
Abstract
Introduction:
Gallbladder volvulus (GV) is a rare surgical entity marked by torsion of the gallbladder on its axis secondary to mesenteric anomalies. Due to its clinical similarity to acute cholecystitis and preoperative diagnosis is difficult.
Clinical case:
A 79-year-old female with cardiovascular comorbidities presented with sudden abdominal pain and emesis. Initial laboratory examination tests showed leukocytosis and hyperbilirubinemia, while ultrasound suggested acute cholecystitis. Due to persistent symptoms and the development of a palpable mass, the patient underwent laparoscopic cholecystectomy. Intraoperatively, a gangrenous gallbladder secondary to complete volvulus was identified.
Results:
The gallbladder was detorsed and resected without complications. The postoperative course was uneventful, and the patient was discharge on the third day.
Conclusion:
GV should be suspected in elderly patients presenting with atypical biliary symptoms and a “floating gallbladder” on imaging. Early surgical intervention via laparoscopic cholecystectomy is essential to prevent life-threatening complications such as perforation and peritonitis.
Keywords
Introduction
Gallbladder volvulus is an atypical pathology when the gallbladder turns on its axis at the cystic pedicle (artery and duct), leading to vascular compromise. While its exact etiology remains obscure, it is frequently associated with mesenteric anomalies that grant the gallbladder abnormal mobility. Since its first description in 1989, approximately 500 cases have been reported worldwide. 1
The condition predominantly affects the elderly, with a female-to-male ratio of 3:1, most commonly occurring between the ages of 60 and 80. 2 Despite advances in imaging, preoperative diagnosis is achieved in less than 10% of cases, often being misdiagnosed as acute cholecystitis.3-7 Delayed surgical intervention is associated with mortality rates between 6% and 16% due to complications such as sepsis or peritonitis.7,8
Clinical Case
A 79-year-old female with a history of hypertension, left bundle branch block, and dyslipidemia presented to the emergency department. She described 6 days of diarrhea, sudden, intense, colicky abdominal pain around the epigastrium radiating to the hypochondria and back, combined with nausea, several emetic episodes, and oral intolerance. She reported a similar episode with a self-limited course 8 months prior. On admission, the patient was hemodynamically stable and afebrile, but exhibited tenderness in the epigastrium and right hypochondrium and had a positive Murphy’s sign.
Laboratory analyses revealed leukocytosis, indirect hyperbilirubinemia, and elevated liver enzymes. Arterial blood gases demonstrated compensated respiratory alkalosis. Hepatobiliary ultrasound showed a dilated extrahepatic bile duct (10 mm) without endoluminal lesions, non-specific thickening of the gallbladder wall (8 mm), and a negative sonographic Murphy’s sign. This case was initially managed as Tokyo II Acute Cholecystitis.
Magnetic Resonance cholangiopancreatography (MRCP) ruled out choledocholithiasis but indicated biliary unexplained biliaty dilatation. The clinical course worsened, with increasing pain and the appearance of a palpable mass in the right hypochondrium. Laboratory follow-up showed worsening leukocytosis with a left shift. Given the clinical deterioration, the patient was referred for urgent laparoscopic cholecystectomy.
Intraoperative Findings
The gallbladder exhibited ischemic walls with necrotic areas and adhesions to the omentum (Figure 1). A complete gallbladder volvulus was identified, rotating on a long, poorly inserted cystic pedicle without hepatic appearence (Figure 2). A long, poorly inserted, and ischemic cystic duct with a transition zone following the torsion was observed (Figure 3). After detorsion, the “Critical View of Safety” was reached, and the cystic artery and duct were lugated with Hem-o-lok clips.
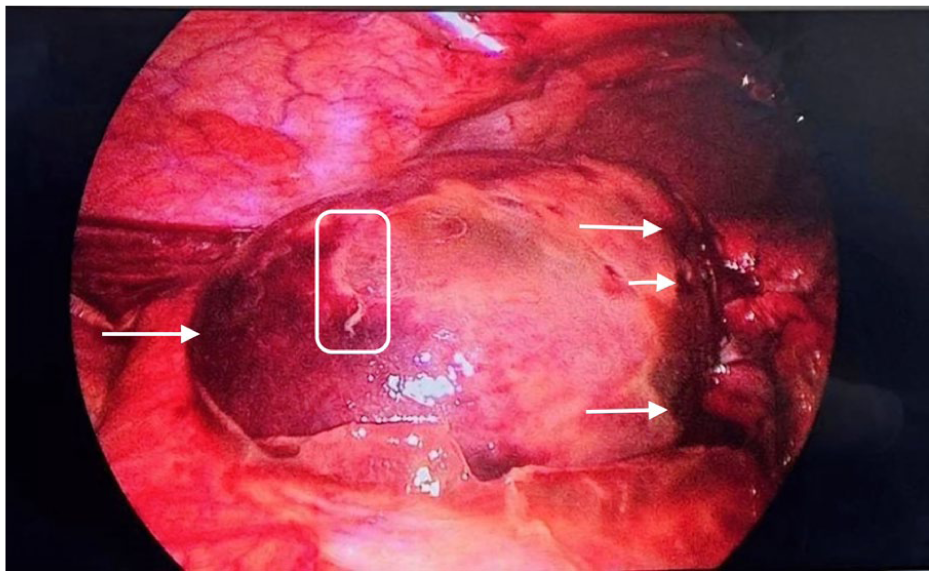
Gallbladder with thickened walls (rectangle) and necrotic regions (arrows).

Cephalad displacement of the gallbladder demonstrates that this organ is free from the hepatic bed of inflammation (black arrow) and has a single inflammatory attachment point on the liver edge (white arrow).

Cystic artery (black arrow) and cystic duct (white arrow) showing fibrotic changes at the torsion site with ischemic low-insertion cystic duct.
Evolution
The postoperative course was acceptable (oral tolerance satisfactory, pain settled and laboratory parameters normal). The patient was discharged on the third postoperative day.
The chronological sequence of the patient`s clinical course, form the onset of the symptoms to the surgical intervention and discharge, is summarized in Table 1.
Timeline of Clinical Presentation, Diagnostic Workup, and Surgical Intervention.

Discussion
GV can be classified into 2 types: complete torsion (greater than 180°), which usually presents as an acute surgical abdomen due to rapid vascular occlusion, and incomplete torsion (less than 180°), which may mimic recurrent biliary colic.3,9,10
The “floating gallbladder” phenomenon is the primary predisposing factor, often caused by anatomical changes during gallbladder embryogenesis, including prevalence of an elongated and incomplete mesentery, leaving the cystic pedicle susceptible to torsion; low or abnormal insertion of the cystic duct—which may play a rotational axis function—and hepatic atrophy, which results in decreased support and greater mobility.3,9,10 In this case, the presence of a palpable mass and the failure of conservative management for suspected cholecystitis were key indicators of a more complex underlying pathology.
Diagnostic Imaging and Differentials
Differential diagnosis includes acute acalculous cholecystitic, perforated peptic ulcer, and appendicitis. While ultrasound (US) is the first-line tool, abdominal computed tomography (ACT) and Magnetic Resonance Cholangiopancreatography (MRCP) provide superior anatomical detail. Typical MRCP findings, as seen in this case´s retrospective view, include the “whirl sign” of the cystic pedicle and an ectopic gallbladder position.1-4
Study Limitations
This study is primary limited by the inherent nature of a single-case report, which focuses on a specific clinical presentation and may not represent the full clinical spectrum of gallbladder volvulus in different populations. While our findings highlight the importance of early surgical intervention, the extreme rarity of this pathology prevents the formulation of generalized diagnostic protocols or statistical conclusions. In addition, the whirl sign was identified retrospectively, the lack of specific preoperative suspicion remains a significant challenge in the management of this condition worldwide.
Treatment and Conclusion
The definitive treatment is emergency surgery. The laparoscopic approach is now considered the gold standard, allowing for both diagnostic confirmation and therapeutic intervention.3-7 The surgical strategy must follow 3 principles: decompression, detorsion, and safe resection.3,7-10 In conclusion, although rare, GV must remain a differential diagnosis in elderly patients to ensure timely intervention and avoid the high mortality associated with gallbladder gangrene.
Footnotes
Acknowledgements
None.
Ethical Considerations and Consent to Participate
Ethical approval for this case report was waived by the Institutional Review Board of Hospital Universitario San Ignacio/Pontificia Universidad Javeriana, as it is a retrospective description of a single clinical case following standard of care and ensuring patient anonymity.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
All authors listed in this manuscript have contributed significantly to the work and meet the ICMJE criteria for authorship. Specifically, S.R.U., V.C.G., A.B., and J.A.G were involved in the conception and design of the study. S.R.U and V.C.G contributed to the acquisition of clinical and surgical data. S.R.U., V.C.G., A.B., and J.A.G contributed to the analysis and interpretation of the results. The manuscript was drafted by S.R.U and V.C.G and was critically revised for important intellectual content by all co-authors. Finally, all authors have given their final approval of the version to be submitted and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The clinical data and surgical images used during the current study are available from the corresponding author on reasonable request.