the positive effects of alterations in lifestyle and medications on their blood glucose levels. As reported by some researches, finger-pricking method is considered painful by certain patients, who therefore avoid the regular practice of self-testing, even in developed countries. In the United States and in Italy, only a minority of patients with diabetes and those who are injected with insulin tested at least once daily, despite the availability of monitoring devices for free in Italy.4,32,33 After the increased frequent scanning by FGM system, we noted significant improvement in the tested factors, including FOH (behavior) QoL, and HbA1c among the study population at 3 months, which is not unexpected because the frequency of self-testing improved among the study population with the use of advance technology.
This study had few limitations, including the small sample size and the inclusion of only one center for study. More number of studies performed on a larger scale are thus warranted to address these limitations. Nevertheless, this study delivers valuable data about the FGM system and provides helpful insights to its significant positive improvement among adolescents with T1D.
In conclusion, the findings of this prospective study clearly demonstrated that frequent FGM scanning can effectively reduce the frequency of hypoglycemia, HbA1c levels, and FOH and increase the QoL. As compared with self-testing by the conventional finger-pricking method, FGM scanning can increase the frequency of self-testing among patients. Further studies are required to determine whether improved outcomes can be achieved with the prolonged and consistent use of the FGM system.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AAAH and MAAD conceived and designed the experiments and contributed to the writing of the manuscript. AAAH and AAR wrote the first draft of the manuscript and agreed with manuscript results and conclusions. MAD made critical revisions and approved the final version of the manuscript. All authors reviewed and approved the final manuscript.
Informed Consent Statement
During the informed consent process, study participants are assured that data collected will be used only for stated purposes and will not be disclosed or released to others without the consent of the participants.
Institutional Review Board Statement
The study protocol was approved by the Research and Ethics Committee of Prince Sultan Military Medical City, Riyadh, Saudi Arabia.