
Abstract
Aims
To study the respiratory variation of right atrial (RA) pressures at baseline and during atrioventricular nodal reentry tachycardia (AVNRT).
Methods
Of the 23 patients screened, 16 participants with typical AVNRT were included in the study. After ensuring adequate hydration, baseline RA pressures were measured as the height of ‘a’ and ‘v’ waves. The patients were asked to take deep breaths, and the measurements were taken in both inspiration and expiration.
Results
Of the 16 participants, 14(87.5%) showed a normal fall in the height of ‘a’ and ‘v’ waves with inspiration, 1(6.25%) showed no change and 1(6.25%) showed a rise in height at baseline, p <0.01. During induced AVNRT, the ‘a’ and ‘v’ wave heights increased in 8(50%), remained same in 6(37.5%) and showed a normal fall in 2(12.5%), p = 0.07 for ‘a’ waves and p = 0.09 for ‘v’ waves. When the magnitude and direction of change in ‘a’ and ‘v’ wave height at baseline was compared with AVNRT, it showed a significant difference with 13(81.25%) participants demonstrating positive Pseudo-Kussmaul's sign, p <0.01. Mean age was numerically higher in those with a more considerable inspiratory rise in RA pressures but was not statistically significant, χ2(2) = 3.1, p = 0.21.
Conclusions
Pseudo-Kussmaul's sign does occur in a substantial number of patients during AVNRT. Clinical appreciation of this phenomenon is possible in half to three-fourth of patients, provided the mean RA pressures are low enough for the variation to be visible in the neck.
Keywords
What's new?
Kussmaul's-like respiratory variation of right atrial pressures has not been described in the context of AVNRT.
Our study demonstrates the presence of such a phenomenon, and the frequency of occurrence in this group of patients.
This provides unique insights into the understanding of hemodynamics during AVNRT.
Introduction
Jugular venous pressure (JVP) changes during atrioventricular nodal reentry tachycardia (AVNRT) have been well described. It is one of the causes of regular cannon waves 1 leading to its named clinical sign called as Frog sign. 2 We came across a few patients with ongoing AVNRT who showed a respiratory variation in the height of cannon waves (Supplementary Video 1, Supplementary Video 2). This respiratory variation was opposite to that normally expected in patients with normal systolic and diastolic function of the left ventricle. It showed an increase in the height of JVP with inspiration. This paradoxical increase did not occur once the tachycardia was terminated.
Normal JVP should fall with inspiration. An increase in its height with inspiration is called Kussmaul's sign. 3 This sign is not commonly described in the context of AVNRT. Due to the lack of literature describing this phenomenon, we decided to conduct this study in patients presenting with typical AVNRT to assess its reproducibility. The hypothesis we intended to test was whether patients with a normal respiratory variation at baseline demonstrated an inspiratory rise in right atrium (RA) pressures during AVNRT.
Methods
Trial Design and Oversight
This was a single-centre, prospective, cohort study conducted at U. N. Mehta Institute of Cardiology and Research Centre, Ahmedabad, Gujarat, India. The study was approved by the Institutional Ethics Committee and was conducted between October 2019 and March 2020. No patient or public was involved in the trial design, conduct or collection of data.
Patients and Trial Procedures
Consecutive patients over the age of 18 years and diagnosed with supraventricular tachycardia and structurally normal heart were enrolled in the study. Diastolic function was assessed based on the 2016 American Society of Echocardiography (ASE) and European Association of Cardiovascular Imaging (EACVI) guidelines. 4 After taking informed consent, they were posted for electrophysiology testing (EP) and radiofrequency ablation (RFA). Patients confirmed of having typical AVNRT were included in the study. The participants were hydrated well before they underwent pressure measurements. An 8F SR0 Fast-Cath guiding introducer catheter (St. Jude Medical, Plymouth, MN, USA) was passed through the right femoral vein, and the tip was placed at the mid-RA. The iPeX DPT-01 pressure transducer (B L Lifesciences Pvt. Ltd, UP, India) was connected to the catheter to measure the RA pressure waveforms. The patient was instructed to take deep breaths, and the ‘a’ wave and ‘v’ wave heights were recorded in each phase of respiration. We then proceeded with the induction of AVNRT and recorded the heights of ‘a’ and ‘v’ waves in each phase of respiration.
We performed all recordings on the hemodynamic monitor integrated with the Philips cath lab on the Xper Information Management System (Koninklijke Philips N.V., Amsterdam, Netherlands). The sweep speed was reduced to 10 mm/s. For recording the phases of respiration, the low pass filter was kept at the minimum available setting. Before taking measurements, the transducer was zeroed after placing it at a level horizontal to the RA. If, after zeroing of pressures, the RA pressures appeared too low or undetectable, IV fluids were infused through the right femoral vein until the mean RA pressures were more than 2 mm Hg. 5
Statistical Analysis
Normality of data was assessed using skewness and kurtosis, and Shapiro-Wilk test. Continuous variables are presented as mean (95% confidence intervals) unless otherwise specified; the median value is additionally mentioned for non-normal variables. Descriptive data is provided as a number (percentage of the sample). The difference in measurements of waveforms between inspiration (I) and expiration (E) was calculated. This difference was also compared between baseline (B) and during AVNRT (A). The study participants were classified based on whether they had a positive difference, negative difference or none and the same was shown in percentages. Nonparametric Wilcoxon signed-rank test was used to compare medians of paired samples, and the results were expressed as the standardised test statistic (z) with its p value. Kruskal-Wallis test was used to compare nonparametric continuous data with an ordinal dependent variable. An alpha error of 0.05 was accepted for statistical significance. All measured data is presented as a line graph, while the difference in medians between baseline and AVNRT is plotted as a bar graph.
Results
Of a total of 23 participants screened for the study, seven had atrioventricular reentry tachycardia (AVRT) and had to be excluded. Hence, 16 participants of confirmed typical AVNRT were included in the study. Mean age of the study population was 46.41 (38.04, 54.78) years.
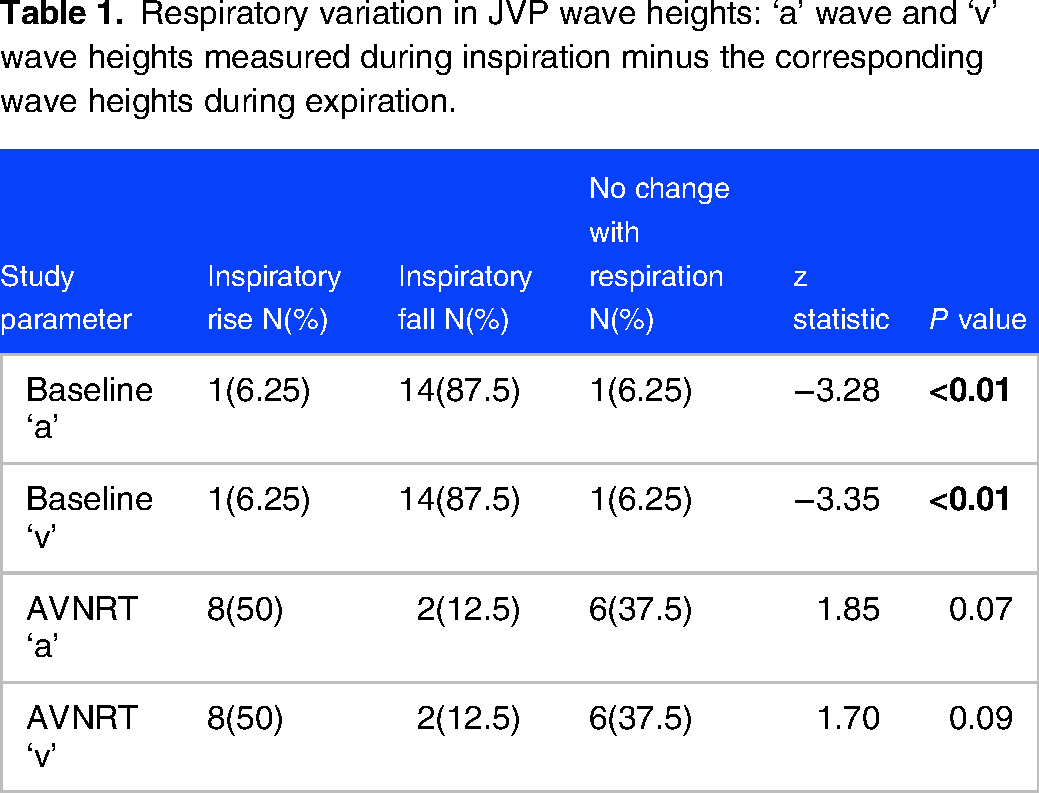
Of the 16 participants, 14(87.5%) showed a normal fall in the height of ‘a’ and ‘v’ waves with inspiration, 1(6.25%) showed no change and 1(6.25%) showed a rise in height at baseline. This change in height on inspiration was statistically significant, p <0.01 (Table 1, Figure 1). During induced AVNRT, the ‘a’ and ‘v’ wave heights increased in 8(50%), remained same in 6(37.5%) and showed a normal fall in 2(12.5%). This change in height did not attain statistical significance, p = 0.07 for ‘a’ waves and p = 0.09 for ‘v’ waves (Table 1, Figure 2).

Inspiratory change in ‘a’ and ‘v’ wave height at baseline. z = standardized test statistic of Wilcoxon signed-rank test.

Inspiratory change in ‘a’ and ‘v’ wave height during AVNRT. z = standardized test statistic of Wilcoxon signed-rank test.
Respiratory variation in JVP wave heights: ‘a’ wave and ‘v’ wave heights measured during inspiration minus the corresponding wave heights during expiration.
When the magnitude of change in ‘a’ wave height in AVNRT and baseline was compared, it showed a significant difference with p <0.01 (Table 1, Figure 3). There were 13(81.25%) participants who showed a considerable inspiratory change in ‘a’ wave in AVNRT compared to baseline. Not only the magnitude, but the direction of change was also generally different, with baseline values showing a normal fall while those with AVNRT showing no change or rise (Table 2).

Comparison of inspiratory change in ‘a’ and ‘v’ wave height at baseline and during AVNRT. z = standardized test statistic of Wilcoxon signed-rank test.
Difference in wave heights: ‘a’ and ‘v’ wave heights measured during AVNRT minus that during baseline.

To know the effect of age on the inspiratory change in RA pressures, the measurements were converted into an ordinal scale of three groups based on their response to inspiration (Figure 4). The first group (labelled 0) had a normal inspiratory decrease and included only two patients. The second group (labelled 1) did not show any change in height with inspiration, N = 6(37.5%), and the third group (labelled 2) showed an increase in height, N = 8(50%). Although there were no statistically significant differences in age between the three groups, there was a numerically higher mean age as we moved from the first to the third group. For the second group, mean age was 40.7(22.2, 59.1) and for the third group was 50(41.9, 58.1), Kruskal-Wallis χ2(2) = 3.1, p = 0.21 (Figure 4).
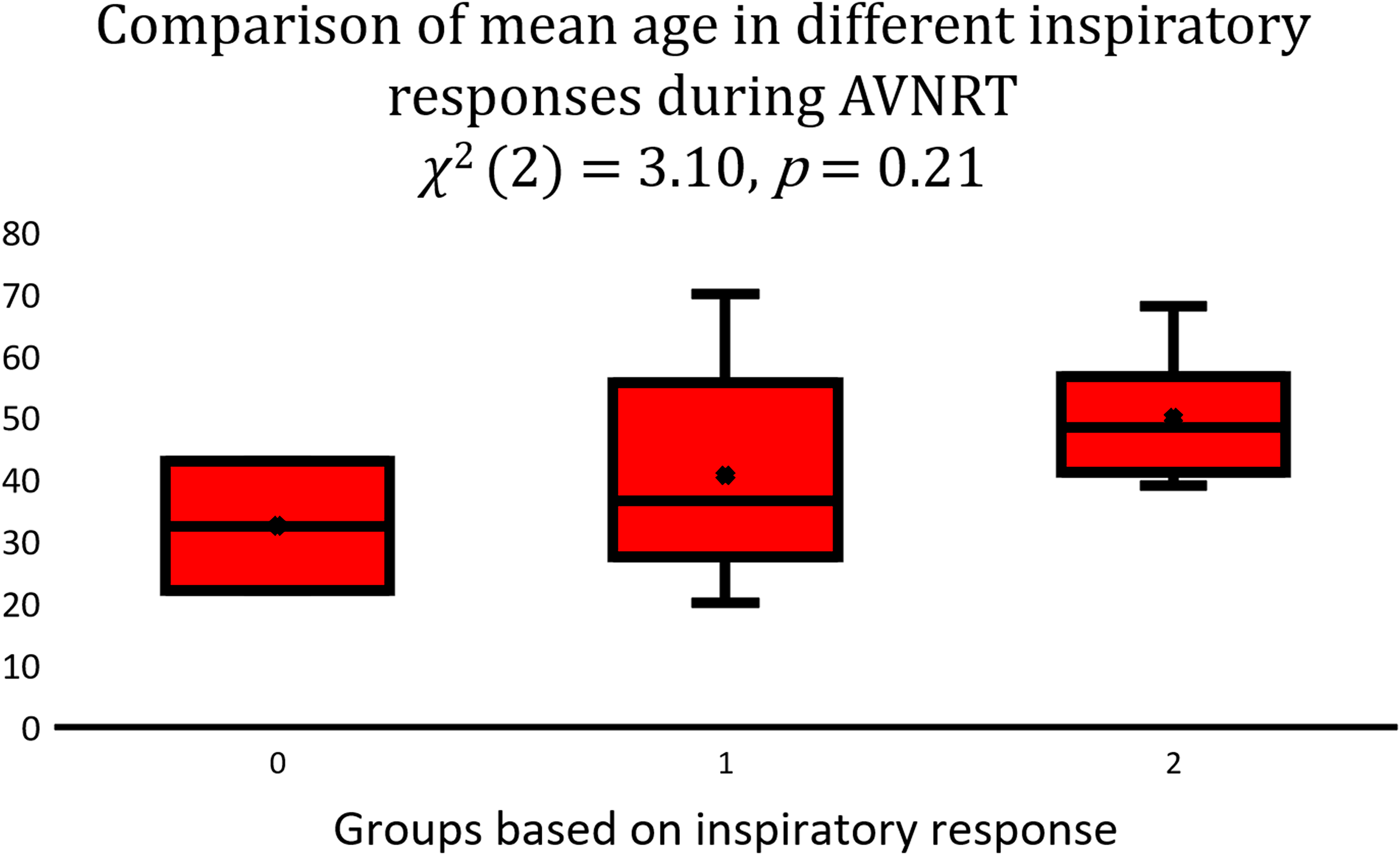
Comparison of mean age between groups classified based on their inspiratory response during AVNRT. Group 0 constitutes those who had a normal inspiratory fall in RA pressures, Group 1 had no change with inspiration, and Group 2 showed a rise in pressures with inspiration. Kruskal-Wallis test was used for statistical analysis.
Discussion
This study shows that normal inspiratory fall in RA pressures is uncommon during AVNRT. RA pressures either rise in 50% of patients or remain the same in 37.5% of patients. This difference in respiratory variation during AVNRT compared to baseline is statistically significant.
Kussmaul's sign is seen in constrictive pericarditis, acute right ventricular myocardial infarction, cardiac tamponade and acute pulmonary embolism. It is defined as a rise in the height of the JVP, or its failure to fall, with inspiration. 3 The primary pathology in these conditions lie in the right ventricle (RV). Here, the increased venous return to the RA during inspiration is not pushed forward with atrial systole because of a noncompliant RV. This is reflected as an increased height in ‘a’ wave during inspiration. Similarly, here in AVNRT, an increase in flow to the RA during inspiration results in an increase in RA pressures as filling of RV is impeded. This is because the RA contracts against a closed tricuspid valve. Also, since the primary pathology here does not lie in the RV, it could be termed as Pseudo-Kussmaul's sign. 6
Our study had 87.5% of participants who fit the definition of positive Kussmaul's sign. In contrast, only 2(12.5%) of participants had this sign at baseline. The respiratory change in median ‘a’ or ‘v’ wave height was not statistically different in the AVNRT group. This could be because of a high percentage (37.5%) of participants who did not show any change in JVP, which could have impacted the calculation of the median difference in heights.
The patients enrolled in this study all had structurally normal heart and no diastolic dysfunction. Besides, the same patients were used as controls to elicit the respiratory variation during AVNRT. This would have nullified diastolic dysfunction as a confounding factor as they would have had an inspiratory rise at baseline too.
The pressures measured in this study were RA pressures. It has been established that there is a discrepancy between mean RA pressures and JVP. There exists a valve with variable competence at the junction of the internal jugular vein and the innominate vein, that might be responsible for this discrepancy in pressures. 7 In half of the patients who showed a rise in JVP with inspiration, the observed range was 1 to 6 mm Hg. This translates to a JVP height of 1.36 to 8.16 cm H2O (as 1 mm Hg = 1.36 cm H2O). 8 This means that, based on the present study, if the RA pressures were such that the upper limit of the cannon waves could be seen in the neck, half of the patients would have a clinically appreciable inspiratory rise in JVP. Of the remaining half, three-fourth will have no change in JVP height with respiration while the remaining one-fourth will have a normal inspiratory fall. Finding the upper limit of cannon waves in mid-neck region is not common, and hence the practical application of this finding is questionable. However, this study does tell us that before we comment on the regularity of cannon waves, it is worthwhile to make the patient hold his breath in each phase of respiration.
Cannon waves occur when the atria contract against a closed tricuspid valve during ventricular systole. They can be regular, or irregular. 1 Irregular cannon waves typically have varying heights depending on which part of systole the atrial contraction falls. If the atrium contract against a slightly open tricuspid valve, the height of the cannon waves will be shorter than when it falls against a closed tricuspid valve. This is further proved by the presence of giant ‘a’ waves of constant height in tricuspid stenosis where the atrium always contracts against a fixed resistance. 9 We hypothesise that the changing AV nodal conduction properties, similar to that occurring in dual AV nodal pathways,10,11 may lead the retrograde P waves to fall at different parts of the QRS complex. This could result in the RA contracting against varying levels of tricuspid valve closure leading to changes in pressures.
Another possible hypothesis to explain this phenomenon pertains to chamber compliance. Usually, the amount of blood that the right heart can accommodate during inspiration depends on the compliance of the RA and RV. 5 In AVNRT, the change in the height of cannon waves may be more pronounced in those with a less compliant RA than in those with a more compliant one. This may explain why every patient with AVNRT did not show a respiratory variation in our study. Atrial compliance is known to decrease with age. 12 Although our study was not powered to analyse the difference in mean age between groups, it still showed a trend towards higher age with an inspiratory increase in JVP during AVNRT.
Irregular and regular cannon waves have different etiologies. While the former is seen in conditions with AV dissociation associated with junctional rhythm, ventricular tachycardia, or isorhythmic AV dissociation, the latter is commonly associated with ventricular tachycardia with retrograde VA conduction, atrial flutter with 2:1 AV block, AVNRT, etc. 1 Understanding the regularity of the cannon waves is the initial step towards formulating a differential diagnosis. In doing so, the respiratory variations are seldom taken into account, which could result in the clinician being misdirected. As demonstrated in the Supplemental Video 1 and 2, respiratory variation can be commonly encountered in clinically practice as AVNRT usually occurs in structurally normal hearts.
The clinical appreciation of this respiratory variation will depend on the hydration of the patient and the compliance of the left atrium. While the lack of respiratory variation in cannon waves will seldom cause a confusion, the variation, if present, should prompt the clinician to carefully time it with respiration to find out if it is a truly irregular cannon wave, or a regular cannon wave having respiratory variation.
Conclusion
Pseudo-Kussmaul's sign does occur in a substantial number of patients during AVNRT. Clinical appreciation of this phenomenon is possible in half to three-fourth of patients, provided the mean RA pressures are low enough for the variation to be visible in the neck. Age-related decrease in atrial compliance and varying cycle lengths of AVNRT with respiration are possible hypothesis to explain this phenomenon. This study emphasises the importance of timing the regularity of cannon waves in each phase of respiration. We are conducting a similar study in patients with other types of supraventricular tachycardias, like paroxysmal atrial tachycardias, atrioventricular reentry tachycardias and atypical AVNRT, to supplement our understanding of this phenomenon further.
Footnotes
Author contribution(s)
Availability of Data and Materials
All original data collected and the statistical outputs will be shared along with this submission.
Consent to Participate
The consent to participate was not obtained as only the usual protocols for AVNRT were followed and no additional procedures were performed. The data that were already being obtained during the electrophysiology procedures were used for this study.
Consent for Publication
All necessary written consents were obtained from patients for publication of videos.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This was obtained from the institutional ethics committee UNMICRC affiliated to the B. J. Medical College, Ahmedabad (ECR/1254/Inst/GJ/2019) with approval number EC/Approval/20/Cardio/13/06/2022.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.