
Abstract
Background
Mucoepidermoid carcinoma of the parotid gland may occasionally present with cyst-like or deceptively benign radiologic features, even when the final histopathological architecture is predominantly solid. Diagnostic difficulty increases when the lesion appears separated from the parotid gland and mimics a superficial postauricular cyst.
Case presentation
We report the case of a 49-year-old patient presenting with a painful left postauricular swelling associated with ipsilateral House-Brackmann grade III peripheral facial paralysis. Ultrasound and MRI suggested a well-circumscribed benign cystic lesion, interpreted as a remodeled epidermoid cyst, located in the retroparotid/postauricular region. However, the clinical red flags prompted surgical management. Histopathological examination considered most compatible with a mucoepidermoid carcinoma involving the parotid/posterior parotid region, with dermal extension. The patient subsequently underwent total parotidectomy and cervical lymph node dissection, followed by adjuvant radiotherapy after multidisciplinary tumor board discussion.
Conclusion
This case highlights that any postauricular or parotid-region mass associated with facial nerve dysfunction should be considered malignant until proven otherwise, even when imaging suggests a benign cystic lesion. Radio-clinical discordance should prompt an oncologic diagnostic strategy and careful histopathological evaluation.
Keywords
Introduction
Cystic or cyst-like lesions of the parotid and peri-parotid region include both non-neoplastic and neoplastic entities. Benign differential diagnoses include Warthin tumor, lymphoepithelial cysts, first branchial cleft cysts, lymphatic malformations, epidermoid or dermoid cysts, and retention cysts. However, several malignant salivary gland tumors, including mucoepidermoid carcinoma, acinic cell carcinoma, salivary duct carcinoma, myoepithelial carcinoma, and metastatic intra- or periparotid lymph nodes, may also show cystic or deceptively benign imaging features.1-4 Cystic metastatic lymph nodes within or around the parotid gland should also be considered, particularly metastases from cutaneous squamous cell carcinoma of the head and neck region. 5 The parotid gland is the most commonly affected site, 6 with a female predominance and a mean age at diagnosis of around 49 years. Reported 5-year overall survival ranges from 67% to 90%, depending on histological grade.6,7 Although most patients present with a solitary, asymptomatic mass, mucoepidermoid carcinoma may have a substantial cystic component. 8
We report a case of mucoepidermoid carcinoma of the posterolateral extension of the parotid gland, which radiologically mimicked a benign postauricular epidermoid cyst, while the clinical presentation (pain and facial nerve paralysis) was discordant and suggestive of malignancy.
Case Presentation
A 49-year-old patient presented with a two-month history of a painful swelling in the left retroauricular region, associated with ipsilateral peripheral facial paralysis.
On physical examination, there was a left retroauricular mass in the parotid region, with violaceous discoloration of the overlying skin (Figure 1). The mass was mobile relative to the deep plane, with a soft consistency. Examination of the auricular region and the skin of the external auditory canal was normal. The cervical lymph node chains were free of palpable adenopathy. Clinical photograph showing a violaceous swelling in the left retroauricular region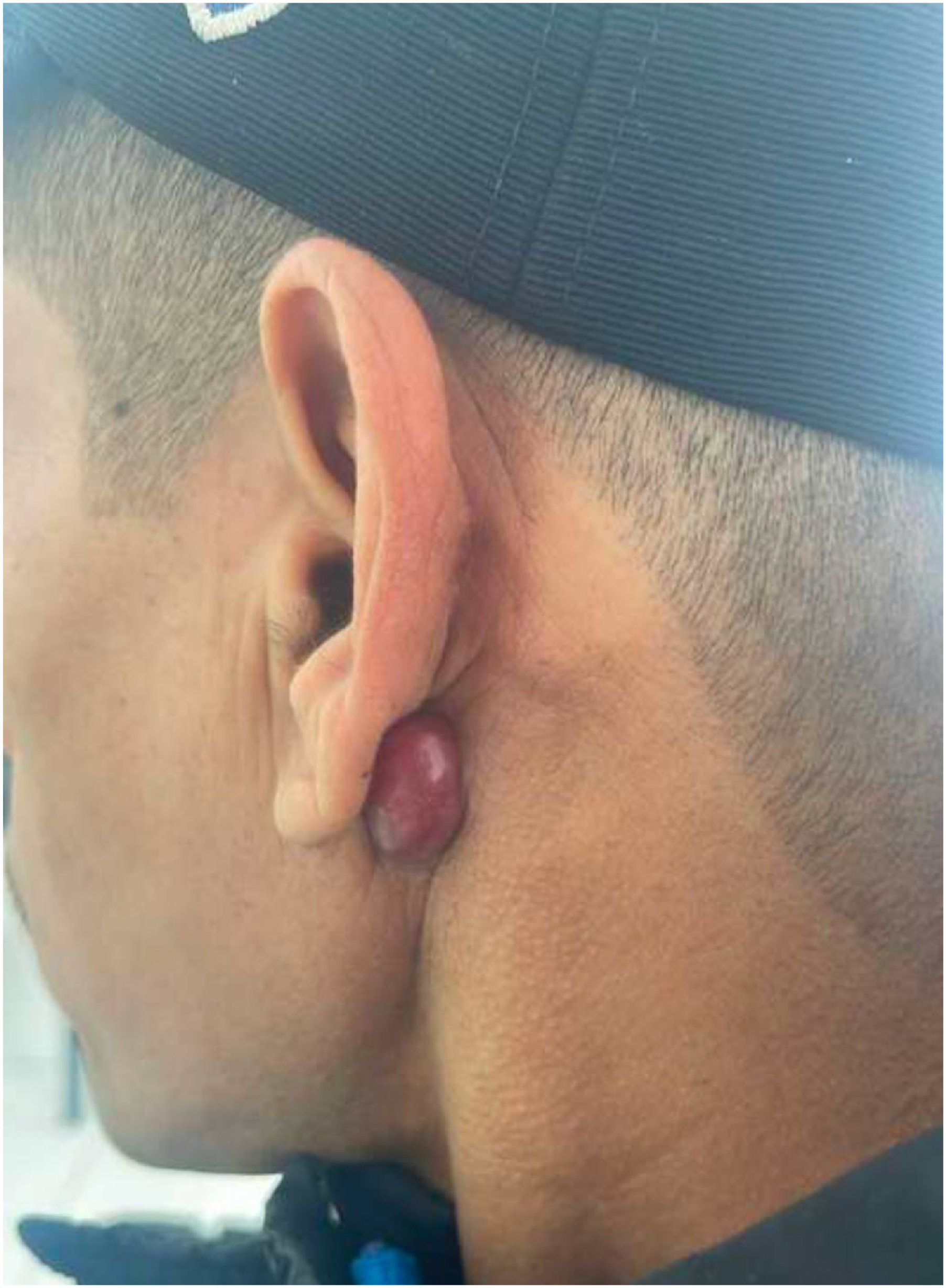
Cranial nerve examination revealed a left peripheral facial paralysis, grade 3 according to the House-Brackmann classification. The remainder of the ENT examination was unremarkable.
An initial facial ultrasound was performed and showed a left para- and retroauricular subcutaneous mass, iso-echogenic, discretely vascularized predominantly at the periphery, with regular contours, respecting adjacent soft tissues, and measuring 12 × 9 mm.
Facial MRI (Figure 2) demonstrated a well-circumscribed, oval lesion with sharp margins, hypointense on T1-weighted images, hyperintense on T2-weighted and diffusion sequences with a decreased apparent diffusion coefficient (ADC ≈ 1), and showing homogeneous, moderate enhancement after gadolinium injection. The lesion was located in the left retroparotid region, separated from a normal-appearing parotid gland by a thin fat plane. It measured 14 × 14 × 17 mm. No definite radiologic evidence of facial nerve involvement or perineural spread was identified. MRI was initially interpreted by a head and neck radiologist as suggestive of a remodeled epidermoid cyst. After histopathological diagnosis, the images were retrospectively reviewed in a multidisciplinary setting by the radiology and ENT teams. The lesion still showed well-circumscribed margins and a superficial postauricular location, explaining the initial benign interpretation; however, the facial nerve dysfunction remained clinically discordant with a benign cystic diagnosis. Axial facial MRI. Well-circumscribed oval lesion in the left retroparotid/postauricular region, indicated by white arrows. (A) T1-weighted image showing a hypointense lesion. (B) T2-weighted image showing a hyperintense lesion. The lesion appeared separated from the parotid gland by a thin fat plane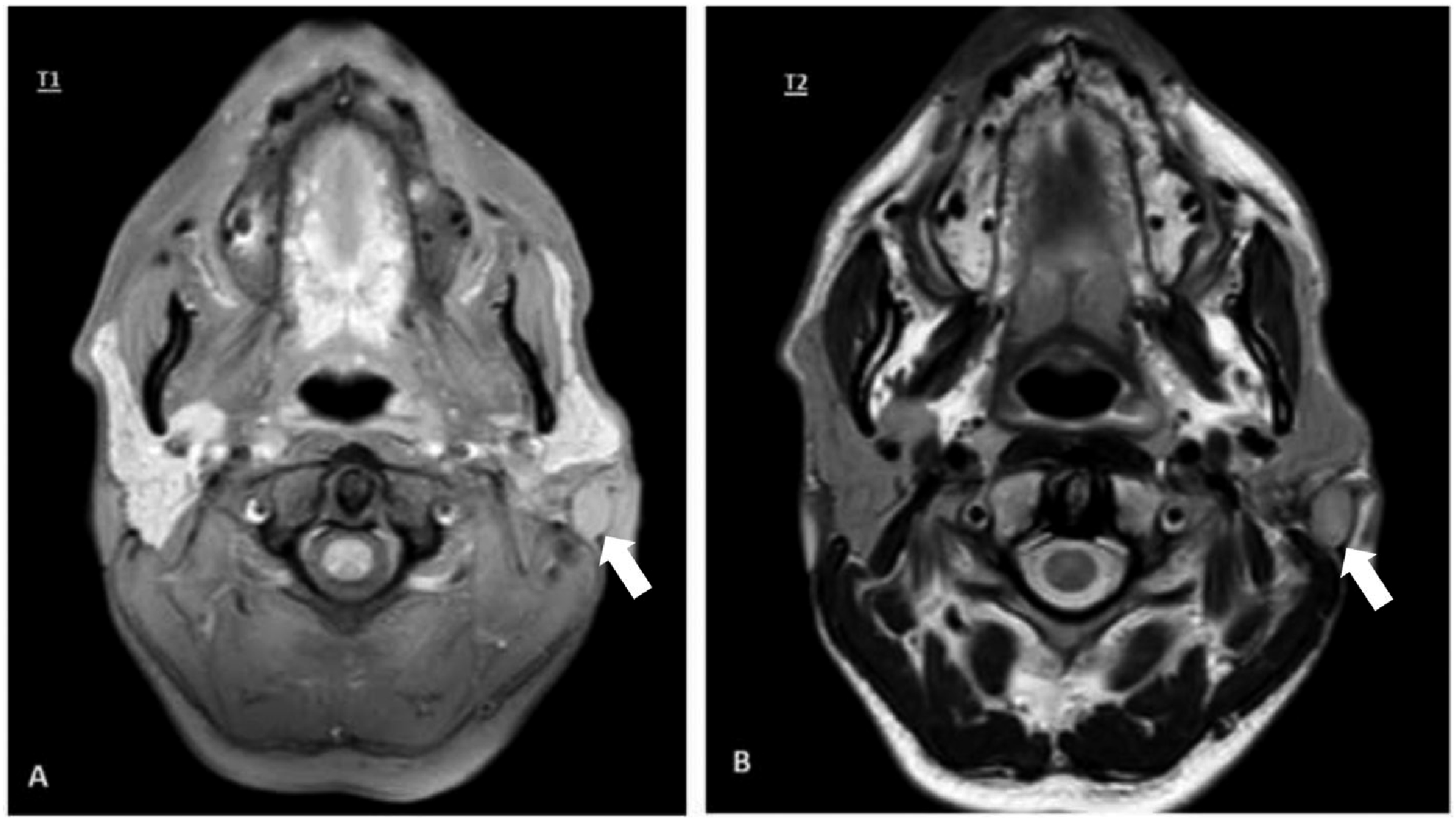
The patient underwent exploratory cervicotomy under general anesthesia. The initial surgical excision removed the mass en bloc together with its cutaneous covering. Histological examination of the initial cutaneous specimen showed a dermal localization of an infiltrative carcinomatous proliferation compatible with mucoepidermoid carcinoma, with an intact overlying epidermis. The tumor was composed of mucin-producing, epidermoid and intermediate cells, with moderate cytologic atypia and mitotic figures. No lymphovascular emboli or perineural invasion were identified.
A complete extension workup was negative. The patient then underwent a total parotidectomy combined with cervical lymph node dissection. Subsequent total parotidectomy confirmed a 1.5 × 1.3 cm mucoepidermoid carcinoma showing a predominantly solid and lobulated architecture with epidermoid, mucosecretory and intermediate/basaloid components. In view of the infiltrative dermal presentation and the associated facial nerve paralysis, the tumor was considered clinically aggressive and managed accordingly in a multidisciplinary oncologic setting. Surgical margins were not specified in the pathology report. Peritumoral lymph nodes and cervical lymph node dissection were negative for metastasis, with 0/7 peritumoral nodes, 0/14 level IIa nodes, 0/13 level III nodes and 0/4 level IV nodes involved. No extranodal extension was identified. The nodal stage was therefore pN0. Molecular testing for MAML2 rearrangement was not performed. The diagnosis was based on conventional histomorphological criteria.
The immediate postoperative course was uneventful. Facial nerve function remained House-Brackmann grade III postoperatively, which improved to House-Brackmann grade II at 3 months. The surgical wound healed without salivary fistula or infection. The case was discussed in a multidisciplinary tumor board, and adjuvant radiotherapy was indicated and performed because of the malignant histology, dermal involvement, and clinically aggressive presentation. At the last follow-up, 6 months after surgery, the patient showed no clinical or radiological evidence of recurrence.
Discussion
This observation illustrates the diagnostic difficulties that may arise in the evaluation of parotid tumors, particularly when there is discordance between clinical, radiological and histopathological findings. Certain MRI features can suggest benignity or malignancy, but overlap exists between benign and malignant lesions, and sometimes clear discrepancies appear between imaging and final histopathology. 9
The malignant nature of salivary gland tumors can be suspected based on a combination of clinical and paraclinical criteria. Clinically, pain, facial paralysis and lymph node involvement should alert the clinician. In our patient, there was a grade 3 peripheral facial paralysis concomitant with the onset of the tumor, and the mass was painful, two arguments in favor of malignancy despite a radiological appearance suggestive of a benign cyst.
Epidermoid cysts and mucoepidermoid carcinoma may overlap radiologically when both appear as well-circumscribed cystic or cyst-like lesions. Clinically, epidermoid cysts are usually slow-growing, superficial, mobile, and painless unless inflamed or ruptured. They do not cause facial nerve paralysis. Radiologically, epidermoid cysts are typically well-demarcated lesions with high signal on T2-weighted images and diffusion restriction related to keratinaceous content. In contrast, MEC may present as a cystic or mixed solid-cystic parotid lesion; low-grade tumors may appear deceptively benign, whereas high-grade tumors more often show infiltrative margins, solid components, necrosis, perineural spread, nodal disease, or skin invasion.
Although no perineural invasion was identified in the available pathology report, this finding should be interpreted with caution. Clinical facial nerve dysfunction may occur through several mechanisms, including close tumor contact, inflammatory involvement, compression, microscopic neural involvement not captured in the sampled sections, or involvement of small peripheral branches. Therefore, the absence of reported perineural invasion does not fully negate the clinical significance of the facial nerve paralysis.
Histologically, epidermoid cysts are lined by stratified squamous epithelium and contain laminated keratin, without infiltrative growth or cytologic malignancy. MEC is defined by a variable admixture of mucous, epidermoid and intermediate cells, with grading based on architectural and cytological features such as cystic component, neural invasion, necrosis, mitotic activity and anaplasia.1,2,4
MRI remains the imaging modality of choice for the evaluation of parotid masses. Classically, carcinomas appear hypointense to intermediate on T1-weighted images. Non-enhanced T1-weighted images are best for describing MEC because the high-signal fat of normal parotid tissue offers natural contrast. Other series have shown that only high-grade carcinomas consistently follow this pattern, whereas low-grade carcinomas may appear hyperintense on T2-weighted images, thereby mimicking a benign tumor. 10 This underlines the interest of new dynamic sequences (diffusion and perfusion), 1 which improve tissue characterization, but even with these tools, clear distinction between benign and malignant lesions is not always possible.
In the present case, the term “cystic” refers primarily to the initial radiological impression and cyst-like appearance, rather than to the final histological architecture. The final parotidectomy specimen showed a predominantly solid and lobulated mucoepidermoid carcinoma. This discrepancy between imaging appearance and histological architecture is precisely the diagnostic pitfall highlighted by this case.
Our case also illustrates the problem of radio-clinical discordance: MRI strongly suggested a remodeled epidermoid cyst, but the clinical picture (pain and peripheral facial paralysis) was more suggestive of a malignant parotid lesion. 11 In such situations, the clinician must prioritize clinical red-flag signs and adopt an oncologic approach, even if imaging appears reassuring. This case report has several limitations. First, the absence of histological images limits the reader’s ability to independently assess the pathological features of the lesion. Second, additional immunohistochemical or molecular testing, including MAML2 rearrangement analysis, could not be performed because of local logistical and resource constraints. Finally, because no dedicated expert pathological re-review was available, the pathological interpretation is based on the original institutional histopathological report and multidisciplinary clinicoradiological correlation. Despite these limitations, the case remains clinically relevant because it illustrates an important radio-clinical discordance: a superficially located, well-circumscribed lesion initially interpreted as benign despite the presence of pain and facial nerve dysfunction.
Conclusion
Preoperative evaluation of parotid-region masses requires careful integration of clinical examination and radiological findings. MRI remains a key imaging modality for characterizing parotid tumors, assessing their relationship to surrounding structures, and identifying features suggestive of malignancy. However, imaging may occasionally be misleading, particularly in cystic or well-circumscribed lesions that mimic benign entities.
In the presence of facial nerve paralysis, pain, skin involvement, or other clinical warning signs, malignancy should remain the primary diagnostic concern, even when radiological features appear reassuring. The differential diagnosis should extend beyond mucoepidermoid carcinoma to include other primary salivary gland malignancies and metastatic disease involving the parotid region. This case highlights the importance of recognizing radio-clinical discordance and adopting an oncologic diagnostic and therapeutic approach, with definitive histopathological assessment guiding final diagnosis and management.
Footnotes
Acknowledgement
No specific acknowledgments are applicable for this work.
Ethical Considerations
Ethical approval was not required for this single case report according to institutional practice.
Consent to Participate
Written and informed consent taken.
Consent for Publication
Written informed consent for publication of the clinical details and images was obtained from the patient.
Author Contributions
• Loubna Taali took part in taking care of the patient, researching the bibliography and writing the manuscript.
• Abderrahim Bourial took part in researching the bibliography and writing the manuscript.
• Zineb Dahbi, Said Anajar, Amal Hajjij approved the final manuscript
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
On request, email the corresponding author.