
Abstract
Duodenal obstruction in the setting of situs inversus abdominis is an uncommon clinical finding. We report 2 neonates who presented with bile-stained vomiting and abdominal distension. Diagnostic workup, including radiography and ultrasonography, confirmed the diagnosis of situs inversus abdominis with duodenal obstruction due to annular pancreas in the first case and due to intestinal malrotation in the second. A Ladd’s procedure was successfully performed to relieve the obstruction. Both patients recovered well, initiating full enteral feeds and were subsequently discharged. These cases underscore the diagnostic challenges posed by this rare association and highlight that a standardized surgical approach, adapted to the mirror-image anatomy, can lead to a successful outcome. Early recognition and tailored intervention are crucial in the management of these complex patients.
Introduction
Situs inversus, a rare condition (1 in 8500 people), involves mirror-image positioning of thoracic and abdominal organs.1,2 It is classified as situs inversus with levocardia or dextrocardia, terms which refer only to the left or right direction of the cardiac apex at birth, not the chamber orientation. 1 Isolated dextrocardia (situs solitus with dextrocardia) features a right-pointing apex with otherwise normal visceral arrangement. In contrast, situs inversus with dextrocardia, or situs inversus totalis (incidence 1 in 8000 births), is a complete mirror image of the normal anatomy, while situs inversus with levocardia is rarer (1 in 22 000 births). 1 When situs is indeterminate, situs ambiguous (heterotaxy) exists, with an incidence of 1 in 10 000 births, accounting for 4% of congenital heart disease (CHD) and featuring anomalies like atrial septal defect and common AV canal. 1 Situs inversus totalis patients seldom have other malformations, though they are slightly more frequent than in situs solitus.3,4 For invasive surgery, a mirror-image technique is used, requiring surgeons to adapt port placements and overcome the challenge of operating from the opposite side. While the surgical management of intestinal malrotation in situs anomalies is well-described, the specific anatomical constellation presented in these cases—the association of duodenal obstruction with polysplenia and anticlockwise (reverse) intestinal rotation—constitutes a rare and surgically nuanced variant. This report highlights this distinct combination, emphasizing the diagnostic and technical adaptations required beyond the standard application of Ladd’s procedure in a mirror-image abdomen.
This work was reported in accordance with CARE guidelines (for case reports, Supplemental Material). 5
Case Presentation

Preoperative and postoperative radiographic findings: (A) an upright abdominal radiograph (erect view) demonstrates the “reversed double bubble” sign, characterized by 2 large air-fluid levels in the upper abdomen and (B) a postoperative abdominal radiograph (babygram) confirms the passage of intraluminal gas into the distal bowel, indicating successful surgical relief of the obstruction and the re-establishment of bowel continuity.
Laparotomy confirmed the diagnosis of situs inversus abdominis with duodenal obstruction due to an annular pancreas and associated reverse (anticlockwise) rotation. Findings included a left-sided liver and duodenum (Figure 2A), a right-sided stomach with polysplenia (Figure 2B and C), accompanying intestinal malrotation, and a left upper quadrant cecum and appendix (Figure 2D). A Ladd’s procedure with duodenoduodenostomy was performed to relieve the obstruction (Figure 2E).

Imaging and intraoperative findings in a case of situs inversus abdominis with annular pancreas and polysplenia: (A) left-sided duodenum demonstrating obstruction secondary to annular pancreas, (B) multiple splenic tissues (polysplenia) located on the right side of the abdomen, (C) right-sided stomach and spleen, (D) caecum and appendix positioned in the left upper quadrant, and (E) duodenoduodenostomy performed to relieve the duodenal obstruction caused by annular pancreas.
The postoperative course was marked by initial bilious nasogastric output, which ceased following the passage of green mucoid stool on day 3 (Figure 1B). Vomiting resolved, and enteral feeding was gradually advanced via infusion pump. Full enteral feeds were successfully achieved, and the patient was discharged on postoperative day 20. Then continued with monthly follow-up at the outpatient clinic for 3 months (No symptoms or complaints). The mother is still in contact with us for reassurance.

Erect abdominal X-ray with contrast demonstrating situs inversus with right-sided gastric shadow, left-sided liver shadow, and left-sided duodenojejunal (DJ) junction.
Surgical exploration confirmed situs inversus abdominis with a left-sided liver and duodenum (Figure 4A) and a right-sided stomach and spleen (Figure 4B). Duodenal obstruction due to intestinal malrotation with reverse rotation was identified, with the cecum and appendix situated in the left upper quadrant (Figure 4C). A standard Ladd’s procedure was performed (Figure 4D).
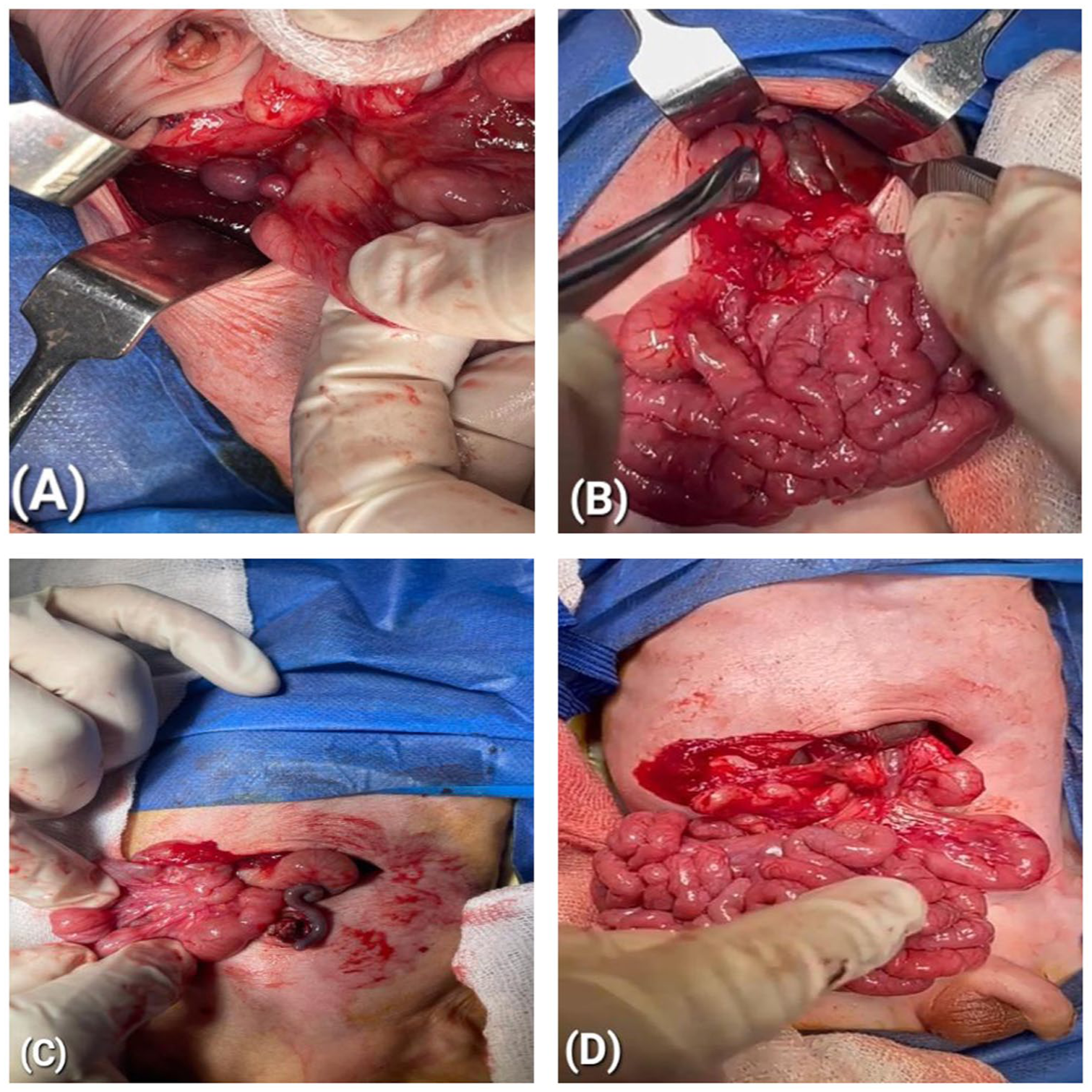
Images during the surgery: abdominal situs inversus with polysplenia and findings at surgery: (A) image demonstrating multiple splenic tissues (polysplenia) in the right upper abdomen, (B) the stomach is positioned in the right upper abdomen, (C) the cecum and appendix are located in the left upper abdomen, and (D) intraoperative image showing the performed Ladd’s procedure.
Postoperatively, bilious drainage diminished significantly and ceased after the passage of stool on the second day. Oral feeding was initiated and progressively advanced, with full feeds tolerated prior to discharge on postoperative day 15. Then continued with monthly follow-up at the outpatient clinic for 3 months (No symptoms or complaints). The mother is still in contact with us for reassurance.
Discussion
Situs inversus is a congenital anomaly characterized by transposition of internal organs from their normal anatomical position (situs solitus).6,7 In situs inversus totalis, there is complete right-to-left reversal, resulting in dextrocardia, a trilobed left lung, a bilobed right lung, a left-sided liver and gallbladder, and a right-sided stomach and spleen.3-8 The etiology is multifactorial, involving autosomal recessive genes, maternal diabetes, and other factors, though no such history was present in our cases.1-3,9 Situs inversus can be asymptomatic and incidental, but it presents early in neonates when associated with intestinal obstruction, as seen here.7,10
Diagnosis is difficult by physical examination alone but is suggested by radiographs showing a “reversed double bubble” sign—a dilated left-sided stomach and right-sided duodenum in Case A, and reversed gastric and hepatic impressions in Case B. 11 Ultrasound confirmed polysplenia in both cases. Echocardiography is crucial for evaluating congenital heart disease (CHD); Case A had an ASD, and Case B had a PFO. The risk of CHD is relatively high if the cardiac apex and stomach are on opposite sides. 12 CHD is a major determinant of survival in these neonates. 12
Gastrointestinal abnormalities, such as annular pancreas or intestinal malrotation leading to duodenal obstruction, are common. 13 Annular pancreas is theorized to result from incomplete rotation of the ventral pancreatic bud during the eighth week of development. 14 The preferred surgical procedure for duodenal obstruction is diamond-shaped duodenoduodenostomy, applicable via laparotomy or laparoscopy for most cases, including duodenal web, without injuring the pancreatobiliary system. 14 Outcomes depend on associated anomalies, with potential complications including anastomotic leakage and sepsis, while long-term issues like vomiting occur in one-third of patients. 14
Diagnostic reliance on classic radiologic signs like the “double bubble” can be misleading in situs anomalies if not meticulously interpreted in the context of mirrored anatomy, potentially delaying intervention. 12 Intraoperatively, the mirror-image arrangement demands deliberate mental reorientation; standard maneuvers must be consciously reversed to safely address malrotation and avoid iatrogenic injury. 15 Furthermore, perioperative risk stratification is crucial, as associated anomalies like polysplenia or congenital heart disease significantly influence physiologic reserve and postoperative recovery, necessitating tailored multidisciplinary planning. 12
The salient feature in both presented cases was duodenal obstruction—due to annular pancreas in the first case and intestinal malrotation in the second —coexisting with polysplenia and anticlockwise (reverse) intestinal rotation, a particularly rare anatomical subtype. This variant necessitates deliberate intraoperative interpretation and modification of standard surgical maneuvers to achieve safe derotation and duodenal patency. Our experience underscores that recognizing this specific anatomical pattern is crucial for preoperative planning and may influence the postoperative feeding trajectory, highlighting an insight beyond the general principle of performing a Ladd’s procedure in situs inversus. The necessary technical adaptation involved performing an appendectomy, dissecting Ladd’s bands, widening the mesenteric root, and deliberately repositioning the bowel—placing the small intestine on the left and the large intestine on the right—which constituted a conscious clockwise derotation maneuver tailored to the anticlockwise rotation and mirror-image anatomy.
This report is limited by its retrospective nature and small number of cases, which restricts generalizability. Follow-up was short, and long-term outcomes such as adhesive obstruction or recurrence remain unknown. Nonetheless, given the extreme rarity of this specific anatomical constellation—duodenal obstruction with anticlockwise rotation and polysplenia—these cases offer practical insights that may assist surgeons encountering similar findings. Collaborative multi-institutional efforts would strengthen future evidence.
Conclusion
Neonates with bilious vomiting and suspected situs anomalies require a high index of suspicion and systematic diagnostic evaluation. Radiographic and ultrasonographic assessment should be meticulously interpreted within the context of mirrored anatomy to avoid delays. When surgical intervention is indicated, a tailored approach—adapting standard procedures such as Ladd’s to the reversed anatomy and anticipating associated anomalies like polysplenia or congenital heart disease—is essential for safe and effective management. Awareness of this rare association and a structured diagnostic-surgical pathway can optimize outcomes even in anatomically complex presentations.
Supplemental Material
sj-docx-1-icr-10.1177_11795476261432010 – Supplemental material for Rare Association of Duodenal Obstruction and Situs Inversus Abdominis: A Two Case Report
Supplemental material, sj-docx-1-icr-10.1177_11795476261432010 for Rare Association of Duodenal Obstruction and Situs Inversus Abdominis: A Two Case Report by Khalid Elsaied Ali Shreef, Abdelrazek Yousef, Ahmad Alkheder, Khaled Alsayed Abualkhair, Khaled Mosad, Amr Elshaer and Amr Elsafy in Clinical Medicine Insights: Case Reports
Footnotes
Acknowledgements
The authors would like to appreciate the patients’ families for their utmost cooperation.
Ethical Considerations
Ethical approval for the publication of this case report was waived by the institutional review board of our university, as per its policy for case reports that do not contain patient images or personal identifying information.
Consent to Participate
Written informed consent was obtained from the patients’ legal guardian for publication of this case report and accompanying images.
Author Contributions
Ahmad Alkheder and Khaled Alsayed Abualkhair: Validation, Writing – review & editing, Visualization, Methodology, Software, Writing – original draft, Formal analysis. Khalid Elsaied Ali Shreef and Khaled Mosad: Validation, Writing – review & editing, Visualization, Methodology, Software, Writing – original draft, Formal analysis. Amr Elshaer: Validation, Formal analysis, Writing – review & editing. Amr Elsafy: Validation, Formal analysis, Writing – review & editing. Abdelrazek Yousef: Supervision, Writing – review & editing, Project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.