
Abstract
BACKGROUND
The new coronavirus causes systemic inflammation and damage to various organs. So, this study aimed to follow up patients with COVID −19 after recovery for three months by performing cardiac, pulmonary and laboratory tests.
MATERIALS AND METHODS
This was a prospective cohort study of COVID-19 patients who were discharged from Baharloo Hospital. The diagnosis of COVID-19 was confirmed by PCR or long CT scan. Inclusion criteria were age over 18 years and patients with more than 50% of pulmonary involvement in lung CT scan. The patients were called to Baharloo hospital three months after recovery and were examined for cardiac, pulmonary and blood tests.
RESULT
Our study included 178 participants with mean age of 55.70, and 50.6% of them were male. Among pulmonary factors in the hospital, 71.9%, 15.7%,1.7%,19.1% and 53.4% had positive GGO, consolidation, reverse halo sign, traction bronchiectasis and vascular enlargement, respectively. After three months follow up, percentage of patients who had reticulation, honeycombing, fibrotic brand and bullae were 12%, 1.1%,8.4% and 0%, respectively. The Mean values of FVC and FEV1 were reported 4.21 and 3.01, respectively. Among Cardiac factors, positive PVC, PAC and mean Pap were decreased after three months. Only Growth in myalgia and Decreased sense of taste were statistically significant. Also, D dimer, UA protein, PMN, Ferritin CRP, PMN, LDH and HB amounts had decreased significantly.
CONCLUSION
Our study indicated that in addition to pulmonary changes, rapid damage to other organs and the occurrence of cardiac symptoms and changes in laboratory result were also reported in patients recovered from COVID-19.
Introduction
In December 2019, an outbreak of a new type of coronavirus (COVID-19) with acute respiratory symptoms was reported in Wuhan, China, which spread rapidly around the world and became one of the most important global problems. 1 Evidence suggests that the new coronavirus first infects the lungs, then causes systemic inflammation and damage to various organs, and eventually death. 2 Although the virus is less likely to cause mortality than its predecessor, SARS, it has a much higher potential for transmission and spread in the community, which in total can cause more deaths. 2 As of 28 February 2022, the disease has infected more than 400 million people worldwide and caused the deaths of more than 5.5 million people, according to the World Health Organization. 3 Reports of virus mortality vary, with about 6.5% in China and 2.15% abroad China..4,5 The results of blood and histological examinations of critically ill COVID-19 patients showed a decrease in the number of peripheral lymphocytes and an increase in inflammatory markers, which indicates overactive function and disruption of the patient's immune system.2,6 Although at the beginning of the outbreak of the disease, its symptoms were more in the form of fever and respiratory problems, 7 but rapid damage to other organs and the occurrence of cardiac, gastrointestinal, dermatological, neurological and renal symptoms were also reported in patients with this disease.8,9 Some studies have looked at the long-term follow-up of people with SARS who have recovered. The results of these studies indicate a high probability of developing pulmonary, cardiac, hepatic and psychological disorders after recovery from the disease.10,11 Different studies demonstrated that most of the COVID-19 survivors had symptoms including fever, sputum production, fatigue, diarrhea, dyspnea, cough, chest tightness on exertion and palpitations in the three months after discharge.12,15
Due to the emergence of COVID-19, little is known about the long-term effects of this disease. However, as for reported multisystemic involvement of the disease, as well as studies of the long-term effects of SARS, patients with COVID-19 who have recovered are more likely to have complications. So, in this study, we decided to follow up patients with COVID −19 after recovery for three months by performing cardiac, pulmonary and laboratory tests.
Materials and Methods
Study design and patient selection
This was a prospective cohort study on survivors of COVID-19 patients discharged from Baharloo hospital in Tehran, from January 2021 to September 2021. The diagnosis of COVID-19 in patients with high clinical suspicion was confirmed by PCR or lung CT scan by two experienced radiologists. Hospitalization criteria were Tachy Penea (RR> 30) and shortness of breath, PaO2 / FiO2 ≤300 mm Hg and SpO2 <90%, Increasing Aَ-a gradient equation and also involvement of more than 50% of the lung in CT scan. (A-a) gradient can be estimated indirectly using the partial pressure of oxygen (P o2) (obtained from blood gas analysis) in a simple mathematical formula:[A-a gradient = P o2 in alveolar air (estimated from the alveolar gas equation) – P o2 in arterial blood (measured from a blood gas)].
Inclusion and exclusion criteria
Inclusion criteria were age over 18 years, definite diagnosis of COVID-19, patients with more than 50% of pulmonary involvement in lung CT scan (CT scan at the time of visit or during hospitalization). Exclusion criteria were patients who need aggressive mechanical ventilation during hospitalization and intubate, people who smoke (cigarettes or smoked substances/recently or at any time before), people with a history of chronic lung disease, people with chronic organ failure (heart, kidney, liver), participants who have received chemotherapy recently and Insulin-dependent diabetics patients. (Figure 1)

Consort diagram of 178 included patient
The hospital's statistics officer first provided the details of patients between the ages of 30 and 60 who had been hospitalized since the beginning of the epidemic. Then, through the Pax CT scan system, these patients were isolated by a radiologist to examine those with more than 50% lung involvement. Patients were contacted by telephone and were talked to the them or their first-degree relatives about the aim of the study. It was explained that participation in the study will be completely voluntary. Also, benefits of participating in the study and the problems that may occur during the study were described. The patient was given 24 hours to make a decision, after which he/she was contacted again and entered the study with his/her informed consent.
Primary patient information including demographic information (age, gender, body mass index), clinical information of patients at the time of COVID-19 infection (signs and symptoms, duration of hospitalization, smoking history, history of underlying disease, medications received, ICU admission) was recorded in checklists designed for this purpose.
Treatment strategy and medicines used
The patients in our study were those who were in the severe respiratory and critical phase of COVID-19. At this stage there is wide range of more severe clinical symptoms. These symptoms in sever phase include:
Rapid progression of respiratory symptoms Taki Penne (30> RR) and shortness of breath PaO2 / FiO2 ≤300 mm Hg, SpO2 <90.3% Increasing A- a gradient and also involvement of more than 50% of the lung in CT scan Patients with symptoms of respiratory failure: despite non-invasive oxygen therapy SpO2≤ 88% Patients with symptoms of shock The patient needs mechanical ventilation or is under mechanical ventilation The patient suffers from multiple organ failure
These symptoms in critical phase include:
The Treatment strategy for the critical stage of COVID-19 patients based on tenth edition of Ministry of Health and Medical Education of Iran (MOHME) are:
Remdesivir prescription
Based on the proposed priority, the iniation of Remdesivir treatment was considered as a three-day treatment period up to the first 7 days from the onset of patient's symptoms requiring oxygen. The treatment is as follows:
Remdesivir 200 mg IV on day 1
Remdesivir 100 mg IV on day 2 and up to 5 days
Corticosteroids
Methylprednisolone 40/250 mg, Dexamethasone 8 mg intravenously daily for a maximum of 10 days or oral prednisolone tablets 0. 5 mg/ kg for a maximum of 10 days
Higher doses of corticosteroids and pulse therapy may be prescribed as salvage therapy based on the clinical judgment of the attending physician and the patient's condition.
Initiation of preventive anticoagulant therapy:
Heparin 5000 IU SC TDS
BMI≥40: Heparin 7500 IU SC TDS
Or
Enoxaparin 40 mg SC once daily
BMI ≥ 40: Enoxaparin 40 mg SC BID
Supportive therapies
Antibiotics in patients with suspected bacterial respiratory infections and other infectious causes,
CAltra tablets (lupinavir / ritonavir) 200/50 mg every 12 hours, 2 times a day for at least 7 days and up to 14 days
Tablets (Atazanavir / Ritonavir) 300/100 mg, One daily tablet with food or Atazanavir 400 mg daily for a minimum of 7 days and a maximum of 14 days
Interferon beta-1b (1b-β IFN) 250 micrograms by subcutaneous injection every other day for 5-7 doses
Interferon beta-1a (1a-β IFN) 44 micrograms by subcutaneous injection of 5-7 doses every other day.
Other treatment in critical phase
Convalescent plasma: If plasma therapy is needed according to physician opinion, it should preferably be started from the beginning of the disease (in the first 72 hours).
The use of IVIG in hospitalized patients is allowed only if a clinical decision is made under the supervision of a three-member team consisting of the attending physician and two lung or infectious or internal or intensive care specialists.
Discharge criteria
The following criteria were considered for the discharge of hospitalized patients from COVID-19 wards:
The fever has been stopped for at least 24-48 hours without the use of febrifuge, Respiratory symptoms such as cough are convalesced (persistent cough) and there is no shortness of breath, PSpO2 >93% without ventilator in room or if it is low, with other discharge criteria, the oxygen saturation level should be stabilized to an acceptable level (pSpO2 > 90%) for two to three consecutive days and should not decrease. Other vital signs of the patient are stable at the discretion of the attending physician.
The following criteria is for better decisions about discharge from general awards:
CBC is normal before discharge; CRP is at least 50% and ESR is at least 20% lower than before.
In cases where a CXR / CT scan was requested due to the severity of the symptoms, the previous imaging findings were reduced and no new lesions were created.
The patient does not need intravenous therapy.
The following criteria are considered for the discharge of hospitalized patients from intensive care unit (ICU):
COVID-19 patients are discharged with the opinion of the intensive care specialist or anesthesiologist with the following conditions:
Improvement in respiratory distress and oxygenation paO2 above 60 mm Hg and PACO2 below 50 mm Hg without the need for respiratory support
Improvement in new arrhythmia and eliminate the need for cardiovascular support with MAP above 60 mm Hg, without the need for inotropic and vasopressor support, accurate ECG and hemodynamic monitoring
Improvement of organic disorders and systemic infections and the absence of metabolic acid and base metabolic disorders
Echo test
All patients underwent a single transthoracic echocardiogram (TTE), to evaluate left and right ventricular function, left ventricular diastolic function and left ventricular global longitudinal strain (GLS). All echocardiograms were performed by two experienced certified sonographers. All measurements were performed according to EACVI (European Association of Cardiovascular Imaging) recommendations for cardiac chamber quantification.
In case of poor image quality, Simpson's biplane LVEF was measured, or LVEF was estimated by eyeball assessment. Left ventricular dysfunction was defined as LVEF below 52% and/or GLS worse than − 18%. Right ventricular dysfunction was defined as a tricuspid annular plane systolic excursion (TAPSE) < 17 mm and/or a right ventricular systolic excursion velocity (RV S’) <10 cm/s. 16 Impaired LVEF was defined as a systolic ejection fraction ≤ 50%. RV-function was determined by visual assessment, measurement of TAPSE, and right ventricular fractional area change (RV-FAC). TAPSE ≥ 20 mm was considered as an indicator for normal RV-function. Right ventricular dysfunction was considered present when RV-FAC was < 35%. Mitral regurgitation was determined by left atrium jet area and width of vena contracta. pressure half time (PHT) was determined using jet/left ventricular outflow tract (LVOT) width, diastolic flow reversal in proximal descending aorta. 17
Pulmonary function testing
Spirometry was performed by a physician based on the ATS criteria (American Thoracic Society), two hours after breakfast. On the same day, a spiral chest CT scan was performed using Siemens 16-slice device by a radiology technician in accordance with the safety principles of standard of the Radiology and Radiation Hygiene Association. Spirometry was interpreted by a pulmonologist and CT scan was performed by a licensed radiologist. Data were collected in a questionnaire based on a table of variables.
Laboratory tests
The routine laboratory tests including biochemistry, coagulation function, and infection biomarkers were performed in each patient after admission.
Clinical follow-up
The patients were called to Baharloo hospital three months after recovery and were examined for cardiac, pulmonary and labratory tests, and the results were recorded in checklists.
All the mentioned evaluations were performed with same tools and specialists. Thus, to perform initial evaluation of patients and follow-up session same electrocardiographs, echocardiographs, spirometers, CT scans, and laboratory tests were used.
Ethics statement
Considerations related to the well-being of the human subject took precedence over the interests of science and society. The research protocol contains a statement of the ethical considerations and indicated that there is compliance with the principles enunciated in this Declaration. All medical evaluations performed by scientifically qualified technicians and under the supervision of clinically qualified physicians. All precautions were taken to protect the patient's privacy, the confidentiality of the patient's information and to minimize the impact of the study on the subject's physical and mental health and on the personality of the patients. Written informed consent was obtained from all eligible patients before enrollment in our study. The patients informed of the right to abstain from participation in the study or to withdraw consent to participate at any time without reprisal. The study was approved by Ethics Committee of Tehran university of medical sciences.
Statistical analysis
All statistical analyses were performed using SPSS version 26.0. Data were compared using paired sample T test. Quantitative variables were presented as mean ± standard deviation. Qualitative variables were presented as frequency and percentage. For missing data, replace missing values were determined.
Results
Our study included 178 participants with mean age of 55.70 and 50.6% of them were male. Patients mean hospital length of stay was 6.2
Baseline characteristics of the COVID-19 patients.

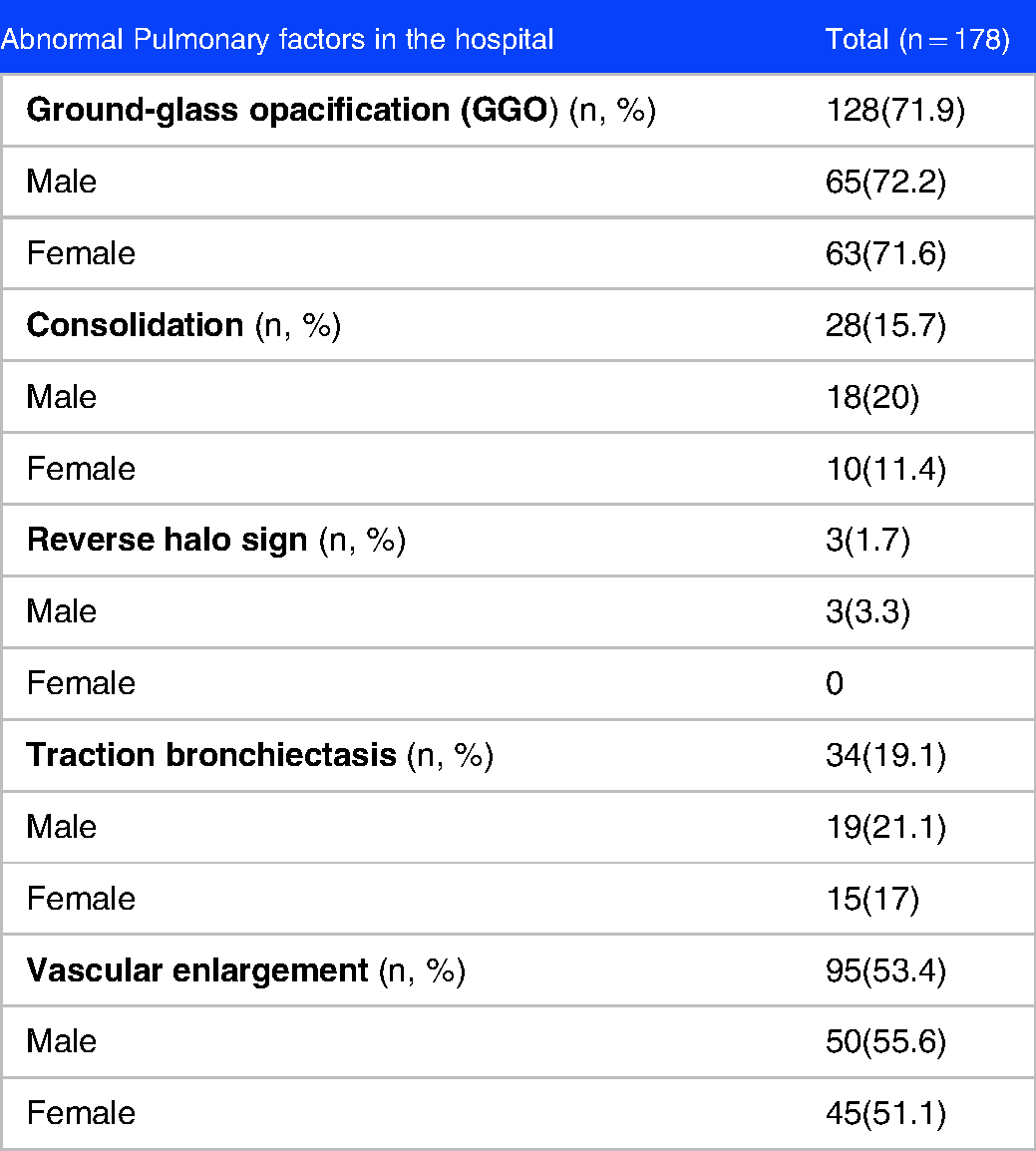
Among pulmonary factors in the hospital, 71.9%, 15.7%,1.7%,19.1% and 53.4% had positive GGO, consolidation, reverse halo sign, traction bronchiectasis and vascular enlargement, respectively. (Table 2)
Pulmonary factors of the COVID-19 patients in the hospital.
After three months follow up, percentage of patients who had reticulation, honeycombing, fibrotic brand and bullae were 12%, 1.1%,8.4% and 0%, respectively. (Table 3) Also, Mean of FVC and FEV1 was 4.21 and 3.01 respectively. (Table 4)
Pulmonary factors of the COVID-19 patients three month after discharge.

Proportion of vital capacity of COVID-19 patients (Total n = 178, Male = 90, Female = 88).

Among Cardiac factors positive PVC, PAC and mean Pap was decreased after three month follow up and these was statistically significant. Normal axis, positive ischemic changes, positive RWMA and normal RV function didn't change after three months. Also, normal rhythm, mean EF and positive VDH was increased after three months. (Table 5)
Cardiac factors of COVID-19 patients.

No patients had Aneusomy and Olfactory disorder. Complications such as myalgia, decreased sense of smell and decreased sense of taste increased after three months follow up. Only Growth in myalgia and decreased sense of taste was statistically significant. Only one patient had taste disorder after three months. (Table 6)
Complications following COVID-19 infection.

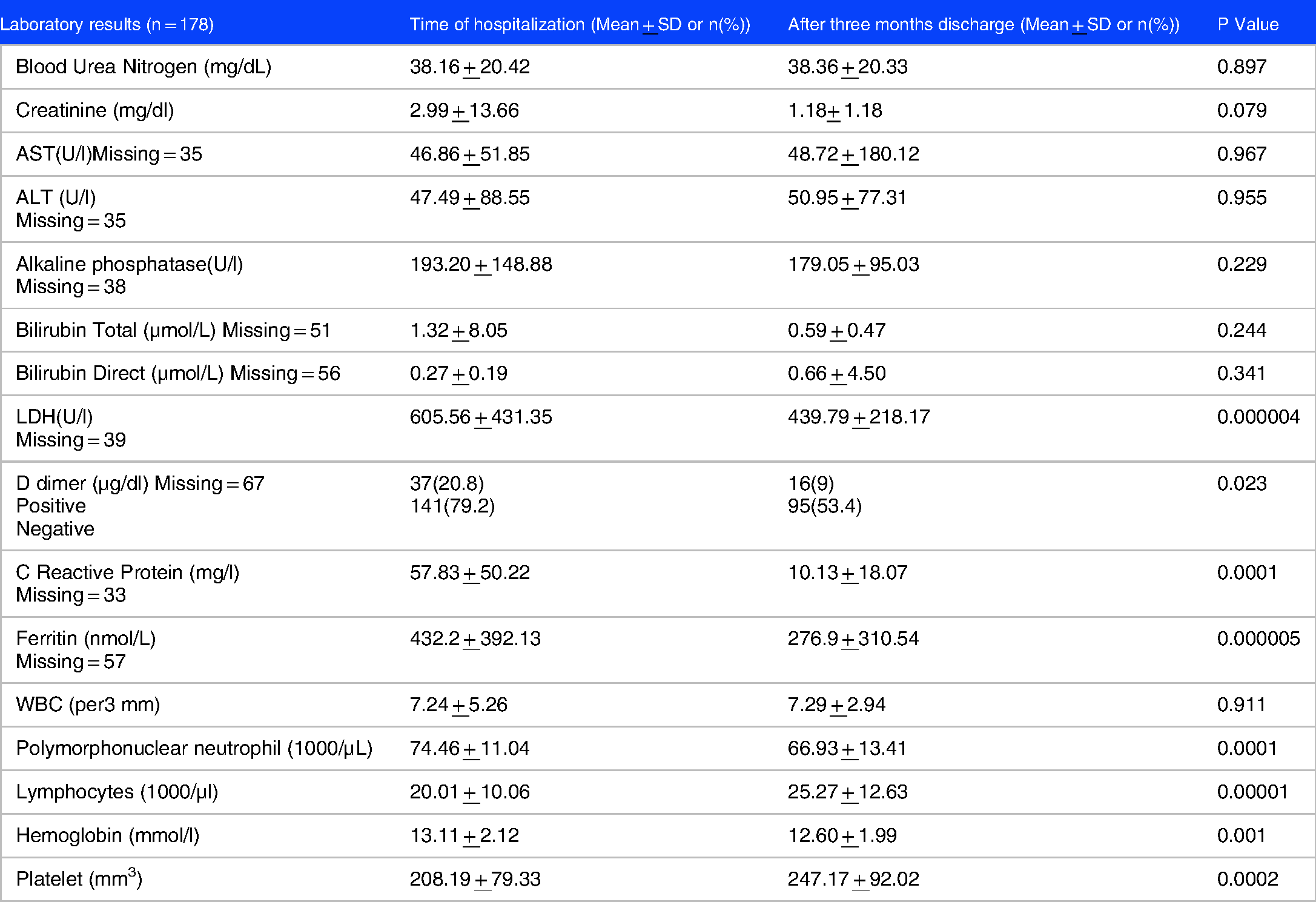
Among patient's laboratory results BUN, CR and WBC did not change significantly after three months follw up. In addition, D dimer, UA protein, PMN, Ferritin CRP, PMN, LDH and HB amounts had decreased significantly. Also means of LYMPH, and PLT had increased significantly. (Table 7)
Laboratory results of COVID-19 patients.
Discussion
As COVID-19 pandemic started, many people infected and convalesced from the disease. The patient's clinical sequelae were always an important issue for clinicians and healthcare workers. A combination of symptoms that are often reported after recovering from COVID-19 called Post COVID-19 sequelae. A better understanding of the clinical spectrum and long-term effects of COVID-19 is needed. 18
In our prospective cohort study on survivors of COVID-19 in Baharloo hospital, we found that among pulmonary factors in the hospital, 71.9%, 15.7%, 1.7%, 19.1% and 53.4% had positive GGO, consolidation, reverse halo sign, traction bronchiectasis and vascular enlargement, respectively. After three months follow up, percentage of patients who had reticulation, honeycombing, fibrotic brand and bullae were 12%, 1.1%, 8.4% and 0%, respectively. Mean of FVC and FEV1 was 4.21 and 3.01, respectively. Among Cardiac factors positive PVC, PAC and mean Pap was decreased after three month and these was statistically significant. Also, normal rhythm, mean EF and positive VDH was increased after three months. Only Growth in myalgia and decreased sense of taste was statistically significant. D dimer, UA protein, PMN, Ferritin CRP, PMN, LDH and HB amounts had decreased significantly. Also means of LYMPH, and PLT had increased significantly.
Most of the articles included in the discussion did not mentioned the discharge criteria of COVID-19 patients. Those that mentioned these criteria19,20 were same as our criteria except one factor that is two consecutive negative COVID-19 nucleic acid detection at least 24 hour apart. In Baharloo hospital, RT-PCR is not one of the prerequisites for COVID-19 discharge, but according to the facilities and conditions of patients and the place of care after discharge, it may be recommended (patients with underlying immunodeficiency and patients who need to be transferred to long-term care units).
Sometimes the hospital discharge criteria are not same in different regions, because health authorities consider many factors such as capacity of the healthcare system, laboratory diagnostic resources, and the current epidemiological situation. 21 According to the Centers for Disease Control and Prevention, meeting criteria for discontinuation of transmission-based precautions (TBP) is not a prerequisite for discharge. 19
The first study that investigate the long-term effects of COVID-19 on changes in pulmonary function three months after their hospital discharge, was Yu-miao Zhao et al study. Different degrees of radiological abnormalities were detected in 39 patients. Lung function abnormalities were detected in 14 patients. Higher level of D-dimer on admission could effectively predict impaired DLCO after three months discharge. Their mean age was 47.74, among which 41.82% were female. The patients in this study are younger and the female percents is more than our study. 22
Ground glass opacities are the most common CT findings within 0–3 days of symptom onsets of COVID-19. Over time, GGO remains a common finding and consolidation increase. These two symptoms mean the disease is progressing rapidly. 23 In our result 71.9% had abnormal GGO. Several previous studies Similar to our study have described the main CT signs of COVID-19, summarized as GGO and consolidation.24,26
Diffuse alveolar damage is a hallmark of ARDS (acute respiratory distress syndrome). 27 VES (vascular enlargement sign) on thoracic CT was found in almost two-thirds of COVID-19 patients, which plays an important role in development of pneumonia caused by coronavirus. 28 In our study, 50% of people had vascular enlargement, and the findings confirm previous studies. In M Liu et al study, a total of 41 COVID-19 survivors (male: 22, female: 19) were enrolled in the study, including 26 patients of moderate type and 15 patients of severe type. In our study all of patients had severe type. the predominant CT patterns of abnormalities observed at 7 months after discharge were interlobular septal thickening (32%) and traction bronchiectasis (29%). Traction bronchiectasis on chest CT, and opacity score at discharge, were independent risk factors for developing pulmonary fibrosis at 7 months after discharge.. 20 In our study 19.1% of patients had traction bronchiectasis in hospital and after three months of follow up 12.4% had reticulation, %8.4 had fibrotic band and 1.1% showed honeycombing signs, respectively. As our result also showed , development of honeycombing is very rare. Fibrotic changes without honeycombing are the most common CT finding. 29 In our pulmonary result the least common finding was honeycombing. The residual pulmonary fibrosis in COVID-19 survivors after discharge depends on many factors such as patient's age, CT severity, consolidation/crazy-paving scores, and ICU admission. 30 This may be the reason for the difference in the percentages of pulmonary results of our study with other studies.
In Fumagalli et al study baseline pulmonary function tests were 55.7 ± 15.6 for FEV1%, 68.6 ± 16.0 for FVC%, and 1.2 ± 0.1 for FEV1/FVC%. Although pulmonary function showed a small improvement after 6 weeks, patients experienced a more significant improvement after 6 and 12 months in FEV1% (95.4 ± 13.7 and 107.2 ± 16.5), FVC% (91.3 ± 14.5, and 105.9 ± 15.6), and FEV1/FVC% values (1.04 ± 0.04, and 1.01 ± 0.05). 13 patients enrolled in the study were aged 57.8 ± 10.0 years, almost exclusively male. 31
In B Kerget et al study 60 patients enrolled in the study. Mean age of the patients was 51.4 ± 18.2 years. Forty-two (70%) of the patients were men and 18 (30%) were women. FEV1 and FVC values on day 7 were significantly higher than those at admission. FEV1 and FVC values were lower than expected in 76.3% and 75.3% of the patients at admission, while these rates fell to 43.4% and 38.1% on day 7 of treatment, respectively. This study showed that COVID-19 patients’ CRP, ferritin, and fibrinogen levels decreased with treatment, consistent with previous studies, while FEV1 and FVC values increased. 32
In Lassen et al study, from 215 patients mean age of the study sample was 63 ± 12 years and 59% were male. Right ventricular (RV) function improved after recovering from COVID-19. TAPSE, and RV longitudinal strain (RVLS) (25.3 ± 5.5% vs 19.9 ± 5.8%), did not significantly improve.. 33 Impaired left and right-ventricular function were significantly associated with higher mortality. 17
On admission ECG, patients with poor outcomes tend to have a longer QTc interval, more frequent prolonged QTc interval, longer QRS duration, faster heart rate, higher incidence of PAC, PVC, T-wave inversion. 34 In Mahmoud-Elsayed study, RV impairment was associated with increased D-dimer and C-reactive protein levels. The main abnormalities were right ventricle (RV) dilatation (41%) and RV dysfunction (27%). In contrast, in one study included adults 18 years or older with COVID-19 pneumonia who underwent TTE left ventricular function was normal in most (89%) patients. In this study like ours most patients had severe type 1 respiratory failure requiring mechanical ventilation with more than half requiring vasopressor support during admission. 35
Shivdas Naik et al reported that of 1234 patients, most common symptoms included myalgia (10.9%), fatigue (5.5%), shortness of breath (6.1%), cough (2.1%), insomnia (1.4%), mood disturbances (0.48%) and anxiety (0.6%). Median age of the patients was 63 years, 114 (31.2%) of the patients were smokers. Two hundred and nineteen (56.6%) were male. In our study, smokers were among the exclusion criteria. 36 In Penas et al study, from a total of 1200 hospitalized patients with COVID-19, a greater of patients with myalgia at hospital admission (20%) showed post-COVID symptoms. A higher proportion of patients presenting myalgia exhibited musculoskeletal post-COVID pain when compared to those without myalgia. 37
Sense of taste loss(STL) is a common symptom in COVID-19 and may be the first and/or only symptom of this disease. In Erdal Sakalli et al study eighteen (22.2%) patients with loss of sense of smell showed no improvement 20 days after diagnosis. A total of 63 (77.8%) patients described improvement in loss of sense of taste within 20 days, with 17 (21.0%) patients showing mild recovery, 27 (33.3%) patients showing moderate recovery, and 19 (23.4%) patients showing complete recovery. The average time for recovery of the sense of taste was 8.20 ± 7.07 days. 38
A few studies have conducted on LYMPH and PLT assessment among recovered COVID-19 patients. Wen et al study found that COVID-19 patients are still vulnerable after hospital discharge because T cells decreased remarkably, whereas monocytes increased in patients in the early recovery stage (ERS). 39 Yip et al conducted a cohort study of 76 patients with COVID-19 in three tertiary hospitals of the National University Health System study. The lymphocyte count was significantly lower in the severe infection and then, observed that the rise in AS-Lymph pre-dated clinical recovery in several patients. 40 These findings are similar to our result. This is still unclear if lymphocytes are protective or immunopathogenic. Recovery is associated with formation of T cell memory that can consider as a biomarker for disease outcome and control. 41 In a meta-analysis of nine studies, a total of 1779 patients with COVID-19, found that platelet count was significantly lower in patients with more severe COVID-19. 42 Platelets have immunomodulatory activity. 43 Platelets can also mediate a response to various RNA viruses such as COVID-19 44 and lead to thrombotic vascular occlusion.45,47 Patients with mild symptoms have a slightly increased platelet count, whereas thrombocytopenia is a hallmark of severe COVID-19 infections. 48 So, it seems that because of this point, number of platelets increased three months after recovery in our result.
One of the limitations of this study was that we assumed our patients did not have any cardiovascular or pulmonary diseases prior to the COVID-19 infection. Another limitation was that we excluded smokers from the study.
Conclusion
Our study indicated that myalgia and decreased sense of taste complications and from laboratory result, LYMPH, and PLT had increased significantly after three months follow up. Also, GGO and Vascular enlargement are the most common pulmonary sign, and honeycombing and Bullae are very rare. Among cardiac factors PVC, PAC and Pap increased after three months follow up.
Footnotes
Acknowledgments
We would like to thank hospital staff for collaboration and help.
Authors’ Contributions
Author 1: Conceived of the presented idea and supervised the project, verified the paper.
Author 2: Wrote the paper, preparing the final articles’ table and figures, conducted the analysis.
Author 3: Collected the data, contributed data or analysis tools, analyzed the data and prepare tables and figures.
Author 4: Collected the data.
Author 5: Collected the data, Wrote the paper.
Author 6: Collected the data, contributed data or analysis tools, Performed the analysis, Wrote the paper.
Author 7: Collected the data, contributed data or analysis tools.
Author 8: contributed data or analysis tools, analyzed the data.
Author 9: Conceived of the presented idea and supervised the project, verified the paper.
All authors discussed the results and contributed to the final manuscript.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
This article has ethics approval and consent from ethics committee of Tehran university of medical science.
Availability of Data and Materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].