
Abstract
Background
Heart transplant (HTX) recipients are at a significantly higher risk of adverse clinical outcomes, due to chronic immunosuppression and co-existence of other chronic conditions, when contracting the SARS-CoV-2 infection. Although vaccination against SARS-CoV-2 is currently the most promising measure for the prevention of severe Coronavirus Disease 2019 (COVID-19) among solid organ transplant recipients, the extent of immune response and its protective efficacy among patients receiving HTX has not been sufficiently studied.
Methods
We performed a systematic review of the literature by inquiring PubMed/Medline to identify original studies among HTX recipients, who had received at least one dose of the SARS-CoV-2 vaccine. Data on the measured humoral or cellular immune response was collected from all the eligible studies. Factors associated with a poor immune response were further investigated within these studies.
Results
A total of 12 studies comprising 563 HTX recipients were included. The average age of the study participants was 60.8 years. Sixty four percent of the study population were male. Ninety percent of the patients had received an mRNA vaccine (Pfizer/ BNT162b2 or Moderna/mRNA-1273). A positive immune response to SARS-CoV-2 vaccine was variably reported in 0% to 100% of the patients. Older age (> 65 years), vaccine dose (first, second, or third), time since HTX to the first dose of the vaccine, the time interval between the latest dose of the vaccine and measurement of the immune response, and the type of immunosuppressive regimen were all indicated as potential determinants of a robust immune response to the SARS-CoV-2 vaccination.
Conclusion
HTX recipients demonstrate a weaker immune response to the vaccination against SARS-CoV-2 compared to the general population. Older age, anti-metabolite agents such as mycophenolate mofetil, and vaccination during the first year following the HTX have been indicated as potential determinants of a poor immune response.
Keywords
Introduction
At the time of writing this article, 79,555,007 cases of coronavirus diseases 2019 (COVID-19) have been identified in the U.S. with a total of 968,839 reported deaths. 1 Additionally, 254,984,673 individuals have received at least one dose of a vaccine against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Despite declining trend in the number of new cases of COVID-19 and hospitalization rate, the number of patients with pre-existing comorbidities, who are at the risk of developing severe COVID-19 remains high. 2
In patients with COVID-19, the severity of the disease, worse clinical outcome, and mortality are correlated with the intensity of the hyper-inflammatory response in the form of a cytokine storm.3–5 Additionally, those with pre-existing comorbidities are at an additional risk for development of poor clinical outcome and mortality. 6
Heart transplant (HTX) recipients constitute a high-risk population of patients in the setting of COVID-19.7-9 In addition to harboring higher number of comorbidities, 10 HTX patients have a suppressed immune state, which has been a controversial risk factor for the development of more severe COVID-19 or poor clinical outcomes.7,8,11
At present, vaccination against COVID-19 is the only preventive measure to mitigate the severity of the diseases, reduce hospitalization rate and mortality, and ultimately end the pandemic.12-14 However, due to chronic immunosuppression and existence of multiple comorbidities, production of sufficient anti-SARS-CoV-2 spike immunoglobulin titer or effective neutralizing antibody after vaccination against COVID-19 has been variable among patients with a transplanted solid organ.15-21
As HTX patients constitute a unique population of transplant recipients, we aimed to conduct this systematic review to summarize scarce data in the literature on the development of immune response following vaccination against SARS-CoV-2 and factors associated with a weaker immunity.
Methods & Materials
Study design
A systematic review was conducted according to the Reporting Guidelines for Meta-analyses of Observational Studies (MOOSE). 22 Two reviewers (SS and GP) independently searched the literature to identify articles addressing SARS-CoV-2 vaccination in patients with HTX. Any conflict was resolved by discussing with the third investigator (MSA). The protocol for this systematic review has been registered with the Open Science Framework and is available to the public (DOI:10.17605/OSF.IO/HV4FJ).
Literature review
The literature review was performed by electronic query of the online database Medline/PubMed using the following combination of search terms: (COVID-19 vaccin* OR SARS-CoV-2 vaccin*) AND (Cardiac transplant* OR Heart transplant*). The title and abstract of the retrieved articles were reviewed for relevancy. The full text of relevant articles was further assessed for eligibility. The reference list of eligible studies and relevant review articles were also manually reviewed for additional citations.
Study selection
Studies were eligible if they were in English language, reported on human subjects older than 18 years, and measured the immune response to SARS-CoV-2 vaccination in HTX recipients. Studies were not eligible if they were animal experiments, editorial/commentary, or review articles. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 23 throughout the literature review and for study selection (Figure 1).
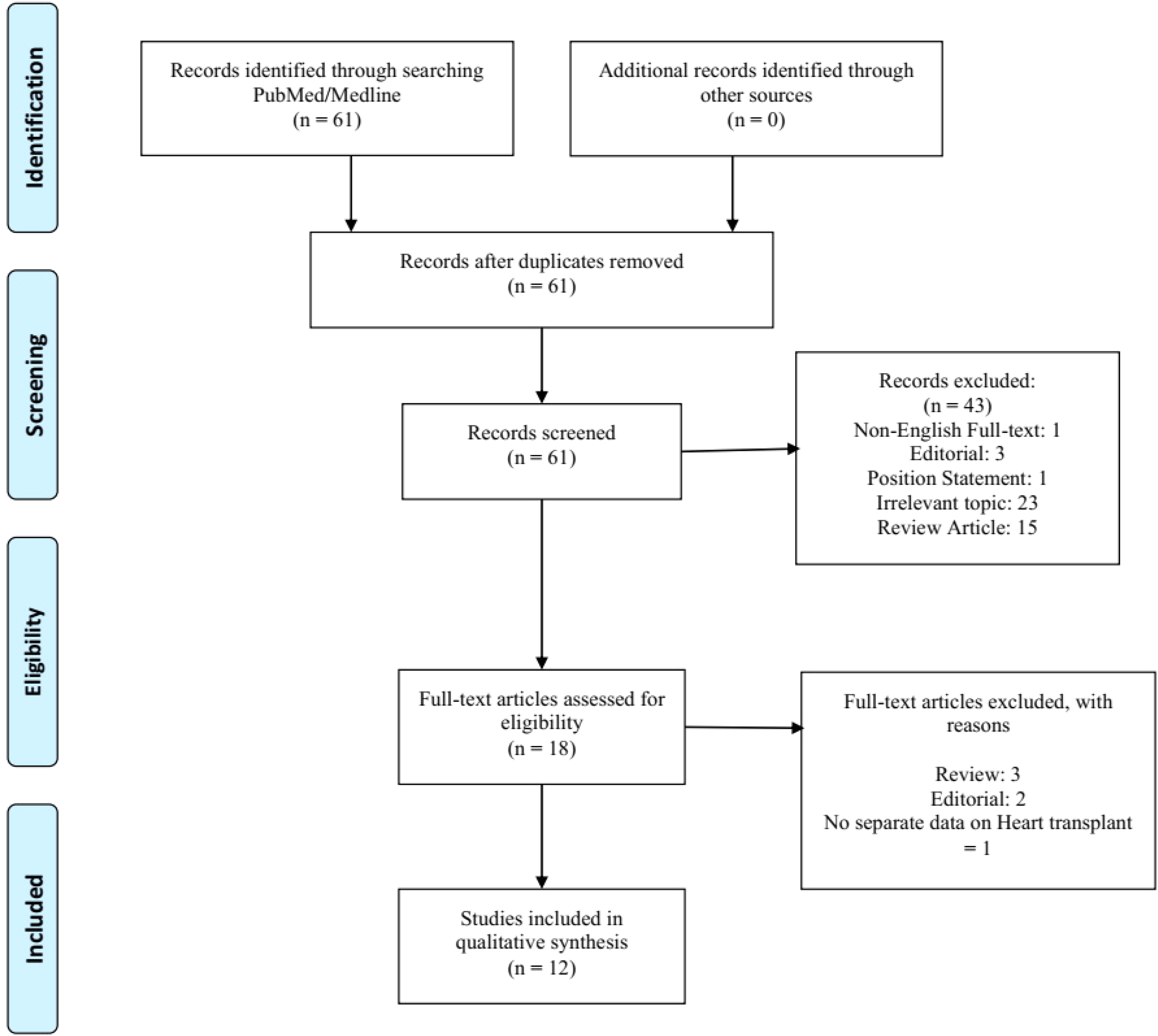
PRISMA flowchart demonstrating our step-by-step approach to the literature review, articles screening, and study selection.
Data collection
Data pertinent to the variables of interest was collected from eligible studies. This included age, gender, country of origin, features of COVID-19 vaccine such as type, dose, and time from the latest dose of vaccine to the time of measuring the immune response, time interval from HTX to the first dose of vaccine, immunosuppressive regimen, and the study conclusion on vaccine efficacy.
Outcome measure
The primary endpoint of this systematic review was to determine a detectable response rate to SARS-CoV-2 vaccine in HTX recipients. The secondary endpoint of this study was to elaborate on factors associated with a poor immune response.
Statistical analysis
Extracted data from eligible studies were examined by simple descriptive statistics and in a qualitative manner. Continuous variables are presented as mean ± standard deviation (±SD) or median [interquartile range]. Categorical variables are presented as percentages. Due to a small number of HTX cases and a large heterogeneity in the measurement and reporting of the data, a more vigorous statistical analysis was not feasible and hence not performed.
Results
A total of 61 records were identified through December 2021 by electronic inquiry of PubMed/Medline and manual search of the bibliography list of relevant review articles. The full text of 18 studies was further evaluated for eligibility. Of these, 12 articles were eligible to be included into this systematic review17-21,24-30 (Figure 1). This encompassed a total of 563 HTX recipients with an average age of 60.8 years (range: 18-80), who received at least 1 dose of SARS-CoV-2 vaccine. Out of the studies with a reported gender distribution (496 patients),17-20,24-28,30 319 were male (64.3%) and 177 were female (35.7%). The patient population enrolled in these studies were from Israel,24,26-28 Europe (Italy, Spain, Germany, and Greece),17,19-21,29 Taiwan, 30 and the USA18,25 (Table 1).
Characteristics of studies included in our systematic review.

M:F: Male to female ratio; HTX: Heart transplantation; RBD: Receptor binding domain; N/A: Not applicable;
[] refers to 95% confidence interval;
The utilized vaccines for the immunization of HTX recipients against SARS-CoV-2 were Pfizer/BNT162b2 (449 patients, 79.7%),17,18,20,21,24-29 Moderna/mRNA-1273 (122 patients, 19.9%),18,19,25 Johnson & Johnson/Ad26.COV2.S (1 patient, 0.2%), 25 and AstraZeneca/AZD1222 (ChAdOx1 nCoV-19) (1 patient, 0.2%). 30 Immune response was measured after the second dose of an mRNA vaccine in 464 patients (82.4%),17,18,20,21,24-29 after the third dose of an mRNA vaccine in 96 patients (17.05%), 26 after the first dose of an mRNA vaccine in 1 patient (0.17%), 17 and after the single dose of the vector-based vaccine in 2 patients (0.35%).25,30
Time to administration of the first dose of COVID-19 vaccination ranged from 8 days before 17 to more than 166 months after HTX 24 (Table 2). Time from the last dose of the vaccine (first, second, or third) to the time of the last measurement of the immune response ranged from 9 days 21 to 10 weeks. 25
Features of antibody response in patients with heart transplantation.
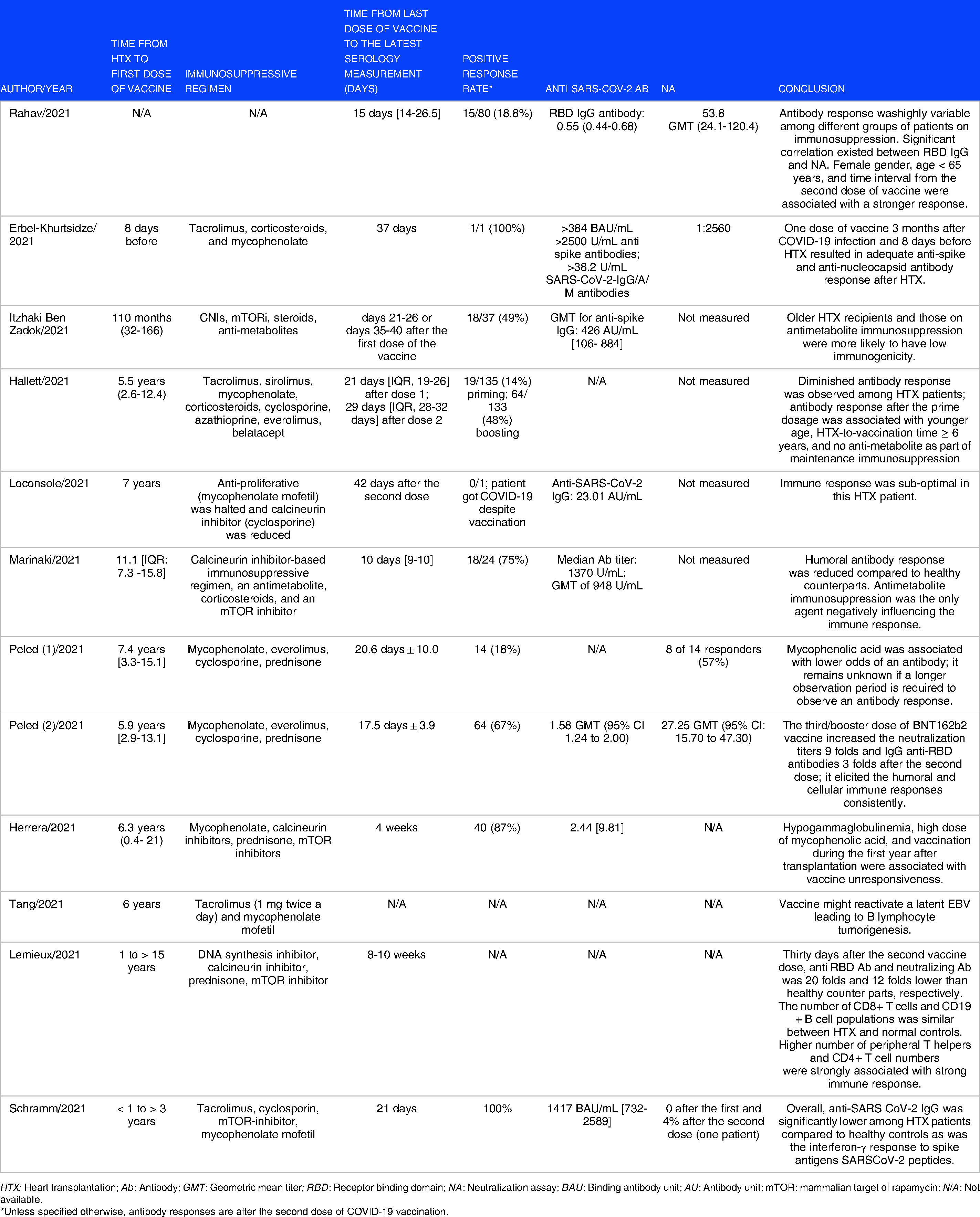
HTX: Heart transplantation; Ab: Antibody; GMT: Geometric mean titer; RBD: Receptor binding domain; NA: Neutralization assay; BAU: Binding antibody unit; AU: Antibody unit; mTOR: mammalian target of rapamycin; N/A: Not available.
*Unless specified otherwise, antibody responses are after the second dose of COVID-19 vaccination.
Studies included in this systematic review utilized a combination of humoral and/or cellular immunoassay in measuring the immune response against SARS-CoV-2 vaccine among HTX recepients. This included anti-receptor binding domain (RBD),18-21,26-28 anti-spike,17,18,24 or anti-nucleocapsid antibody levels 17 (measured as a titer or as a positive response rate), neutralization17,26 or pseudo-neutralization activity25,27,28 of anti-SARS-CoV-2 antibodies, interferon-γ assay,19,29 and peripheral T-cell counts or its subsets (CD4 + and CD3 + cells). 25
Regardless of the laboratory test, immune response (humoral or cellular), or the manufacturer-provided cut-off for the detection of an immune response, a positive response was variably observed in 0% to 100% of the HTX recipients. Based on a qualitative appraisal of the included studies, a weaker immune response was implicated in relation to an age > 65 years,24,28 male gender, a short time interval between the second dose of the SARS-CoV-2 vaccine and the time of measuring the immune response, 28 vaccination within the first year after HTX, antimetabolite immunosuppressant,19,21,24,27 and a weaker cellular immune response.25,29
Discussion
Our systematic review and qualitative analysis of the literature on the immune response to SARS-CoV-2 vaccination observed a weaken humoral immune response among HTX recipients. Although more studies are required, older age, antimetabolite immunosuppressants, and vaccination within the first year of HTX seemed to be associated with a weak immune response to SARS-CoV-2 vaccine. Yet, no study has demonstrated an association between race, or socioeconomic status, and the strength of the immune response.
In a prospective cohort of 658 solid organ recipients, Boyarsky et al. measured the humoral response against RBD of the SARS-CoV-2 spike protein after the first and second dose of the vaccine. 16 At a median (IQR) of 21 (18-25) days after the first dose, 15% of the patients developed a positive response while the positive response rate was 54% at a median (IQR) of 29 (28-31) days after the second dose. On the opposite, 46% of the patients did not develop any antibody response after SARS-CoV-2 vaccine dose 1 or 2. Out of those receiving antimetabolite immunosuppressants, 8% developed a humoral response to the first or the second dose compared to a 32% response rate in those receiving an immunosuppressant regimen besides antimetabolites. Although sex and race did not demonstrate any significant association with the response rate after either dose of the vaccine in this study, older age and shorter time interval since HTX were all associated with a higher probability of a weaken response to the SARS-CoV-2 vaccine. Interestingly, an enhanced response rate for humoral immunity after the second dose was noted among the middle-aged group (40-59 years), and in those who were 7 years and longer beyond HTX.
Erbel-Khurtsidze et al. presented a case with a robust immune response to one dose of SARS-CoV-2 vaccine, 3 months after contracting the SARS-CoV-2 infection and 8 days prior to receiving the HTX. 17 However, it is noteworthy that both events, infection and vaccination, occurred prior to the HTX and initiation of the induction immunosuppression. In a cohort of 96 HTX recipients receiving 3 doses of SARS-CoV-2 vaccine, Peled et al. demonstrated a significantly higher rate of humoral and cellular immune response to SARS-CoV-2 vaccine after the third dose. 26 Still, there was no humoral response in 33% of the HTX recipients. Younger age, stronger renal function, use of mycophenolate as the antimetabolite immunosuppression, and lower serum levels of C-reactive protein were significant predictors of a positive antibody response. Interestingly, a positive T-cell response was observed in the majority of HTX recipients following the third dose of SARS-CoV-2 vaccine in the absence of a positive humoral/antibody response, suggesting a positive cellular immunity despite no antibody response. In another prospective study of 50 cardiothoracic transplant recipients, Schramm and colleagues measured the immune response to a full-dose BNT162b2 vaccine 10 to 36 months after HTX and compared it to healthy individuals. 29 In contrast to 98% response rate in healthy individuals after the first dose, only 10% of the HTX recipients had a positive humoral or cellular immune response three weeks after the two-dose series of the vaccine. Such a poor immune response might be explained, in part, by shorter time interval after transplantation as all the patients were in their second to third year post-HTX. Although there was no significant difference between responders and non-responders to the third dose of SARS-CoV-2 vaccine in terms of the time after HTX in the study of Peled et al., 26 such a time interval was significantly shorter among solid organ recipients in the study of Boyarsky et al. 16 Besides an additional boosters given to the transplant patients in the former study, 26 all were HTX recipients, compared to the latter in which a combination of heart, lung, kidney, liver, and pancreas had been transplanted. 16
The variation in the response rate to SARS-CoV-2 vaccine among HTX recipients can be, in part, explained by the different time interval from the latest dose of the vaccine to the time of serological testing.17,25 In a serological assay of 34 healthcare workers, who had received two doses of Pfizer/BNT162b2 in three weeks interval, Mueller et al. demonstrated that while anti-nucleocapsid antibody titer remained undetectable over a 5-week observation period, the anti-spike antibody constantly rose up 4 to 5 weeks after the first dose of the vaccine. 31 A similar pattern of rapid increase in anti-SARS-CoV-2 antibody levels has been also observed in the plasma obtained from US donors, from a mean of 21 IU/mL in December 2020 to 506 IU/mL in June 2021. 32
A prior history of COVID-19 prior to either dose of SARS-CoV-2 vaccine might have an impact on the robustness of the immune response among HTX recipients.17,25 In a case-control study of 26 heart/lung transplant recipients and 12 healthy controls, Lemieux et al. demonstrated a robust anti-RBD IgG response among the control group compared to a minimal response by heart/lung transplant recipients. 25 However, those heart/lung transplant recipients with a history of COVID-19 prior to SARS-CoV-2 vaccination showed a comparable immune response to the healthy controls. While dysregulation of the immune system has been proposed as an underlying mechanism for a variable response to vaccination against COVID-19 in patients with a prior history of SARS-CoV-2 infection, time interval between the infection and vaccination seems to play a pivotal role in the strength of the immune response. 33
Currently, several SARS-CoV-2 antibody tests manufactured by different research and commercial laboratories have received an emergency use authorization (EUA) from the United States Food and Drug Administration (FDA). 34 Besides different techniques employed by these serological tests (Enzyme-linked immunosorbent assay [ELISA], Chemiluminescence Enzyme Immunoassays [CLIA], Fluorescence Immunoassays [FIA], and the Lateral Flow Immunoassays [LFIA]), targets (spike protein, receptor binding domain [RBD], and nucleocapsid), and antibody function (immunoglobulin [Ig] A, M, and G titer or neutralizing activity) measured by these tests also vary. Studies included in this systematic review utilized a combination of these humoral and/or cellular immunoassay in measuring the immune response against SARS-CoV-2 in HTX patients.
An analysis of the electronic medical records of older US veterans, who had been vaccinated against SARS-CoV-2 between February 1stand September 30th, 2021 revealed that immunization with Moderna and Pfizer-BioNTech vaccines stays effective, 120 days after the second dose, in the prevention of hospitalization due to COVID-19, in 86% and 75% of the cases, respectively. 35 This study included an older population of patients with multiple underlying comorbidities. Other studies have also indicated that an age > 65 years old and existence of comorbidities such as diabetes, chronic renal diseases, autoimmune and/or rheumatologic conditions, and malignancy are associated with a weaker immune response, an observation that is forming the evidence for current recommendation for booster doses.2,33,36,37 As these conditions are more prevalent among HTX recipients, the waning immunity in these patients after a series of vaccination against COVID-19 remains to be investigated by longitudinal studies. Of note, while humoral response is an important measure of immunity in the short run, cellular immunity plays a more important role when assessing the long-lasting protection against SARS-CoV-2. 33
A case-control study among hospitalized adults aged ≥ 18 years after completing a series of vaccination with one of the 3 commercially available SARS-CoV-2 vaccines in the US showed an efficacy rate of 93% with the Moderna vaccine in the prevention of hospitalization due to COVID-19 followed by 88% with the Pfizer-BioNTech and 71% with the Janssen/Ad26.COV2 vaccines. 38 Although anti-RBD and anti-spike IgG levels were significantly higher with the mRNA vaccines than that with the adenovirus type 26 (Ad26) vector vaccine, the protective efficacy declined 4 months after the last dose of the vaccine. Nevertheless, this study had excluded those cases with a known underlying immunocompromised condition, precluding its generalizability to solid organ transplant recipients such as HTX patients included in this systematic review.
The goal of immunosuppression in HTX patients is to prevent or treat allograft rejection. In this context, immunosuppression is divided into induction and maintenance regimens, which utilize interleukin-2 receptor antagonists, polyclonal anti-thymocyte antibodies, calcineurin inhibitors (tacrolimus and cyclosporine), antimetabolites or antiproliferative agents (azathioprine, mycophenolate mofetil, and mycophenolate sodium), proliferation signal inhibitors or mammalian target of rapamycin (mTOR) inhibitors (sirolimus and everolimus), and glucocorticoids. 39 There is a paucity of knowledge on the immunogenicity of SARS-CoV-2 vaccination in immunocompromised individuals including solid organ recipients (especially HTX patients) due to their exclusion from the flagship clinical trials.40-42 However, as elaborated in this systematic review, the immune response following any doses of SARS-CoV-2 vaccine has been sub-optimal among HTX recipients, especially in older patients within the first year of transplantation, and due to the use of an antimetabolite as an immunosuppressive agent. Whether a more aggressive approach is required and will be beneficial to immunize these vulnerable patients remains within the scope of future studies. Additionally, as more data is being published on the durability of immunity among patients with a prior dose of COVID-19 vaccine, a better understanding will be achieved for optimal scheduling of booster doses among HTX patients. Ideally, such information will arise from studies exclusively on immunocompromised patients so as to make the conclusion applicable to HTX recipients.
Limitations
Although this is the first systematic review summarizing available studies on the immune response to SARS-CoV-2 vaccine among HTX recipients, it harbors several limitations, mainly inherent to the current literature. A large body of the literature on immunization of HTX recipients comprises of case reports or case-control studies because SARS-CoV-2 clinical trials have excluded patients receiving cytotoxic or immunosuppressive regimens. Additionally, due to smaller sample size and retrospective methodology, the laws of cause and effect cannot be reliably investigated for a weaken immune response to the SARS-CoV-2 vaccine. This is especially true when the population of HTX recipients in either of these included studies are heterogeneous and of varying demographics, socioeconomic status, and clinical condition, which make the pooled analysis unfeasible. Finally, as the endpoint of most studies was quantification of antibody levels following immunization against SARS-CoV-2, they have fallen short at demonstrating the vaccine efficacy in the prevention of severe cases of COVID-19. Also, with evolving guidelines for booster vaccinations among immunocompromised patients, eyes will be on future studies to demonstrate the efficacy of additional doses of COVID-19 vaccine in eliciting a more robust immune response among HTX recipients. Such an endpoint needs to be compared to the general population in terms of infection rate by SARS-CoV-2, ICU admission, and mortality rate especially in the context of a deescalating pandemic.
Conclusion
This qualitative systematic review of the literature on the immune response to SARS-CoV-2 vaccine among HTX recipients observed that older age, being within the first year after the transplant, and use of antimetabolite as an immunosuppressive agent are implicated as potential factors associated with a weaken immune response. Cellular and humoral immunity seem to mount in parallel after vaccination against SARS-CoV-2, with a strong cellular response paving the way for a stronger humoral immunity.
Footnotes
Acknowledgements
We would like to extend our great appreciation to Ms. Lisa M. Parker for her extensive effort in reviewing this manuscript for language proficiency.
None of the authors received any financial support in any form.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.