
Abstract
Introduction:
Descending necrotizing mediastinitis (DNM) is an acute infection of the mediastinum secondary to odontogenic, pharyngeal, or cervical infections that extend into the deep cervical spaces and progress into the mediastinum. This case report and literature review aim to contribute to the understanding of DNM and emphasize the importance of the surgical approach in its treatment.
Presentation of the case:
A 28 year old male with no relevant history, consulted a fourth level institution after presenting upper respiratory symptoms. CT scans revealed compatible findings with type II DNM plus bilateral pleural empyema. Pleural and mediastinal drainage, pleurectomy, and pulmonary decortication were performed using bilateral thoracoscopy. Cervical drainage via cervicotomy was subsequently required. Antibiotic treatment was continued for 6 weeks. For the literature review, a search was conducted in PubMed, Elsevier, and Scielo, yielding 35 articles published between 1938 and 2024, of which 22 were selected by the authors.
Discussion:
Treatment of DNM requires broad-spectrum antibiotics and timely surgical drainage. The approach must depend on the anatomical extent of the disease. Endo’s classification, revised by Sugio, allows appropriate staging and surgical guidance. Mediastinal drainage can be performed via thoracotomy or video-assisted thoracoscopy, and it often needs to be complemented with cervicotomy for adequate infection control.
Conclusion:
This case exemplifies the pivotal role of anatomical classifications as a tool to guide the surgical approach. Nonetheless, more evidence is still needed to standardize management. Detailed knowledge of the pathophysiology and the pathways of dissemination allows for the Implementation of effective surgical strategies tailored to each patient.
Keywords
Introduction
Descending necrotizing mediastinitis (DNM) is a rare and lethal infectious disease of the mediastinum secondary to an oropharyngeal infection.1 -3 Approximately 2% of patients with oropharyngeal infections develop it.4,5 Reported mortality rates range from 11% to 50% despite patients receiving definitive surgical intervention.2,3,6 -9 The cornerstone of treatment is drainage and surgical debridement of the involved cervical and mediastinal spaces, through transcervical and/or transthoracic routes depending on the extent of the disease. 5
We present the case of a 28-year-old male who sought care at a tertiary care institution with clinical manifestations consistent with DNM. This article aims to illustrate the optimal drainage approaches for surgical management, supported by a review of the pertinent literature. This report was prepared in accordance with the SCARE criteria. 10
Clinical Case
A 28-year-old male with no prior past medical history, including no history of immunosuppression or known risk factors for severe infection such as malnutrition, tobacco use, or chronic alcohol consumption, presented to a tertiary referral center with a 3-day course of odynophagia and fever, which 48 hours before admission progressed to include right-sided pleuritic pain and dyspnea. Upon admission, examination revealed pharyngeal erythema, tachycardia, tachypnea, and use of accessory respiratory muscles. Initial chest radiography revealed a right-sided pleural effusion. Laboratory evaluation revealed leukocytosis (25,600/µL), neutrophilia (23,000/µL), and elevated C-reactive protein levels (50.4 mg/L), with platelet count within normal range (294,600/µL), prompting the initiation of empirical intravenous antibiotic therapy with an aminopenicillin combined with a macrolide.
For the differential diagnosis of pulmonary thromboembolism, a computed tomography angiography (CTA) was performed, revealing pneumomediastinum and pneumothorax associated with bilateral loculated pleural effusions and inflammatory changes in the mediastinal fat. Given the suspicion of descending necrotizing mediastinitis with bilateral pleural empyema, the patient underwent urgent surgical intervention consisting of mediastinal and pleural drainage (Figure 1). Intraoperatively, bilateral thoracoscopic pleurectomy and pulmonary decortication were carried out, together with bilateral mediastinal drainage achieved via posterior mediastinotomy.
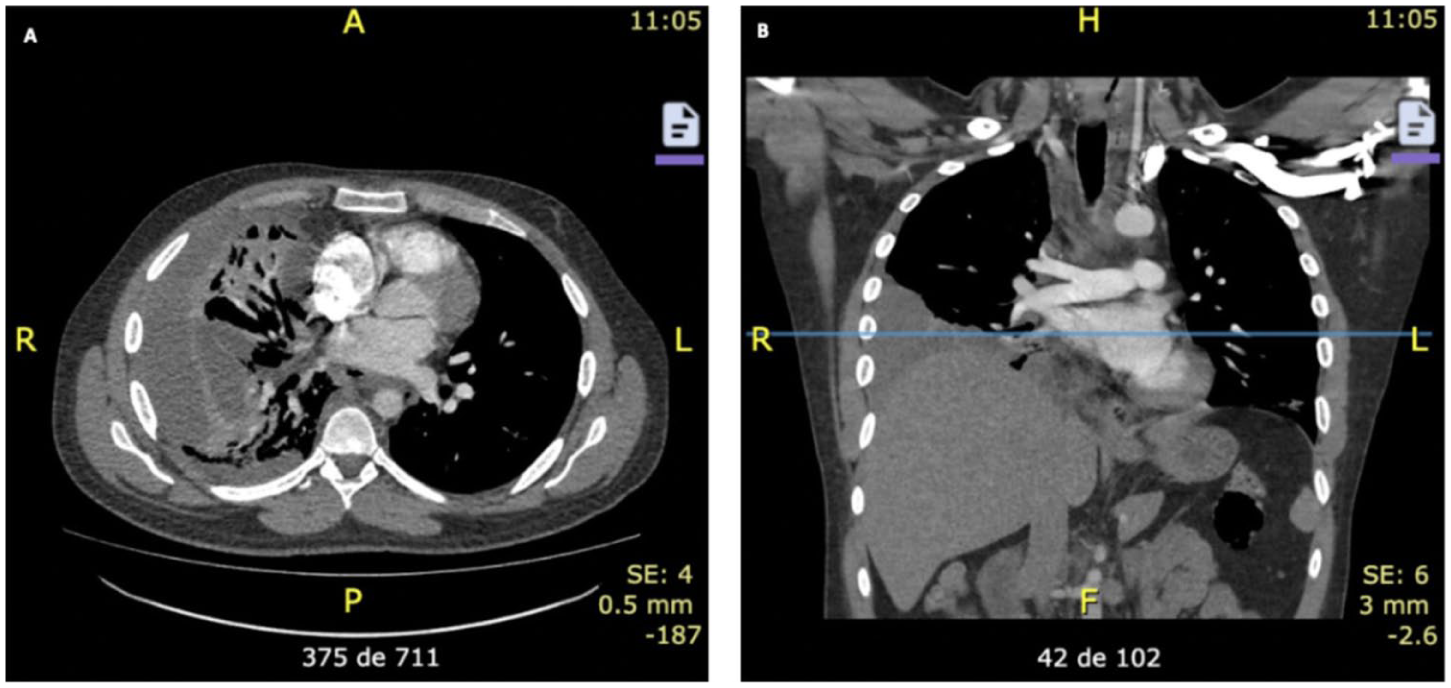
(A) Axial and (B) coronal chest CT scan obtained at admission showing pneumomediastinum and right hydropneumothorax with loculated fluid and inflammatory changes of the mediastinal fat.
During ICU follow-up, the patient showed clinical signs of systemic inflammatory response. Contrast-enhanced CT of the chest and neck reported a 21 cm3 collection adjacent to the left thyroid lobe, extending posteriorly from the upper third of the esophagus into the visceral mediastinum, measuring 46 mm × 79 mm × 130 mm, with an associated gas collection (Figure 2C). Three days after the initial CT, follow-up chest CT noted inflammatory changes in the mediastinal fat with right paratracheal and hilar lymphadenopathy, scant free fluid in the visceral space at the level of the diaphragmatic esophageal hiatus, and right pleural collections.

(A) Axial and (B) coronal 5 day follow-up chest CT scan showing free fluid in the visceral space at the level of the esophageal hiatus of the diaphragm with right pleural collections. (C) Axial neck CT scan demonstrating a collection adjacent to the left thyroid lobe extending posteriorly from the upper third of the esophagus toward the visceral mediastinum with approximate dimensions of 46 mm × 79 mm × 130 mm, a volume of 21 cc, and an associated intrathyroid gas collection on the left.
Intraoperative findings in the right hemithorax documented right pleural empyema with fibrinopurulent membranes and entrapment of the lower and middle lobes with 1000 cm3 of pus. A bulge of the posterior mediastinum below the carina was noted, with drainage of purulent material accompanied by periesophageal necrotic tissue. In the left hemithorax, a 300 cm3 pleural empyema was identified, devoid of fibrinopurulent membranes but with notable bulging of the posterior mediastinum. The patient remained in the intensive care unit (ICU) for 10 days, requiring invasive mechanical ventilation and vasopressor support for 2 days.
As a result, the patient underwent a second procedure consisting of mediastinal drainage via thoracoscopy combined with drainage of the cervical visceral space collection through cervicotomy (Figure 2A and B). Intraoperatively, a 20-cc retroesophageal abscess was identified, accompanied by an inflammatory reaction involving the prethyroid muscles and the cervical neurovascular bundle. Exploration of the right hemithorax showed pleural empyema with numerous fibrinopurulent membranes amounting to 700 cc, located between the right lower lobe, diaphragm, upper lobe, and paravertebral sulcus. In the left hemithorax, pleural empyema without fibrinopurulent membranes of 300 cc and bulging of mediastinal pleura at the level of the esophagus was observed.
During the first 2 weeks, the thoracostomy tubes and cervical drain were removed. He exhibited a pronounced improvement in both local and systemic inflammatory manifestations and regained tolerance to oral intake. Cultures of pleural and mediastinal membranes identified Streptococcus anginosus and Enterococcus faecalis of usual pattern, both sensitive to the previously instituted treatment. Antibiotic therapy was completed at home with ampicillin-sulbactam for 6 weeks from the date of the second surgical procedure. Outpatient follow-up over several months demonstrated a satisfactory clinical evolution, with no recurrence of the mediastinal infection or subsequent severe systemic infections.
Discussion and Literature Review
DNM is a rare, yet life-threatening disease arising from microbial contamination of the mediastinum. The literature describes that it most commonly affects adult patients and is associated with baseline comorbidities such as diabetes mellitus, hypertension, chronic kidney disease, and malignancy, as well as risk factors including alcohol abuse, chronic obstructive pulmonary disease, and poor dental health.3,4,12 Approximately 2% to 5% of oropharyngeal infections can progress to DNM, predominantly linked to odontogenic infections, tonsillitis, soft-tissue infections secondary to foreign bodies, and chronic sinusitis.2,3,12 Gravity plus the negative intrathoracic pressure facilitate the progression of microbial contamination through 1 or more cervical spaces of the deep cervical fascia. The infection spreads without anatomical barriers through the visceral space (pretracheal fascia), the vascular space (carotid sheath), and the retrovisceral space (prevertebral/retropharyngeal fascia), the latter being the main route. A relationship has been proposed between the cervical route of contamination and the area of mediastinal involvement. Dissemination through the pretracheal, vascular, and retrovisceral spaces has been associated with anterior, middle, and posterior mediastinal involvement, respectively.1,3,7,13,14 Sugio et al reported in a cohort of 225 patients with DNM that the retrovisceral space was the most frequently involved (60.9%), although 46.7% of patients had dissemination through multiple routes.
In 1983, Estrera et al suggested the following diagnostic criteria for DNM: (1) clinical manifestations of severe infection; (2) radiographic findings characteristic of the disease; (3) intraoperative documentation of necrotizing mediastinal infection; and (4) established association of oropharyngeal or cervical infection as the cause of the necrotizing mediastinal process. For the diagnosis to be established, at least 1 criterion must be met.3,11,13,15,16
Contrast-enhanced CT of the neck and chest represents a valuable tool for both diagnostic assessment and preoperative planning.4,16 Within the thoracic cavity, the presence of mediastinal inflammatory changes together with pneumomediastinum, pleural effusion, and pericardial effusion strongly indicates mediastinitis. Findings in the neck and chest enable identification of the infectious focus and facilitate the formulation of an appropriate plan for thoracic and/or transcervical drainage, if required.12,17 Moreover, the use of this tool is advised for monitoring patients during the postoperative period. 18 Although plain radiography offers low sensitivity and specificity, findings such as mediastinal widening or pneumomediastinum can strongly suggest the diagnosis.5,8 The innominate vein serves as an important radiological reference point to differentiate mediastinal from isolated cervical disease, thereby guiding the need for cervical drainage through cervicotomy with or without associated mediastinal drainage. 12
Endo et al proposed an anatomical classification according to the location of mediastinal inflammatory changes. Type I (44.4%) describes an infection localized in the superior mediastinum above the carina. Type II (56.6%) presents subcarinal inflammatory involvement. Type IIA implies anterior mediastinal involvement, and type IIB implies anterior and posterior mediastinal involvement.5,19 Because Endo’s classification fails to categorize posterior mediastinal involvement, it is considered limited and has prompted the development of various modifications. Sugio et al suggest adding type IIC, where the infection involves only the posterior mediastinum due to its high frequency (34.4% of type II) demonstrated in their cohort of 203 patients. 3 Type IIA infections are related to pretracheal fascial involvement, whereas type IIC infections are related to retrovisceral involvement. 3 Similarly, Guan et al proposed a classification that separates the mediastinum into superior and inferior compartments, with the inferior further subdivided into anterior and/or posterior regions, resulting in 4 distinct categories. 20
Treatment consists of surgical drainage complemented by antibiotic coverage. The surgical route is tailored according to the disease’s extent. Previous reports have recommended performing serial CT scans with transcervical and thoracic drainages as needed.12,21 The transcervical route allows drainage of the involved cervical spaces and the superior mediastinum, whereas transthoracic routes via thoracotomy or video-assisted thoracoscopy allow drainage of the inferior mediastinum. 5
Combined surgical management with cervicotomy and mediastinal drainage was proposed by Mihos et al. The cervical approach should achieve drainage and debridement of the pretracheal/visceral fascia and/or the prevertebral fascia. 13 The use of negative-pressure systems for cervical wound management has been reported, demonstrating evidence of reduced ICU stays and overall hospitalization time. 17 Mediastinal drainage entails debridement and evacuation of the superior and/or inferior mediastinum by incising the mediastinal pleura, followed by drainage, debridement, and irrigation through a mediastinotomy performed via posterolateral thoracotomy or video-assisted thoracoscopy. 13 Given the high frequency of associated pleural effusion and empyema, pulmonary decortication and pleurectomy are sometimes required. In cases where pericardial effusion, pericardiotomy should be performed. Patients with type I DNM benefit from a transcervical approach with dissection of the superior mediastinum via cervicotomy; however, this may be insufficient to achieve disease control, and these patients may therefore require additional interventions.3,5,14,18,19 Type IIA DNM requires a transthoracic mediastinal approach (open or video-assisted), although the possibility of a subxiphoid mediastinal approach without sternotomy has been described.13,20 In types IIB and IIC, transthoracic mediastinal drainage is always required, either by thoracotomy or video-assisted thoracoscopy. 19 Additionally, it has been reported that 34.9% of IIC cases require transcervical drainage, underscoring the importance of considering a retropharyngeal transcervical approach combined with transthoracic approaches. Likewise, in type I, IIA, and IIB mediastinitis, combined cervical and transthoracic drainage was required in 31.0%, 20.0%, and 11.3% of cases, respectively.3,5 Previously, combined transthoracic and cervical drainage was performed in only 2% of cases, with mortalities reaching up to 32%. 5 Addressing the collection adequately from the outset helps avoid reoperations—reported in up to 31%—as well as mortality and prolonged hospital stays.2,12
Growing interest in less invasive strategies has popularized the use of the thoracic approach through video-assisted thoracoscopy, which is considered a safe and effective alternative.17,22 Tanaka et al compared its use with thoracotomy, showing longer operative time, duration of mechanical ventilation, greater blood loss, and hospital stay, favoring the use of the thoracoscopic approach despite finding no differences in mortality. The study shows that the thoracotomy approach was performed mainly in type IIB mediastinitis, demonstrating that open surgery is still recognized as the most effective and safest way to drain complex mediastinal collections. Notably, drainage by thoracoscopy was associated with a higher reoperation rate. 16 More studies are needed to evaluate the effectiveness and outcomes of thoracoscopy for severe cases.
Limitations
This article describes a single case, which limits the generalizability of the findings. Additionally, management decisions were based on the clinical presentation and evolution of the patient and may not be applicable to all DNM cases. Further studies with larger cohorts are required to better define optimal surgical strategies for patients in this condition.
Conclusion
DNM is a rare disease with high morbidity and mortality, associated with mechanical ventilation, ICU stays, and prolonged hospitalizations. Due to improved diagnostic methods and optimal surgical drainage (transthoracic and transcervical), a reduction in overall mortality has been observed. The cornerstones of management consist of optimal antibiotic coverage and surgical debridement guided by the cervical and mediastinal involvement. The complementary classifications proposed by Endo and Sugio are a key tool to guide the surgical drainage approach; however, more information is still needed to standardize management. The case presented illustrates that a proper understanding of the disease and its routes of spread makes it possible to integrate effective, less invasive surgical strategies with lower morbidity, mortality, and reoperation rates.
Footnotes
Ethical Considerations
Approval was obtained from the Ethics Committee of Hospital Universitario San Ignacio.
Consent to Participate
Informed consent was obtained from the patient and her guardian for the publication of this work. A copy of the written informed consent is available for review by the Editor of this journal.
Consent to Participate
Written informed consent was obtained from the patient for publication of this report and accompanying images.
Author Contribution Statment
Carlos Solano and Natalia Restrepo-Abisambra contributed equally to the conception, design, and development of the manuscript. Natalia Restrepo drafted the manuscript, performed the literature review, and contributed to data interpretation. Carlos Solano contributed to patient identification, clinical management, and critical revision of the manuscript.
Sebastián Rodriguez, Mauricio Peláez, and Fernando Alvarado contributed to clinical data collection, patient management, and critical revision of the manuscript.
All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has no external sponsorship. It was funded by the researchers’ own means.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
AI Use Statement
The English translation of the original Spanish manuscript was assisted by ChatGPT (OpenAI, GPT-5), used exclusively for translation purposes without generating or modifying scientific content. Grammar and spelling were reviewed using Grammarly.