
Abstract
Introduction
Submaximal exercise gas exchange may be a useful tool to track responses to therapy in pulmonary arterial hypertension (PAH) patients.
Methods
Three patients diagnosed with idiopathic PAH, on differing therapies, were included. Standard clinical tests (echocardiography; 6 minute walk) were performed pre and 3-5 months after treatment. Gas exchange was measured during 3 minutes of step exercise at both time points.
Results
Gas exchange variables, end tidal CO2 (PETCO2) and the ratio of ventilation to CO2 production (VE/VCO2), during submaximal exercise were able to track patient responses to therapy over a 3-5 month period. Two patients demonstrated positive improvements, with an increased PETCO2 and decreased VE/VCO2 during light exercise, in response to an altered therapeutic regime. The third patient had a worsening of gas exchange (decreased PETCO2 and increased VE/VCO2) following no changes in the medical regime from the baseline visit.
Conclusion
Gas exchange variables measured during light submaximal exercise, such as PETCO2 and VE/VCO2, may be able to better detect small changes in functional status following treatment and could, therefore, be a useful tool to track disease severity in PAH patients. Further study is required to determine the clinical usefulness of these gas exchange variables.
Introduction
Although the 6 minute walk test is simple and widely employed to assess submaximal exercise capacity and response to therapy in pulmonary arterial hypertension (PAH), it provides limited information. 1 Maximal cardiopulmonary exercise testing (CPET) can provide more comprehensive physiologic information, but is less widely available, is subject to varying interpretation across centers, and may be inconvenient for patients to perform. Submaximal exercise gas exchange measurement, using simplified technology (ie, ‘plug and play’ systems), 2 may be a simple alternative to formal CPET that could provide information beyond that available from a 6 minute walk.
Methods
Three patients diagnosed with idiopathic pulmonary arterial hypertension were included in the present report. Each patient was seen twice in the PH clinic, with the visits separated by approximately 3-5 months. As part of their assessments standard clinical tests were performed, which included a transthoracic echo and 6 minute walk test, at both visits. In addition, submaximal exercise step tests were performed in conjunction with clinical tests, which consisted of 2 minutes rest, 3 minutes exercise and 1 minute recovery. Gas exchange was measured throughout using a SHAPE gas analysis system (SHAPE Medical Systems Inc, St. Paul, MN). The SHAPE system is a newly designed, small and portable gas analysis system that is self calibrating, containing built-in automated temperature, barometric pressure and humidity corrections. The interface is simplified and the software designed so that extensive understanding of the methodology and equipment is not required (Fig. 1). 2

A SHAPE system which consists of a gas analyser, laptop, mouthpiece and pneumotach appliance and finger pulse oximeter.
Case Descriptions
Patient A
A 29 year old female evaluated for syncope was diagnosed with idiopathic PAH following right heart cath-eterization in December 2009. The pulmonary artery pressure at catheterization was 69/29 with a mean pulmonary arterial pressure (PAPm) of 45 mmHg, right atrial pressure (RAP) 5 mmHg, pulmonary wedge pressure (PCW) 5 mmHg, cardiac output (Q) 4.0 L/min, cardiac index (QI) 2.52 L/min/m2 and pulmonary vascular resistance (PVR) 10.0 Wood units. The patient was subsequently started on combination therapy, consisting of sildenafil (Revatio®) 20 mg tid and inhaled trepostinil sodium (TYVASO®) titrated to 9 breaths qid, and re-assessed approximately 3 months later.
Patient B
A 56 year old female who was first diagnosed with idiopathic PAH in September 2004. It is possible she may have hereditary hemorrhagic telangiectasia based upon frequent nosebleeds but without other diagnostic features. Continuous prostanoids seemed contraindicated because of thrombocytopenia, and acquired Von Willebrands disease. Most recent right heart catheterization from June 2009 demonstrated a pulmonary artery pressure of 133/40 with a PAPm 78 mmHg, RAP 11 mmHg, PCW 10 mmHg, cardiac output 3.5 L/min with QI 2.09 L/min/m2 and PVR 19.6 Wood units. The patient had been on various therapeutic regimes but when seen in the PH clinic in February 2010 was functional class III on combination therapy, consisting of bosentan (Tracleer) 125 mg tid and iloprost (Ventavis) Solution for Nebulization 10 ug/1 ml by inhalation 6-7 times daily, and had been on this medication for approximately 2 years. The patient remained on the same therapy and returned for re-assessment 5 months later.
Patient C
A 56 year old male was first diagnosed with PAH in 2005 in the context of prior splenectomy and was subsequently started on sildenafil (Revatio®) 20 mg tid in March 2006. The patient remained on this therapy until his visit to the PH clinic in March 2010, when the dose of sildenafil (Revatio®) was increased to 40 mg tid because the patient still had exercise limitations that impaired quality of life. Prior to the dose increase the patient had a right heart catheterization and had a pulmonary artery pressure of 78/21 with a PAPm 42 mmHg, RAP 8 mmHg, PCW 10 mmHg, Q 6.0 L/min, QI 2.7 L/min/m2 and PVR 5.3 Wood units. The patient was seen back, and re-tested, approximately 4 months later.
These cases are part of an on going study investigating gas exchange in PAH patients that has been reviewed and approved by the Mayo Institutional Review Board. Patient consent was obtained prior to testing.
Results
Traditional clinical tests
Echocardiographic measurements and 6-minute walk distance are shown in Table 1.
Routine clinical measures used to assess pulmonary hypertension severity.

Submaximal Exercise Gas Exchange

Patient A: Gas exchange variables at rest and during exercise at baseline (circle) and 3-months following treatment (square). Data is presented for PETCO2 (

Patient B: Gas exchange variables at rest and during exercise at baseline (circle) and 5-months following treatment (square). Data is presented for PETCO2 (
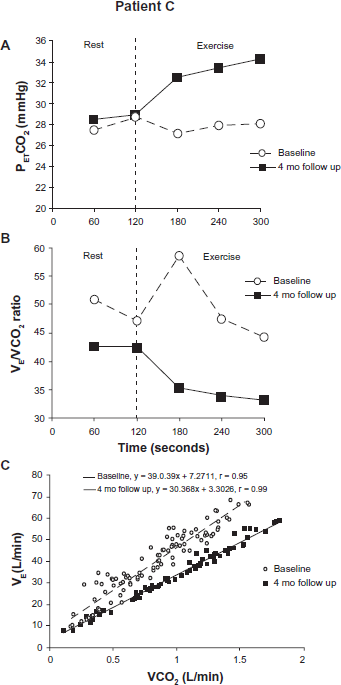
Patient C: Gas exchange variables at rest and during exercise at baseline (circle) and 4-months following treatment (square). Data is presented for PETCO2 (
Discussion
Multiple parameters are currently utilized in an effort to track progress of patients with pulmonary arterial hypertension, and each of them has their strengths and weaknesses. Following a major shift in therapeutic approach such as occurred in patient A, we saw substantial improvement in multiple parameters including gas exchange variables. Patient B, with no fundamental change in treatment plan, had multiple parameters that were persistently abnormal but without consistent or major changes in direction. Worsening of submaximal gas exchange variables, PETCO2 and VE/VCO2, was of concern but the significance of such changes needs to be further elucidated by serial follow up. Patient C was in a category of quite well preserved 6 minute walk distance and RV function where sensitivity of such methods for improvement in condition is limited. In fact he had little change in his right heart function/pressure by echo estimates aside from the increase in TAPSE, and a decrease in 6 minute walk distance. Gas exchange variables suggested there was an improved function following 4 months of therapy and appeared consistent with his impression of clinical improvement. It is possible that gas exchange variables, such as VE/VCO2, are more sensitive measures than other clinical measures and are able to better detect smaller changes earlier following treatment. Gas exchange data during submaximal exercise could, therefore, be a useful tool to track disease severity in PAH patients. Reduced pulmonary perfusion and V/Q (ventilatory/ perfusion) mismatch is thought to be the most likely cause of alterations in breathing efficiency and end-tidal CO2 levels in PAH.
Traditional clinical measures used to determine PAH severity and track patient responses to treatment are expensive, time consuming and require technical expertise (echocardiography) or lack sensitivity and ignore important aspects of disease (6 minute walk test). 1 There is currently a need for more sophisticated endpoints that can be simply and inexpensively obtained. Recently it has been suggested that measuring gas exchange during exercise may be the answer, considering that one of the main symptoms of PAH is dyspnea. Submaximal CPET may be a more meaningful and specific endpoint measure that allows for the measurement of key variables (ie, physiological dead space, breathing efficiency and end-tidal CO2) that are likely to be affected by PAH. Recent research has described characteristic gas exchange abnormalities in PAH patients, including a high VE/VCO2 slope/ratio, 3 a low resting PETCO2 and decreased PETCO2 during exercise. 4 It has been suggested that these gas exchange variables track physiological changes in response to therapy. 5 There is potential for developing algorithms, using multiple gas exchange variables (ie, VE/VCO2, PETCO2 and other parameters), that may allow a more sophisticated and sensitive, yet simple, way to track disease status. More work is clearly required in this area to determine which parameters should be used and also to standardize testing so that there is uniformity in clinical practice.
Conclusion
These cases demonstrate the potential utility of measuring submaximal exercise gas exchange to track responses to therapies in PAH patients. This will need to be evaluated and validated in a study of multiple PAH patients before its potential role in a clinical setting and as an endpoint measure can be fully understood.
Abbreviations
cardiopulmonary exercise testings;
pulmonary arterial hypertension;
mean pulmonary artery pressure;
pulmonary wedge pressure;
end tidal CO2;
pulmonary vascular resistance;
cardiac output;
cardiac index;
right atrial pressure;
right ventricle systolic pressure;
tricuspid annular plane systolic excursion by M-mode echocardiography;
ratio of minute ventilation to expired carbon dioxide (a measure of breathing efficiency);
ventilation/ perfusion.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material. Written consent was obtained from the patients for publication of this study.