
Abstract
Introduction:
Achilles tendon xanthomas are uncommon lipid-rich lesions associated with familial hypercholesterolemia, typically affecting adult patients. Presentation during childhood or adolescence is uncommon, particularly among female patients, and often indicates severe underlying dyslipidemia. Early recognition is important to prevent long-term complications.
Case presentation:
A 17-year-old Indian girl presented with bilateral posterior ankle swelling and discomfort. Clinical examination revealed firm, non-tender, fusiform swellings adherent to both Achilles tendons. Laboratory evaluation revealed elevated low-density lipoprotein cholesterol and apolipoprotein B levels, consistent with heterozygous familial hypercholesterolemia. Magnetic resonance imaging (MRI) of both ankles demonstrated diffuse tendon thickening with a hypointense signal on T2-weighted sequences and speckled heterogeneity on proton density fat-suppressed images, confirming xanthomatosis. Surgical excision was performed on the right side, and histopathological examination confirmed the presence of foam cells and cholesterol clefts. The left-sided swelling was managed conservatively, with serial follow-up demonstrating stable morphology and no progression.
Discussion:
Radiological assessment using MRI allowed a clear distinction between xanthomas and other tendinopathies. Given the patient’s functional limitations, surgery provided mechanical relief, whereas lipid-lowering therapy addressed the underlying systemic risk.
Conclusion:
Recognition of tendon xanthomas in adolescents supports timely identification of hereditary dyslipidemia and initiation of coordinated orthopedic and metabolic care, with potential long-term cardiovascular benefit.
Keywords
Introduction
Achilles tendon xanthomas represent a diagnostic manifestation of systemic lipid disorders, commonly observed in familial hypercholesterolemia. 1 These lesions consist of lipid-laden macrophages, extracellular cholesterol clefts, and multinucleated giant cells deposited within tendinous tissue and typically appear in the context of persistent hyperlipidemia, particularly in individuals with low-density lipoprotein receptor (LDLR) mutations. 2 In the Fredrickson classification, these are commonly often associated with Type IIa familial hypercholesterolemia, although other lipid phenotypes can occasionally be implicated. 3 Clinically, tendon xanthomas may present as firm, non-tender, slowly enlarging swellings over tendon sites, with the Achilles tendon being one of the commonly affected regions, along with the extensor tendons of the hands and knees. 4
While Achilles tendon xanthomas are commonly described in adult males, presentation in adolescents, especially females, is unusual and may reflect early expression of significant dyslipidemia.5,6 Radiological identification of tendon xanthomas has become more refined with the use of magnetic resonance imaging (MRI), which offers high soft tissue contrast and can identify subtle intratendinous structural changes long before clinical deterioration. 7 These imaging findings not only assist in distinguishing xanthomas from tendinopathies and partial tears but also provide important clues to the underlying metabolic pathology, even in asymptomatic individuals.
Following the CARE guidelines (for CAse REports), 8 this case documents bilateral Achilles tendon xanthomas in a 17-year-old Indian girl confirmed by radiological and histopathological examinations. The patient’s clinical presentation, biochemical work-up, radiological findings, and successful surgical management are discussed in detail, with an emphasis on early diagnostic recognition and integrated care.
Case Presentation
A 17-year-old girl of Indian ethnicity presented to the orthopedic outpatient clinic with a 2-year history of gradually progressive swelling over the posterior aspects of both ankles. She experienced tightness and intermittent aching in both heels, particularly during prolonged standing, brisk walking, or athletic activities. The patient denied experiencing trauma, systemic joint symptoms, or constitutional complaints. Her academic and developmental milestones were appropriate for her age, and she had no history of endocrine, autoimmune, or chronic inflammatory conditions. The patient was otherwise active and healthy, with no known chronic illness or previous medication.
Family history was notable for cardiovascular events and hypercholesterolemia. Her father had experienced a myocardial infarction at the age of 42 years and was on lipid-lowering therapy. Her paternal aunt had been diagnosed with familial hypercholesterolemia in her late twenties and had visible tendon nodules on her hands and elbows. These features raised a preliminary suspicion of a hereditary dyslipidemic syndrome with cutaneous and tendinous manifestations.
On clinical examination, she was normotensive, with a body mass index of 21.6 kg per square meter. Local examination revealed well-defined, fusiform, firm, and non-tender swellings over the posterior aspects of both ankles, fixed to the underlying Achilles tendon. The overlying skin was normal. The swellings were approximately 4 cm in longitudinal length, and passive dorsiflexion of the foot was slightly restricted due to mechanical tension. Plantarflexion was preserved, and the rest of the musculoskeletal and neurological examinations were unremarkable. A systematic examination of other common xanthoma sites, including extensor tendons of the hands, elbows, knees, and feet, revealed no additional lesions. The peripheral pulses were intact, and there was no evidence of arcus juvenilis or xanthelasma.
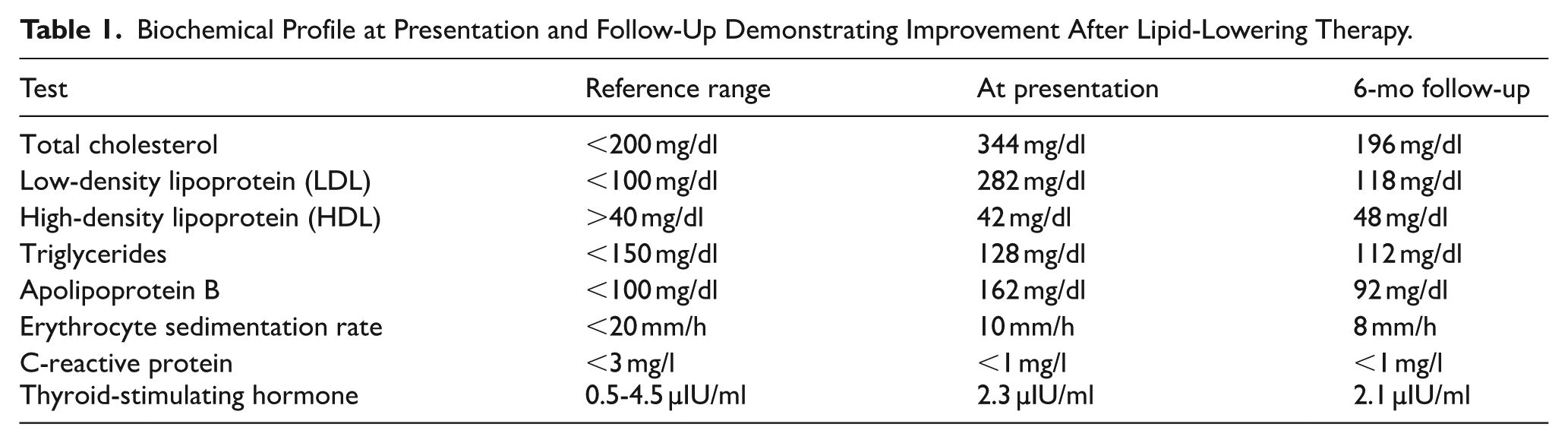
A focused laboratory workup revealed elevated total cholesterol and low-density lipoprotein cholesterol levels, along with an elevated apolipoprotein B concentration. Triglycerides and high-density lipoprotein cholesterol levels were within the reference limits. Inflammatory markers, including the erythrocyte sedimentation rate and C-reactive protein levels, were normal. Thyroid-stimulating hormone levels were within the physiological range. The relevant biochemical parameters are listed in Table 1. These findings, along with a strong family history of hypercholesterolemia, supported the clinical diagnosis of heterozygous familial hypercholesterolemia.
Biochemical Profile at Presentation and Follow-Up Demonstrating Improvement After Lipid-Lowering Therapy.
Radiological assessment of both ankle joints was performed using MRI to characterize the nature of tendon swelling. The imaging findings were nearly symmetrical. On the T2-weighted sagittal sequence, there was thickening of the Achilles tendon, with an anteroposterior diameter measuring 1.88 cm, exceeding reported normative values for Achilles tendon thickness (Figure 1). 9 The tendon appeared hypointense with a relatively uniform signal suppression, suggesting fibrous and lipid-rich infiltrative changes. On proton density fat-suppressed sagittal sequence, an intermediate signal intensity was observed within the tendon body, consistent with intratendinous deposition (Figure 2). Further evaluation using a matched axial slice demonstrated a speckled appearance of the tendon substance, characterized by a heterogeneous signal distribution with alternating hyperintense and hypointense foci, suggestive of admixed lipids and fibrous tissue (Figure 3A and B). These imaging features were consistent with tendon xanthoma. The left Achilles tendon exhibited an identical imaging profile in terms of thickness, signal characteristics, and structural architecture.
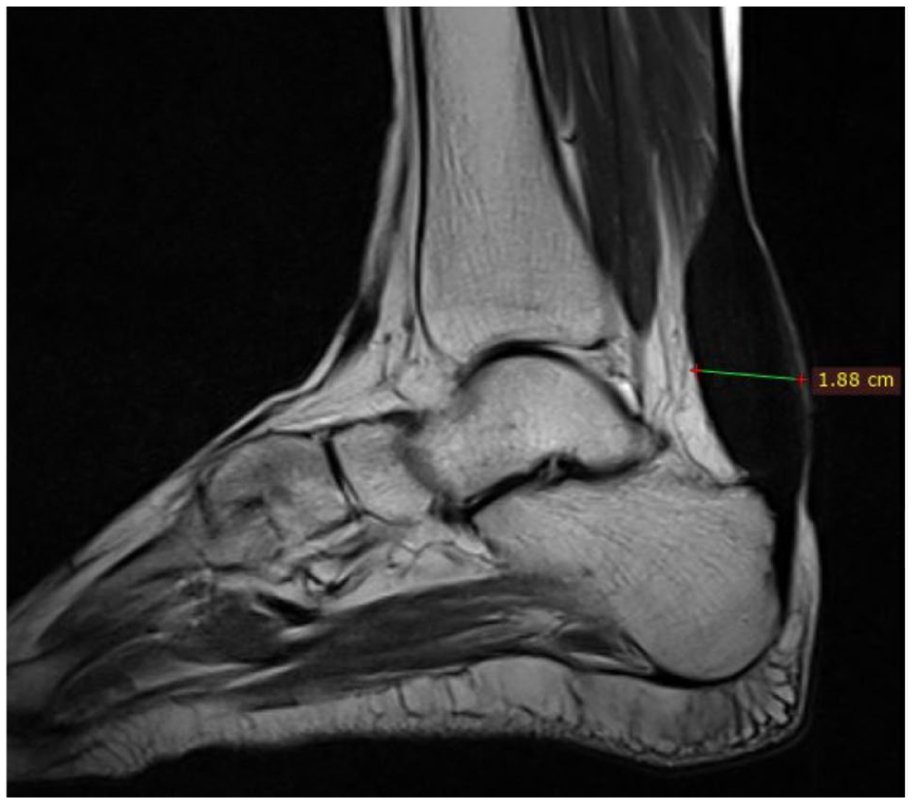
Sagittal T2-weighted image of the right ankle showing an anteroposterior diameter of 1.88 cm, which far exceeds normal dimensions and correlates with advanced xanthomatous infiltration.

Intermediate signal intensity (marked by yellow arrow) on a proton density fat-suppressed sequence, suggestive of lipid and fibrous tissue heterogeneity within the tendon body.
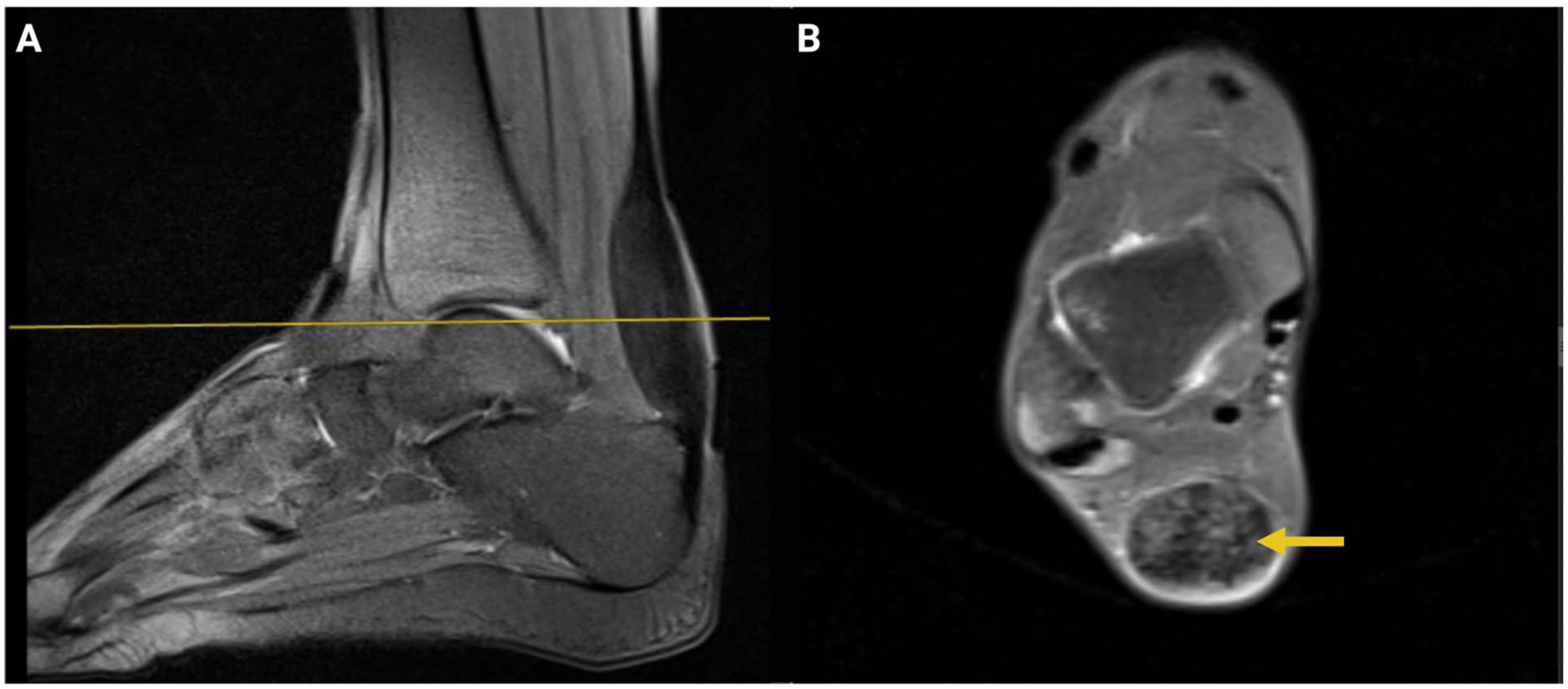
(A) sagittal imaging plane and the corresponding axial slice, (B) where a speckled appearance indicative of patchy lipid accumulation (marked by yellow arrow).
Given the progressive nature of the symptoms and the mechanical limitations imposed by the tendinous enlargement, we decided to proceed with surgical excision on the right side. Under spinal anesthesia, a posteromedial longitudinal approach was used. The Achilles tendon was exposed, and the xanthomatous tissue was identified as yellowish, lobulated, and rubbery masses within the tendon. The deposits were meticulously excised, and primary tendon continuity was restored using a side-to-side epitenon suture technique. The excised tissue was sent for histopathological examination, which confirmed the diagnosis of xanthoma, revealing foam cells, cholesterol clefts, and multinucleated giant cells dispersed in a fibrous stroma. The left Achilles tendon was managed conservatively because symptoms were minimal, and serial monitoring showed no structural progression.
Postoperatively, the patient was immobilized in a neutral ankle position using a short leg cast for 2 weeks. Physiotherapy was initiated thereafter, gradually progressing to full weight-bearing. Concurrently, the patient was referred to the pediatric endocrinology department for initiation of pharmacologic lipid-lowering therapy. She was commenced on high-intensity statin therapy with atorvastatin and received dietary counseling for long-term cholesterol control.
At 6-month follow-up, ankle mobility was normal, swelling had resolved on the surgical side, and the contralateral side remained stable with no clinical or ultrasonographic evidence of recurrence. Her low-density lipoprotein cholesterol level was reduced to 118 mg/dl. Longer-term monitoring is ongoing to assess for recurrence or contralateral progression.
Discussion
Tendon xanthomas, while rare, serve as visually and clinically accessible markers of systemic lipid abnormalities, particularly familial hypercholesterolemia. They tend to appear in locations exposed to high mechanical stress, where lipid-laden macrophages infiltrate the extracellular matrix of tendinous tissue. 10 The Achilles tendon is predisposed to rupture because of its size and load-bearing function. 11 Although adult cases are commonly described, occurrence during adolescence should heighten clinical suspicion for inherited dyslipidemia with early cardiovascular implications.
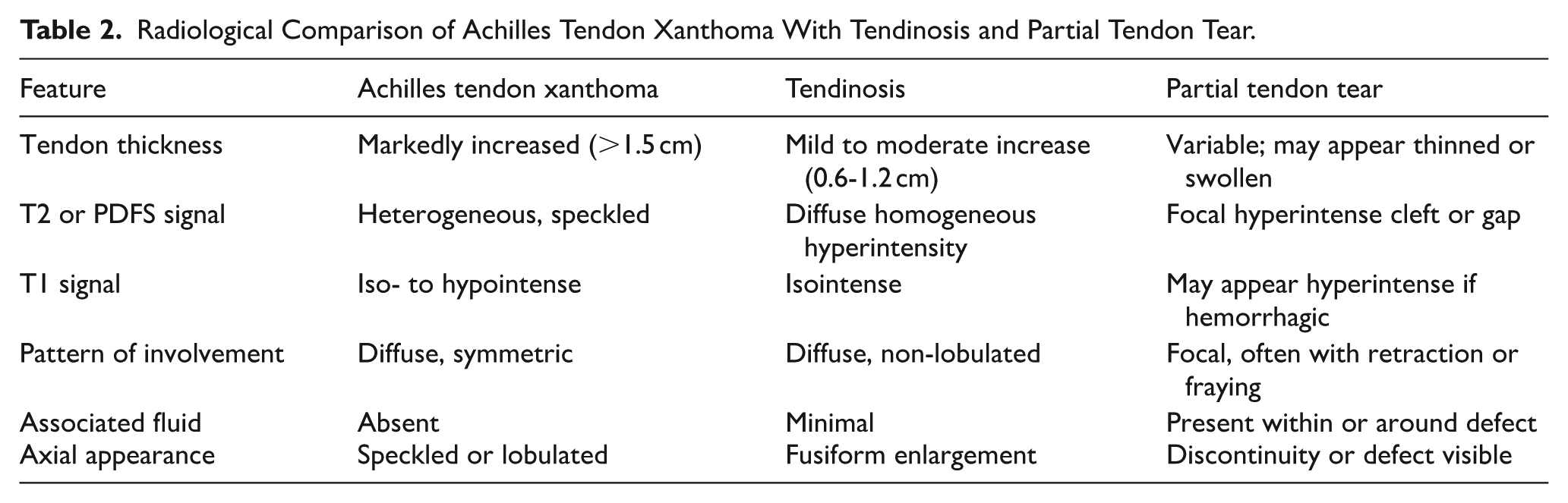
Radiological diagnosis using MRI remains the preferred modality for evaluating suspected tendon xanthomas. Characteristic features include fusiform tendon thickening, decreased signal intensity on T1- and T2-weighted sequences, and a heterogeneous speckled pattern on proton density fat-suppressed images. 12 Axial heterogeneity is particularly helpful in distinguishing xanthomatosis from other tendinopathies. For example, tendinosis typically presents as a homogeneous increase in signal intensity without speckling, 13 whereas partial tendon tears show focal fluid-filled clefts or defects. 14 The relevant radiologic distinctions are outlined in Table 2, which compares Achilles tendon xanthoma, tendinosis, and partial tears across multiple imaging parameters.
Radiological Comparison of Achilles Tendon Xanthoma With Tendinosis and Partial Tendon Tear.
Differential considerations include chronic tendinosis, partial tendon tears, chronic infections such as tuberculosis or fungal tendinopathy, metabolic conditions such as sitosterolemia, cerebrotendinous xanthomatosis, and rheumatoid nodules. Clinical and imaging features in this case excluded these possibilities. Risk factors for tendon xanthomas include LDL receptor mutations, prolonged untreated hypercholesterolemia, high mechanical tendon loading, and family history of premature cardiovascular disease.
Surgical management is generally reserved for symptomatic cases in which the mechanical function is compromised or cosmesis is a concern. Several techniques have been described in the literature, including subtotal excision with primary repair, excision with tendon grafting, and, in some cases, complete tendon reconstruction.15-18 Recently a novel technique for Achilles tendon reconstruction using an ipsilateral autologous semitendinosus tendon graft, which is a form of tendon grafting has been described by Oliva et al. 19 The choice of surgical technique depends on lesion extent, tendon integrity, and patient activity level, with subtotal excision and primary repair preferred in cases with preserved tendon architecture, while graft-based reconstruction is reserved for extensive involvement. In our patient, a side-to-side repair following en bloc excision was sufficient to restore function, reflecting early-stage structural integrity preservation. Surgery addresses local mechanical sequelae but not the underlying metabolic derangement. Therefore, initiation of lipid-lowering pharmacotherapy and regular follow-up with serum lipid profiles and cardiovascular risk assessment are critical for preventing systemic complications.
This report reflects the inherent constraints of a single-patient case, limiting generalizability and causal interpretation. Genetic confirmation of the underlying lipid disorder was not performed, restricting genotype–phenotype correlation. Histopathological validation was limited to the operated tendon, and the follow-up period was insufficient to evaluate long-term tendon remodeling, recurrence, or cardiovascular outcomes. Nevertheless, this case illustrates how a multidisciplinary approach encompassing orthopedic surgery, radiology, endocrinology, and pathology can lead to timely diagnosis and management of a condition that is locally relevant and systemically important. In adolescents with bilateral Achilles tendon swelling, especially with a family history of premature cardiovascular disease, the possibility of tendon xanthoma should be strongly considered.
Conclusion
Early identification of tendon xanthomas in adolescents enables timely diagnosis of hereditary dyslipidemia, initiation of targeted lipid-lowering therapy, and coordinated multidisciplinary care, with the potential to reduce long-term cardiovascular risk. Radiological pattern recognition and timely multidisciplinary care support favorable functional and systemic outcomes.
Footnotes
Acknowledgements
Dr. Amogh Verma serves as an Associate Editor for Clinical Medicine Insights: Case Reports. He had no involvement in the editorial handling, peer review, decision-making process, or publication outcome of this manuscript. All editorial decisions were made independently in accordance with the journal’s standard editorial policies. The authors declare that this role did not influence the conduct, interpretation, or reporting of the study.
Ethical Considerations
Ethical approval was not required for this study as per the policies of our institution. The Institutional Review Board waived the need for approval in accordance with the institutional guidelines for case-based studies.
Consent to Participate
Written informed consent was obtained from the legal guardian of the patient to participate in this study.
Consent for Publication
Written informed consent was obtained from the legal guardian of the patient for publication of this study (including images or case details).
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Generative AI Use Statement
Paperpal and ChatGPT-5 were used only for language and stylistic refinement. These tools had no involvement in study design, data analysis, interpretation, or content development. All intellectual contributions and scientific interpretations are the sole work of the authors, who take full responsibility for the accuracy, originality, and integrity of the manuscript.