
Abstract
Background:
Foreign body aspiration (FBA) in adults is rare and often overlooked, presenting with nonspecific pulmonary symptoms that may mimic recurrent infections or malignancy. Delay in diagnosis can lead to prolonged morbidity and mismanagement.
Case Presentation:
We report a 55-year-old woman with a 2-month history of productive cough, intermittent hemoptysis, dyspnea, pleuritic chest pain, and recurrent pneumonia unresponsive to multiple courses of antibiotics and corticosteroids. Chest X-ray revealed right middle-lobe collapse, while computed tomography demonstrated a linear radiopaque lesion in the right middle-lobe bronchus. Flexible bronchoscopy confirmed complete bronchial obstruction by purulent debris concealing a sharp chicken bone fragment, which was retrieved successfully. The patient showed rapid clinical improvement following removal.
Conclusion:
This case underscores the importance of considering FBA in the differential diagnosis of persistent atelectasis or treatment-resistant pneumonia in adults, even in the absence of aspiration history or risk factors. Diagnostic bronchoscopy remains the gold standard, enabling both definitive diagnosis and therapeutic intervention, thereby preventing misdiagnosis as neoplasm and avoiding unnecessary procedures.
Introduction
Foreign body aspiration in adults is an uncommon but potentially serious condition, accounting for only a small proportion of airway emergencies compared to children.1,2 Unlike in children, where aspiration events are often witnessed, adults may not recall a choking episode, leading to delayed recognition, presentation, and treatment.2,3 The clinical presentation is usually nonspecific and can mimic other respiratory illnesses such as pneumonia, asthma, or even malignancy.1,4
Atelectasis and chronic recurrent pneumonia are familiar complications of undiagnosed endobronchial obstruction.5,6 In cases where lobar collapse or nonresolving consolidation persists despite appropriate medical therapy, physicians should suspect obstructive causes, such as neoplastic lesions, strictures, or foreign bodies.3,5
Flexible bronchoscopy remains the gold standard for both diagnosis and treatment, as it allows direct visualization of the airway, identification of the obstructive lesion, and safe retrieval of aspirated material.1,7
We present a rare case of prolonged atelectasis and recurrent pneumonia in a 55-year-old woman, secondary to an unsuspected chicken bone aspiration. This case highlights the diagnostic challenges of adult foreign body aspiration and the importance of maintaining a high index of suspicion in patients with persistent or unexplained pulmonary symptoms.
Case Presentation
A 55-year-old female presented to the pulmonary clinic with a 2-month history of a persistent productive cough with whitish expectoration, intermittent hemoptysis, dyspnea, pleuritic chest pain on the right side, associated with fever, and fatigue. She had been previously treated multiple times with antibiotics, bronchodilators, and corticosteroids with minimal clinical improvement. There was no history of alcohol consumption or underlying neurological disease. She denied any significant smoking history or known allergies. The patient did not recall any history of aspiration.
Physical Examination showed stable vital signs. Chest auscultation revealed decreased breath sounds and crackles over the right mid-to-lower lung field.
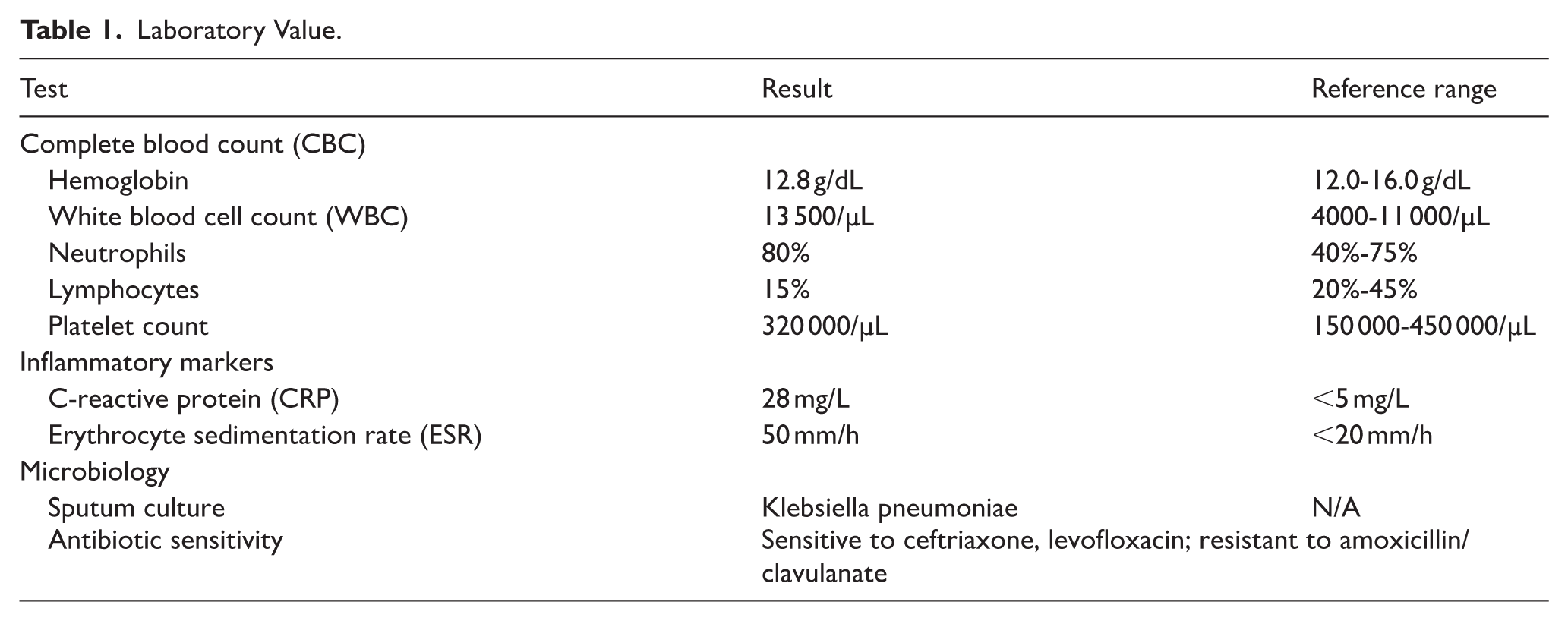
Complete blood count showed a mild leukocytosis with neutrophilia (Table 1). Sputum Culture revealed growth of Klebsiella species. Chest X-ray showed a right mid-lung zone opacity with volume loss. CT scan of the chest revealed right middle lobe collapse with consolidation (Figure 1) which clearly showed a linear, radiopaque foreign body within the right middle lobe bronchus, causing obstructive atelectasis. The primary differential was an aspirated foreign body, with the need to rule out an endobronchial lesion obscured by post-obstructive inflammation. Given the radiological finding of a foreign body with persistent lobar collapse resistant to medical treatment, a diagnostic and therapeutic flexible bronchoscopy was performed under conscious sedation.
Laboratory Value.

CT scan of the chest revealed right middle lobe collapse with consolidation (red arrow).
The examination revealed a complete obstruction of the right middle lobe bronchus by a mass of thick, purulent secretions and inflammatory debris. After careful suctioning and irrigation to clear the exudate, the core of the obstruction was visualized: a sharp, linear, whitish foreign body identified as a chicken bone fragment approximately 1.5 cm in length (Figure 2), which was firmly embedded in the bronchial wall. Using rigid grasping forceps introduced through the bronchoscope’s working channel, the bone fragment was successfully disimpacted and retrieved in its entirety. The bronchial mucosa at the impaction site was noted to be severely inflamed and edematous, which was the likely source of her initial hemoptysis. Immediately following the removal, the right middle lobe was observed to begin re-expanding.

Whitish foreign body identified as a chicken bone fragment approximately 1.5 cm in length.
After the procedure, the patient reported that 2 months prior, she had choked when eating chicken. She had a severe coughing fit and a single episode of hemoptysis, but she had chosen not to seek medical advice at the time. The patient’s postoperative course was uneventful. Her cough resolved dramatically within 24 hours. A follow-up chest X-ray 1 week later showed complete resolution of the right middle lobe atelectasis. The patient was asymptomatic at her 1-month follow-up and had returned to her normal daily activities.
Discussion
Foreign body aspiration (FBA) in adults is an uncommon clinical scenario, yet it can have serious consequences if not promptly addressed. Unlike children, whose aspiration incidents are often witnessed, adults typically present with vague respiratory symptoms and have difficulty recalling the aspiration event. This often leads to diagnostic delays, during which complications such as recurrent pneumonia, lobar atelectasis, or even bronchiectasis can arise.8,9
We report the case of a 55-year-old woman with a 2-month history of persistent cough, paroxysmal fever, and refractory pneumonia, in whom bronchoscopy revealed an obstructing chicken bone fragment. This presentation aligns with documented observation in the literature, where delayed diagnosis in adults with FBA is not uncommon. Özer et al. found that 17.6% of adult FBA patients experienced a “late diagnosis,” with an average delay of more than 22 months, often initially misdiagnosed as malignancy or chronic infection. 8 Similarly, Limper and Prakash reported that most adults with FBA were initially diagnosed with asthma, pneumonia, or tumor, only to have the true cause identified through bronchoscopy. 2
Radiographic findings may contribute to this diagnostic challenge. Plain chest radiographs may appear normal in many cases, and nonspecific findings like atelectasis or chronic consolidation are usually attributed to infection or tumor.10,12 While computed tomography (CT) is more sensitive, it can mistakenly identify a foreign body embedded in granulation tissue as an endobronchial neoplasm. 9 In our case, CT evidence of lobar collapse and an endobronchial opacity highly suggested malignancy, underscoring the need for endoscopic confirmation.
The microbiologic profile further complicates interpretation. Post-obstructive infection such as those caused by gram-negative organisms like Klebsiella pneumoniae are frequently associated with FBA. 11 In our patient, isolation of Klebsiella and the elevated inflammatory indices initially suggested bacterial pneumonia. However, the persistence of symptoms despite treatment highlighted the importance of the differential diagnosis.
Bronchoscopy remains the gold standard for both diagnosis and treatment. While flexible bronchoscopy is generally safe, accessible, and effective, rigid bronchoscopy may be necessary for large or impacted foreign bodies.9,10 In this case, flexible bronchoscopy in this patient enabled direct visualization and removal of the foreign body, leading to immediate re-expansion of the lung and rapid clinical improvement. The literature consistently supports that performing bronchoscopy in cases of unexplained lobar atelectasis or treatment resistant pneumonia improves outcome and prevents unnecessary delays in therapy.2,8
This case underscores the critical importance of maintaining a broad differential diagnosis when an adult presents with persistent atelectasis. Diagnostic delays often stem from not considering aspiration, especially in patients without classic risk factors such as neurological disease, alcohol intoxication, or altered mental status. 12 Clinicians should undertake the following: (i) conduct repeated and targeted histories to identify subtle aspiration events, (ii) suspect obstruction in cases of chronic radiographic abnormalities, and (iii) lower the threshold for diagnostic bronchoscopy when conventional therapy fails. As Boyd et al demonstrate, early bronchoscopy not only establishes the diagnosis but also prevents late complications and misdiagnosis of malignancy. 12
The main limitation of this study was the inability to obtain a CT image that clearly visualized the foreign body. There were no limitations related to the diagnostic approach or the interventional management.
Conclusion
Adult foreign body aspiration often presents with nonspecific symptoms and is frequently misdiagnosed, commonly as pneumonia or malignancy, leading to lobar collapse before recognition. This case highlights that foreign body aspiration in adults, although uncommon, should be considered in patients with persistent atelectasis. Early bronchoscopy can change the clinical course, reduce morbidity, prevent delays in diagnosis and unnecessary treatment.
Footnotes
Author Contributions
Z.W.E. contributed to the study conception, drafting the manuscript, and clinical data acquisition. M.A.B. literature review, and drafting of the initial manuscript. M.J. drafting, and critical revision of the manuscript. N.A. supervised the study, and performed final manuscript review and editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent to Participate
Written informed consent was obtained from the patient for publication of this case report and accompanying images. Ethical approval was not required for this case report.