
Abstract
Internal abdominal hernias are rare causes of small bowel obstruction but carry a high risk of strangulation and bowel ischemia if not promptly recognized. We report the case of a 92-year-old man with a virgin abdomen who presented with acute abdominal pain and was found on computed tomography to have a closed-loop obstruction with a mesenteric “whirl sign.” Emergency laparotomy revealed the presence of a necrotic colonic loop strangulated by an internal adhesion with no history of prior abdominal surgery or trauma. Segmental colectomy with creation of a protective double-barrel ileostomy was performed, followed by uneventful recovery and subsequent reversal of the ileostomy. This case highlights the importance of considering internal hernia in elderly patients with bowel obstruction and no previous surgery, the value of CT and the “whirl sign” in raising early suspicion of a closed-loop process, and the need for timely surgical intervention to prevent any irreversible ischemic injury.
Introduction
Internal abdominal hernias are defined as the protrusion of intra-abdominal viscera through a normal or abnormal peritoneal or mesenteric aperture within the confines of the peritoneal cavity. They account for a small proportion of cases of intestinal obstruction, with an estimated incidence of 0.2% to 0.9% in autopsy series and 0.6% to 5.8% of all small bowel obstructions.1-4 These hernias may be congenital, related to normal peritoneal recesses or developmental defects, or acquired, most commonly in the setting of previous abdominal surgery, trauma, inflammatory adhesions, or bariatric and colorectal procedures.1-3,5,6
Several classifications have been proposed, typically based on the anatomic site of the defect and type of peritoneal aperture. The most frequent entities include paraduodenal, foramen of Winslow, pericecal, transmesenteric, transmesocolic, sigmoid-mesocolon-related, transomental, supravesical, pelvic, and postoperative (for example, Roux-en-Y anastomosis-related) internal hernias.2,3,5,6 In contemporary series, paraduodenal hernias are reported as the most common congenital subtype, whereas acquired internal hernias have become increasingly prevalent with the widespread use of laparoscopic and reconstructive gastrointestinal surgery.3,5,6
Despite their rarity, internal hernias represent a surgical emergency because they frequently present as strangulating closed-loop obstruction, with reported mortality rates reaching 50% when diagnosis and treatment are delayed.3-6 Clinical manifestations are nonspecific and range from intermittent, vague abdominal discomfort to acute abdomen with signs of sepsis and shock. Cross-sectional imaging, particularly multidetector CT, plays a central role in preoperative diagnosis by demonstrating clustered or displaced loops of bowel, transition points, mesenteric crowding, and characteristic vascular findings such as convergence and twisting of mesenteric vessels at the hernia orifice.3,5,6
Adhesive internal hernias occurring in a virgin abdomen, where no prior surgery or trauma has been documented, are exceptionally uncommon and easily overlooked in the differential diagnosis of bowel obstruction.4,6,7 We present a case of strangulated internal hernia due to an internal adhesion in an elderly patient with no surgical history, emphasizing the diagnostic contribution of CT, the significance of the whirl sign, and the implications for urgent surgical management. The clinical data and sequence of events are based on the patient described in the original draft.
Case Presentation
A 92-year-old man with a medical history of hypertension and long-standing chronic constipation, but no previous abdominal or pelvic surgery and no history of abdominal trauma, presented to the emergency department with acute onset severe diffuse abdominal pain of 1 day’s duration. The pain was progressive and colicky in nature. He reported obstipation since the morning of presentation, with no passage of flatus or stool thereafter. There was no associated vomiting, fever, chest pain, or urinary symptoms.
On arrival, the patient was afebrile with a blood pressure of 165/82 mmHg and a heart rate of 100 beats/minute. Oxygen saturation was within normal limits on room air. Abdominal examination revealed marked distention with generalized tenderness and hyper-tympanism. No guarding or rebound tenderness was initially noted, and there were no palpable masses or hernias. Bowel sounds were decreased. Digital rectal examination showed an empty rectum. Laboratory investigations demonstrated leukocytosis with a white blood cell count of 17 300 × 109/L and a left shift with 78.6% neutrophils. Serum lactate was markedly elevated at 8.8 mmol/L, and C-reactive protein was 38.01 mg/L. Serum creatinine was mildly elevated at 1.57 mg/dL, while hemoglobin, liver enzymes, pancreatic enzymes, and bilirubin were within normal limits. High-sensitivity troponin was negative. These findings raised concern for evolving bowel ischemia in the setting of acute intestinal obstruction. An urgent computed tomography scan of the abdomen and pelvis was performed without intravenous contrast because of impaired renal function. The examination demonstrated a markedly distended colonic segment forming a focal closed-loop configuration, associated with mesenteric crowding and surrounding inflammatory stranding. There was a clear twisting of mesenteric fat and vessels around a central axis at the level of the first sacral vertebra, producing a characteristic mesenteric “whirl sign.” The involved vessels appeared tightly spiraled and convergent toward a single point, consistent with torsion at the site of an internal aperture. A small amount of adjacent free fluid was present, further raising concern for venous congestion and evolving ischemia. Although the absence of intravenous contrast limited direct assessment of bowel wall enhancement, the combination of closed-loop morphology, focal mesenteric vessel twisting, and peritoneal fluid corresponded closely to the structured CT features of strangulating internal hernia and strongly suggested a surgical emergency (Figure 1).
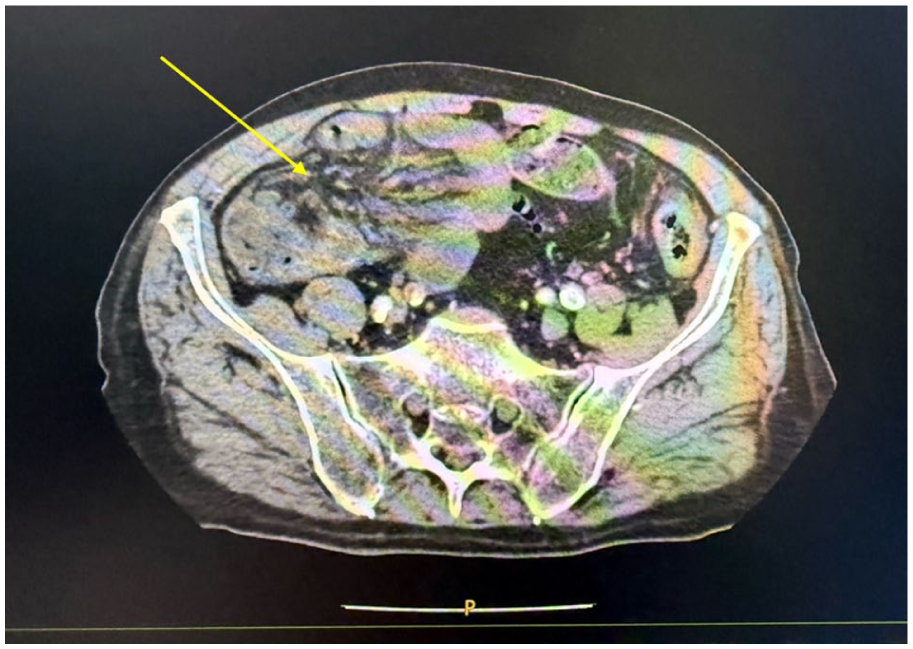
Axial non-contrast computed tomography image of the abdomen demonstrating a mesenteric “whirl sign” (arrow), characterized by twisting of mesenteric fat and vessels around a central axis at the level of the first sacral vertebra. The converging spiraled mesenteric vessels and adjacent distended colonic loop are consistent with a closed-loop obstruction and strongly suggest a strangulating internal hernia.
Given the patient’s advanced age and absence of prior abdominal surgery, several alternative diagnoses were considered. Sigmoid volvulus was contemplated; however, the CT scan did not demonstrate the typical massively dilated sigmoid colon with a “coffee-bean” configuration or mesocolic torsion. Primary intestinal volvulus unrelated to adhesions was also considered but was deemed less likely given the focal nature of the mesenteric twisting and the absence of congenital malrotation or diffuse small bowel involvement. Stercoral colitis was considered in the context of chronic constipation, yet imaging did not reveal fecaloma-associated colonic wall ulceration or pressure necrosis, and the mesenteric whirl sign suggested a mechanical closed-loop process rather than primary inflammatory pathology. Acute mesenteric ischemia of vascular origin was considered less likely due to the lack of embolic risk factors, absence of atrial fibrillation, and the presence of localized rather than diffuse ischemic changes. Overall, the constellation of clinical deterioration, marked lactic acidosis, and CT evidence of a focal mesenteric whirl sign strongly favored a strangulating internal hernia as the leading diagnosis.
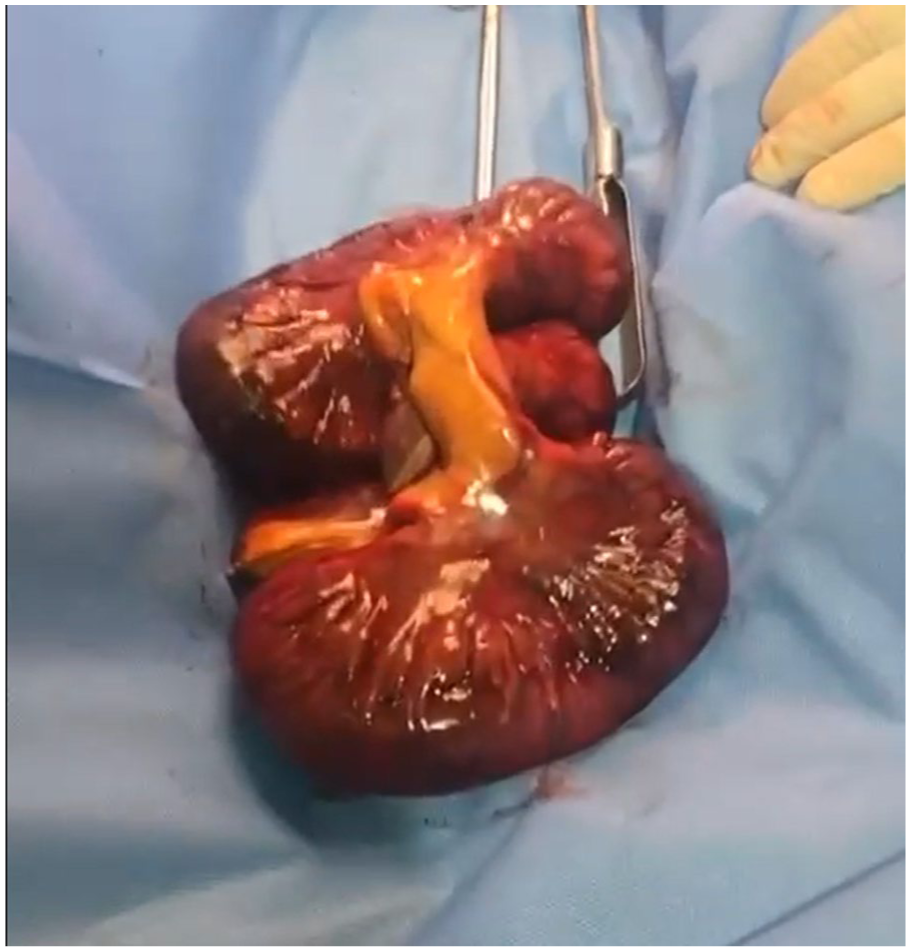
Intraoperatively, a segment of colon was found herniated through a solitary fibrous adhesive band forming a narrow internal aperture. The band extended between adjacent mesenteric leaves and did not correspond to any recognized congenital peritoneal recess, such as a paraduodenal or transmesenteric defect, suggesting an acquired idiopathic adhesion. The entrapped colonic segment was rotated around this fixed point, resulting in a closed-loop configuration with marked venous congestion and transmural ischemia, while the remaining small bowel appeared viable (Figure 2). No additional adhesions, inflammatory changes, or evidence of prior intra-abdominal insult were identified, supporting the diagnosis of an isolated adhesive internal hernia in a virgin abdomen.

Intraoperative photograph showing a strangulated colonic segment with marked venous congestion and transmural ischemia following herniation through a solitary fibrous adhesive band. The dark discoloration and loss of normal bowel sheen indicate nonviable bowel.
Given the patient’s advanced age, markedly elevated lactate level, and the presence of ischemic colonic bowel, a primary anastomosis was considered high risk. Therefore, segmental colectomy with creation of a protective double-barrel ileostomy was elected to minimize the risk of anastomotic leak and postoperative morbidity (Figure 3). The mesenteric defect was carefully closed to prevent recurrence, and the abdomen was closed in standard fashion.
Resected colonic segment following segmental colectomy, demonstrating gross ischemic changes consistent with irreversible bowel necrosis secondary to closed-loop obstruction.
Postoperatively, the patient was managed in the surgical ward. He was kept nil per os (NPO) for 3 days, during which he remained hemodynamically stable without signs of sepsis, and the ileostomy became functional with passage of gas. A liquid diet was then progressively introduced and advanced as tolerated. The remainder of his postoperative course was uneventful. Six weeks after the index operation, he was readmitted for elective reversal of the ileostomy. Restoration of bowel continuity was completed without complication, and the patient was discharged home on postoperative day 2, with regular bowel function and no residual abdominal symptoms at follow-up.
Discussion
Internal abdominal hernias, although uncommon, are a clinically important cause of acute intestinal obstruction with a disproportionately high risk of strangulation and ischemic bowel when compared with more prevalent etiologies such as postoperative adhesions or external hernias.1-6 Classic radiologic and surgical series have estimated that internal hernias account for ~0.6% to 5.8% of all small bowel obstructions, with an autopsy incidence of 0.2% to 0.9%.1-4,7 The rarity of these lesions, their often nonspecific presentation, and the absence of previous surgery in some patients contribute to frequent diagnostic delay and the potential for catastrophic outcomes.3-6
From a pathophysiologic standpoint, internal hernias result from herniation of bowel through a mesenteric or peritoneal aperture that may be congenital or acquired. Congenital defects include paraduodenal fossae, foramen of Winslow, pericecal recesses, and anomalies of the sigmoid mesocolon, whereas acquired defects occur after trauma, inflammation, transplantation, or reconstructive gastrointestinal surgery.1-3,5,6 In the present case, there was no history of surgery or trauma and no obvious congenital sac or classic anatomic recess; instead, a fibrous adhesive band formed a narrow internal aperture through which colon herniated and became strangulated. This pattern is consistent with an adhesive internal hernia in a so-called virgin abdomen, an entity that has been increasingly recognized but remains rare in the literature.4,6,7 Chronic constipation and raised intra-abdominal pressure in this elderly patient may have contributed to the development or tightening of the adhesive band and to herniation of bowel through the defect, although this relationship remains speculative.
The pathogenesis of adhesive internal hernia in a virgin abdomen remains incompletely understood. Several mechanisms have been proposed, including the presence of congenital peritoneal bands that may remain clinically silent until later in life, as well as idiopathic fibrous adhesions arising without an identifiable antecedent event. Subclinical inflammatory processes, minor abdominal trauma, or repeated episodes of increased intra-abdominal pressure may also contribute to localized peritoneal injury and subsequent adhesion formation. Akyildiz et al emphasized the heterogeneity and complexity of internal hernia etiologies, noting that a clear precipitating factor is often absent, particularly in non-postoperative cases. In elderly patients, long-standing constipation and chronic straining may further exacerbate these mechanisms by promoting repetitive mechanical stress on the mesentery, potentially facilitating herniation through a pre-existing or newly formed fibrous band. 4
The present case also underscores the pivotal role of CT in the diagnosis of internal hernias. Multidetector CT is now considered the first-line imaging modality for suspected small bowel obstruction because it allows precise localization of the transition point, assessment of closed-loop configuration, and evaluation of secondary signs of ischemia, such as mesenteric edema, free fluid, reduced or absent mural enhancement, and pneumatosis.3,5-7 Several reviews have described characteristic CT findings associated with specific types of internal hernia, including sac-like clusters of bowel loops in abnormal locations, engorged and converging mesenteric vessels at the hernia orifice, and displacement of anatomic landmarks such as the duodenum, colon, or stomach.2,3,5,6 In our patient, even in the absence of intravenous contrast because of renal impairment, the CT scan clearly demonstrated a mesenteric whirl sign associated with a closed-loop configuration and adjacent fluid, which strongly suggested a strangulating lesion and prompted urgent operative intervention.
The “whirl sign” refers to the CT appearance of spiraled or twisted bowel and mesenteric vessels around a central point. Its presence is highly specific for volvulus or closed-loop obstruction, although sensitivity is limited.8,9 Duda et al reported that patients with a whirl sign were significantly more likely to require surgery for small bowel obstruction than those without this sign. 8 Subsequent case-based reports and pictorial essays have reinforced the importance of recognizing the whirl sign as a radiologic red flag that should lower the threshold for operative management, particularly in the setting of clinical and laboratory features suggestive of strangulation, such as severe pain, leukocytosis, and elevated lactate. 9 In the present case, the combination of severe acute pain, marked lactic acidosis, and CT evidence of a whirl sign was treated as a surrogate marker of bowel compromise, and the decision for emergent laparotomy allowed timely resection of frankly necrotic bowel before the development of perforation or diffuse peritonitis.
Although most internal hernias described in the literature are either congenital or postoperative, a limited number of case reports have documented adhesive or idiopathic internal hernias occurring in patients with no prior abdominal surgery. Several authors have reported isolated fibrous bands causing strangulating internal hernias in virgin abdomens, often presenting with acute bowel obstruction and a high risk of ischemia at the time of diagnosis. These reports consistently emphasize the diagnostic challenge posed by the absence of surgical history and the critical role of CT imaging in raising early suspicion.10-12 Within the classification frameworks described by Ghahremani, Mathieu et al, and Martin et al, the present case does not conform to a classic congenital recess or postoperative defect, but rather represents an acquired, non-postoperative adhesive internal hernia, a rare subset within the broader spectrum of internal hernias.1-3 By documenting a colonic strangulation caused by a solitary adhesive band in an elderly patient, this case expands the limited body of evidence supporting the existence of idiopathic adhesive internal hernias and reinforces the need for heightened diagnostic vigilance in similar clinical scenarios.
Recent radiologic reviews have highlighted that internal hernias should be considered in the differential diagnosis of bowel obstruction especially in patients without previous abdominal surgery, where adhesions are less likely to be the primary cause.4-7 Lanzetta et al emphasized that internal hernias, though rare, represent a potentially life-threatening condition and a diagnostic challenge precisely in this subgroup, because clinicians may be falsely reassured by the absence of prior operations and underestimate the likelihood of an internal aperture. 6 Doishita et al proposed a systematic CT-based approach to internal hernias that focuses on detecting a closed loop, identifying the hernia orifice, and analyzing displacement of surrounding structures and key vessels; their work reinforced the importance of detailed knowledge of peritoneal and mesenteric anatomy for accurate preoperative classification. 5 While precise categorization of the hernia type in our patient was difficult because the defect was formed by an isolated adhesive band rather than a classic peritoneal recess, the CT pattern of a focal whirl of mesenteric vessels and a short segment of compromised colon was nonetheless sufficient to raise strong suspicion of an internal hernia with strangulation.
Management of internal hernias hinges on prompt surgical exploration once signs of strangulation, ischemia, or closed-loop obstruction are present.3-7 Nonoperative treatment, which may be appropriate for partial adhesive small bowel obstruction without signs of ischemia, is generally not recommended in internal hernias because of the high risk of rapid deterioration. 7 The operative principles include reduction of the herniated bowel, assessment of viability, resection of any non-viable segments, and secure closure of the defect to prevent recurrence. Depending on patient stability, timing of presentation, and surgeon expertise, both laparoscopic and open approaches have been described.3-7 In hemodynamically stable patients diagnosed early, a laparoscopic approach can be considered and may allow minimally invasive reduction and repair. However, in elderly or unstable patients with suspected necrosis or perforation, open laparotomy remains the safest option, permitting rapid control, and extensive adhesiolysis when required. In our patient, advanced age, very high lactate, and necrotic colon justified an open approach with resection and creation of a protective double-barrel ileostomy, which was later reversed after recovery.
This case carries several practical lessons for clinical practice. First, internal hernia should remain in the differential diagnosis of bowel obstruction in patients without previous abdominal surgery, especially when CT demonstrates clustered loops, mesenteric crowding, or a whirl sign.4-6,9 Second, the presence of systemic signs such as leukocytosis and elevated lactate should heighten suspicion for strangulation and prompt urgent surgical referral. Third, advanced age and comorbidities should not delay operative intervention when imaging suggests a closed-loop process; instead, operative strategy can be individualized by favoring a temporary stoma rather than primary anastomosis to reduce postoperative risk. Finally, closure of the responsible mesenteric or peritoneal defect at the index procedure remains essential to prevent recurrence.
This report has several limitations inherent to its design. First, as a single case report, the findings cannot be generalized, and causal relationships between chronic constipation, increased intra-abdominal pressure, and the development of adhesive internal hernia in a virgin abdomen cannot be definitively established. Second, preoperative imaging was performed without intravenous contrast due to impaired renal function, which limited direct assessment of bowel wall enhancement and mesenteric perfusion; nevertheless, the diagnosis was supported by characteristic morphologic CT features and confirmed intraoperatively. Third, although the intraoperative findings were highly suggestive of an acquired idiopathic adhesive band, the exact temporal origin of the adhesion remains speculative, and a congenital component cannot be entirely excluded. Finally, the absence of long-term follow-up beyond successful stoma reversal limits assessment of late recurrence; however, closure of the mesenteric defect at the index operation reduces this risk. Despite these limitations, the case provides valuable clinical and radiologic insights into a rare but potentially life-threatening cause of intestinal obstruction.
Conclusion
Adhesive internal hernia in a virgin abdomen is an exceptionally rare but important cause of acute intestinal obstruction. This case of a 92-year-old man with strangulated colonic internal hernia illustrates how careful clinical assessment combined with CT findings, particularly the mesenteric whirl sign, can facilitate early recognition of a closed-loop process even in the absence of intravenous contrast and prior surgery. Prompt surgical exploration with resection of necrotic bowel, closure of the internal defect, and judicious use of a protective stoma led to an excellent outcome in a high-risk elderly patient. Clinicians should maintain a high index of suspicion for internal hernia in elderly patients with acute abdomen and a virgin abdomen, and radiologists should systematically search for subtle CT signs of internal herniation, as early diagnosis and timely operative management are crucial to prevent ischemia, perforation, and death.
Footnotes
Acknowledgements
The authors would like to thank the medical and nursing teams involved in the perioperative care of the patient. Their dedication and clinical expertise contributed significantly to the successful management of this case.
Ethical Considerations
Ethical approval was not required for this single-patient case report, as per the policies of our institution and the standard requirements for descriptive case reports without identifiable data.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case and any accompanying images.
Author Contributions
HF conceptualization, methodology, validation, writing – original draft, writing – review and editing. RN methodology, validation, writing – original draft, writing – review and editing. GK methodology, validation, writing – original draft, investigation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during the preparation of this case report are included within the article. No additional datasets were generated or used.