
Abstract
Background:
Anemia is reported in one-third of the patients with chronic obstructive pulmonary disease (COPD). Anemia, by decreasing oxygen content, can be a contributing factor for hypoxemia. We determined to find whether anemia causes more prominent hypoxia by decreasing the total oxygen content after exercise in anemic patients with COPD.
Methods:
Stable moderate-to-severe COPD patients with and without anemia were recruited. Arterial blood gas analyses were performed on room air before and after a 6-minute walking test (6MWT). Walking distance, oxygen saturation, and heart rate were recorded in each case before and after the 6MWT. Pulmonary function test measurements and other data were obtained from the chart. The mean and standard deviations were calculated for continuous variables. The independent t-test and Kruskal-Wallis test were performed for numerical covariate and univariate analyses. The paired t-test was used for the analyses of data before and after exercise.
Results:
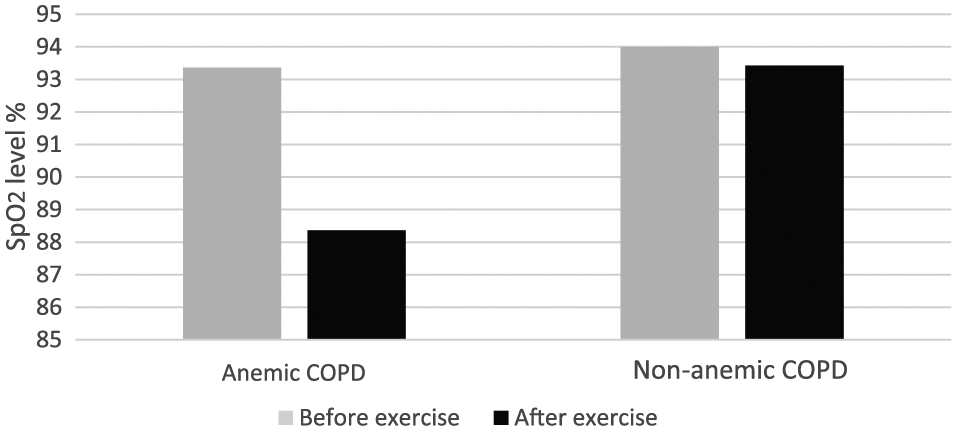
A total of 24 male patients were included in the study; 12 of which were anemic. The oxygen content was decreased in the anemic group (15.22 ± 1.28 vs 15.07 ± 1.22) after exercise, but it was not significant. In the non-anemic group, no oxygen content decrease was observed after exercise (18.83 ± 1.41 vs 18.9 ± 1.37). Interestingly, the Sp
Conclusions:
Anemia does not cause more prominent hypoxemia after exercise in patients with COPD. However, the recorded Sp
Introduction
Previous studies have reported that 13%–33% of patients with chronic obstructive pulmonary disease (COPD) may have anemia.1–3 The mechanism of anemia is not clear, but it is likely related to the systemic effects of COPD. 4 Hypoxemia refers to insufficient oxygenation in blood. It can be caused by hypoventilation, a ventilation-perfusion mismatch, right-to-left shunt effects, diffusion impairment, or reduced inspired oxygen tension. Hypoxemia is most commonly due to a ventilation/perfusion (V/Q) mismatch in COPD. 5 Anemia, itself, does not cause hypoxemia. However, anemia decreases the total oxygen content in the blood. This effect can be compensated by increasing the cardiac output and oxygen extraction ratio. Therefore, until very low levels of hemoglobin are observed, hypoxemia is not a concern in anemic patients. 6
In patients with COPD, besides a V/Q mismatch, the low oxygen content due to anemia may play a role in deterioration, and oxygenation and compensatory mechanisms may not be sufficient to overcome the effects. As a result, anemic patients with COPD may have more indications for long-term oxygen therapy (LTOT) than those without anemia. The significance of low hemoglobin (Hgb) levels in terms of LTOT indications has not been determined for patients with COPD.
Our clinical observations suggested that anemic patients with COPD were prescribed more LTOT than non-anemic patients with COPD. In a retrospective study, we found that anemic patients with COPD were more likely to be qualified for LTOT and had much lower mean oxygen saturation after exercise. 7 Because our previous study was limited being retrospective and not including arterial blood gases (ABG), we were unable to assess arterial oxygen content.
In this study, we determined to find if anemia causes more prominent hypoxia by decreasing total oxygen content after exercise in anemic patients with COPD compared to that of non-anemic patients with COPD.
Methods
This was a prospective clinical study conducted at the Captain James Lovell Federal Health Care Center (FHCC) and was approved by the Institutional Review Board. Patients with COPD who were scheduled in the outpatient pulmonary/oxygen clinic were screened using electronic charts. Inclusion criteria were moderate and severe COPD patients with and without anemia. Exclusion criteria were mild COPD patients, any patient who had a fistula or graft on a radial artery, having bleeding diathesis, were on anticoagulant therapy, patients who were unable to walk, and any patient with a co-morbid condition such as congestive heart failure, pulmonary hypertension, malignancy, pleural disease, history of venous thromboembolism, chronic renal failure, any blood disease, any other important organ failure, or systemic disorder. Any patient who has recent acute exacerbation of COPD was also excluded from the study. We did not exclude any patient with common co-morbidities such as hypertension, diabetes, hyperlipidemia, post-traumatic stress disorder, prostate hypertrophy, and osteoarthritis.
Informed consent was obtained in the clinic from the eligible patients who agreed to participate in the study. The patients were taken inside an exam room and allowed to rest for 10 minutes in a chair. An ABG measurement in room air was taken from the radial artery. After the ABG measurement was complete, pulse oximetry was obtained by attaching the device to the patient’s finger. Oxygen saturation and heart rate were recorded in room air while at rest. A research assistant walked with the patient in the corridor for 6 minutes in room air, and the heart rate and walking distance were recorded. After returning to the exam room, the patient’s ABG level was immediately measured from the other radial artery, while in room air. Finally, blood samples were taken for subsequent measurements within 10 minutes of collection.
The patients’ age, first forced expiratory volume (FEV1), forced vital capacity (FVC), FEV1/FVC, Hgb, hematocrit, body mass index (BMI), smoking history, and prior and current medications were recorded. The cause of anemia was recorded for each anemic patient. If Hgb data were older than 3 months, or if there was a suspicion for an aberrant Hgb measurement, a new Hgb level measurement was requested. Because our previous study showed a mean Hgb level of 11.7 ± 0.92 g/dL in the anemic group and 14.8 ± 0.99 g/dL in the non-anemic group, we included patients with COPD having these hemoglobin levels for each group (10.8–12.6 g/dL for anemic and 13.7–15.7 g/dL for non-anemic patients). Two-year intervals were accepted for the pulmonary function test (PFT) data.
Techniques
Arterial blood gases
A pro-vent arterial blood sampling kit with dry lithium heparin was used for arterial blood ABG measurements. Before the procedure, an Allen test was performed to ensure that both the ulnar and radial arteries were patent. Approximately 3 cm3 of arterial blood was drawn each time. A filter was placed on the tip of the syringe, and air bubbles inside the syringe were removed. After the 6-minute walking test (6MWT), the same procedure was repeated on the other radial artery. Blood samples were sent immediately to the laboratory after the second arterial blood sample was drawn. The ABG analysis was initiated using an ABL 835 Flex blood gas analyzer radiometer within 10 minutes of collection for all blood samples. After the second ABG sample was taken, the patient was asked to remain for 30–60 minutes in the waiting area. The hands and radial pulse were re-evaluated every 5–10 minutes before the patient was allowed to leave.
6-Minute walking test
The patients walked in a 52-foot-long (15.8 m) corridor during the test. A pulse oximeter (Masimo, Irvine, CA, USA) was placed on the index finger during the test, and a research assistant walked with the patient. The total distance walked was recorded at the end of 6 minutes. The Sp
Oxygen content was calculated using the Pa
Statistics
The mean and standard deviation were calculated for continuous variables. The independent t-test and Kruskal-Wallis test were used for numerical covariate and univariate analyses. The paired t-test was used for the analyses of data before and after exercise in both groups. P < .05 was accepted as significance level.
Results
A total of 26 patients with COPD were enrolled in the study. Two of the patients were excluded due to technical reasons, so 24 patients were included in the study. All patients were male, and 50% were anemic. The patients’ characteristics are listed in Table 1. Both groups were matched in terms of age, PFT findings, and severity of COPD. The mean age was not different between the groups, but the anemic group was slightly older. The Hgb levels and hematocrit values were significantly lower in the anemic group. There were 5 patients in non-anemic group and 4 patients in anemic group who had acute exacerbation of COPD within 1-year time period. But during the recruitment date, all patients were stable and free of sign and symptoms of exacerbations.
Patient characteristics.

Abbreviations: DLCO, diffusion capacity; FEV1, first forced expiratory volume; FVC, forced vital capacity; Hgb, hemoglobin; Htc, hematocrit; TLC, total lung capacity.
The PFT values (FEV1, FVC, FEV1/FVC, and total lung capacity [TLC]) and the severity of COPD were not different between the groups. The mean carbon monoxide diffusion capacity (DLCO) was lower in the anemic group compared with the non-anemic group, but did not reach significance. The mean walking distance was lower for the anemic group, but was not significant.
For data analyses, we compared the anemic vs non-anemic groups before and after exercise. The ABG values, heart rates, Sp
Comparison of anemic and non-anemic patients with COPD before exercise.

Abbreviation: COPD, chronic obstructive pulmonary disease.
Comparison of anemic and non-anemic patients with COPD after exercise.

Abbreviation: COPD, chronic obstructive pulmonary disease.
Comparison of anemic patients with COPD before and after exercise.

Abbreviation: COPD, chronic obstructive pulmonary disease.
Comparisons of non-anemic patients with COPD before and after exercise.

Abbreviation: COPD, chronic obstructive pulmonary disease.

Oxygen content before and after exercise in anemic and non-anemic patients with COPD.
Sp
Discussion
We hypothesized that total oxygen content in the arterial blood of anemic patients with COPD would be significantly lower after exercise. During exercise, compared to rest, oxygen release to the tissues would be higher in anemic patients as a compensatory mechanism. Patients with COPD already have a tendency for hypoxemia, mostly due to a V/Q mismatch. As a result, the mean mixed venous blood oxygen saturation would be lower. Also, the increased oxygen demand during exercise would increase cardiac output due to a rising heart rate. Therefore, the circulation time would be shorter for the red blood cells in the pulmonary vasculature for oxygenation.6,8,9 If the blood returning to the lungs (mixed venous blood) has a lower P
We have found 2 important but unexpected findings in this study. First, total oxygen content was not different before and after exercise in anemic patients with COPD contrary to our hypothesis (Table 4 and Figure 1). Second, we found significant decrease in Sp
The reason for the second finding is not clear. However, we suggest that while Sa
We also observed increases, but not decreases, of Sp
Guo et al performed a study on patients with COPD to evaluate the impact of anemia on PFT at rest and ventilator efficiency and exercise capacity using CPETs. They found no differences in the PFT at rest except for a lower DLCO in the anemic group. In our study, the PFT results were similar. The mean DLCO was lower in the anemic group, but no difference was found compared with that of non-anemic group. However, the mean hemoglobin level in the study of Guo et al was lower than those of our patients (11.79 g/dL vs 10.6 ± 0.8 g/dL). Additionally, our study had a smaller number of patients. They also reported a lower peak V
The 6MWD values were lower in the anemic group, but it was not significant compared with that of non-anemic group. Rutten et al 13 reported 6MWD and Body-mass index, airflow Obstruction, Dyspnea, and Exercise (BODE) scores that were the same as patients with and without anemia. These results support our findings.
Cote et al 3 found that in patients with stable COPD the presence of anemia affected feelings of dyspnea and decreased exercise tolerance in the 6MWD. We did not check for dyspnea in our patients. However, the exercise tolerance based on the 6MWD was lower in the anemic group, but did not reach a significance level.
Strengths and limitations
The study was a prospective study with a control group. However, there were some limitations in our study. First, the patient number was small in the groups and we did not randomize for practical reasons. We used the ABGs before and after exercise. It would have been better if we had measured the mixed venous oxygen levels. However, we did not use mixed venous oxygen due to its invasive nature, risk, and cost. The Sp
In conclusion, anemia does not cause more prominent hypoxemia after exercise in patients with COPD. However, the recorded Sp
Footnotes
Acknowledgements
This work was presented in the ACCP meeting October 2017, Toronto, Canada.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
Conception and design: ASC. Acquisition of data: ASC, HD, LW and KH. Analysis and interpretation: ASC and ZC. Drafting the article for important intellectual content: ASC, AF, NA, ZC. All authors contributed to the intellectual content of the manuscript and were consulted for final approval of the submitted version.