
Abstract
Introduction and Significance:
Hydatid disease, primarily caused by the parasite Echinococcus granulosus, commonly affects the liver and lungs. However, it can also involve other organs, including the pancreas. Pancreatic hydatid cysts are rare, constituting less than 2% of all hydatid cases. Their infrequent occurrence and atypical presentation often pose diagnostic and therapeutic challenges, especially in non-endemic regions.
Case Presentation:
A 42-year-old man with a cystic lesion in his pancreatic tail who had no notable medical history was seen. The diagnosis of a pancreatic hydatid cyst was validated by serological testing and diagnostic imaging techniques.
Clinical Discussion:
Due to their uncommon nature, the differential diagnosis of pancreatic hydatid cysts can be challenging. Imaging modalities such as computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound are important for identifying characteristic features. Serological testing further aids in confirming the diagnosis. Treatment typically involves a combination of medical and surgical approaches. Antiparasitic drugs, such as albendazole or mebendazole, are administered to kill the parasite. Surgical intervention is necessary to remove the cyst and reduce the chance of recurrence and complications.
Conclusion:
This instance highlights the significance it is to take hydatid disease into consideration when making a differential diagnosis for pancreatic cystic lesions, particularly in people from endemic regions. For the optimal possible patient outcomes and avoiding of complications, early diagnosis and effective treatment are important.
Introduction
Hydatid cysts, primarily instigated by Echinococcus granulosus, represent a form of parasitic infection that predominantly affects the liver and lungs, though they can occasionally manifest in other organs, including the pancreas. The life cycle of Echinococcus granulosus involves canines—such as dogs, foxes, and wolves—as definitive hosts. These animals harbor adult parasites in their intestines, releasing eggs into the environment through their feces. Human infection typically occurs via accidental ingestion of these eggs from contaminated soil, water, or food, often linked to direct contact with infected dogs or exposure to their fecal matter.1,2 The occurrence of pancreatic hydatid cysts is notably rare, comprising less than 2% of all hydatid cyst cases, and presents distinct challenges in both diagnosis and management.2,3 These cysts arise when hydatid larvae become encapsulated within pancreatic tissue, resulting in the formation of fluid-filled cystic lesions encased in a fibrous capsule. 3 The incidence of hydatid disease exhibits significant geographical variation, with heightened prevalence observed in areas where the parasite is endemic, such as certain regions of the Mediterranean, the Middle East, and South America. 4 Within these endemic zones, the incidence of pancreatic hydatid cysts can be considerable, particularly among individuals with a history of contact with livestock or consumption of contaminated food. 5 Diagnosing pancreatic hydatid cysts poses a challenge due to their atypical presentation and potential overlap with other pancreatic cystic lesions. Imaging modalities such as ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) play a critical role in distinguishing hydatid cysts from other pancreatic conditions. Radiological assessments typically reveal well-defined cystic lesions characterized by features such as internal septations or daughter cysts.7,8 Serological evaluations and enzyme-linked immunosorbent assays (ELISA) further aid in confirming the diagnosis. 9 The management of pancreatic hydatid cysts generally necessitates a multifaceted approach that combines pharmacological treatment with surgical intervention. Antiparasitic agents such as albendazole or mebendazole are frequently employed to combat the infection, while surgical procedures may be indicated to excise the cyst and mitigate the risk of recurrence or complications.10,11 Novel surgical techniques, including cryosurgery (which induces cyst necrosis via extreme cold) and PAIR (Puncture, Aspiration, Injection, Re-aspiration)—a minimally invasive approach involving cyst puncture, aspiration, and scolicidal agent injection—have shown promise in select cases.9,10 Treatment plans should be customized for the patient’s general health state as well as the size and location of the cyst. This case study details a 42-year-old man who, although having no notable medical history, arrived at an academic hospital with a cystic lesion in his pancreatic tail. The diagnosis of a hydatid cyst was confirmed by imaging investigations.
Case Presentation
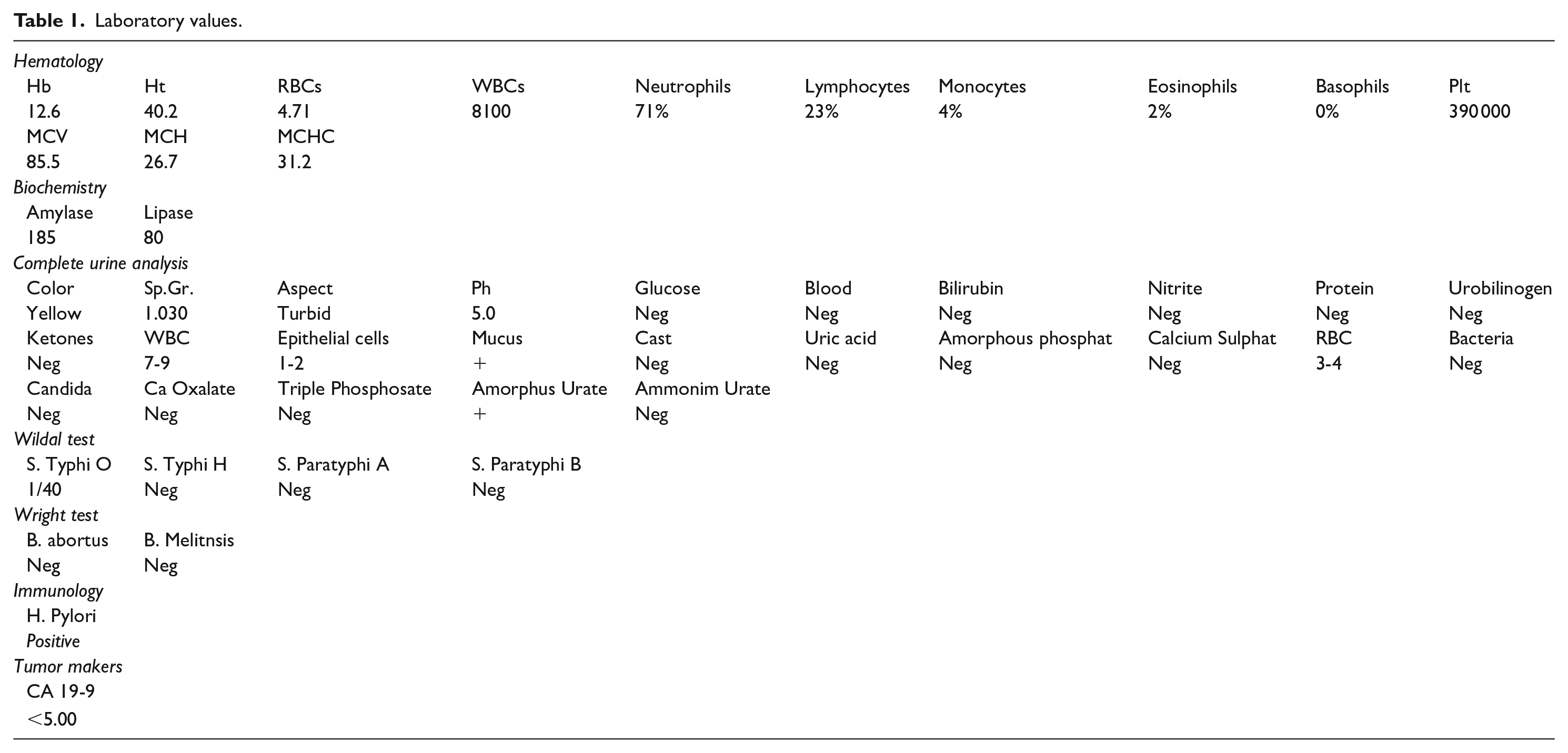
A 42-year-old man who does not smoke and comes from a rural area where dogs and livestock are frequent was brought to the emergency room by a family member who had been having mild epigastric pain for a 4-month. He had no significant medical, surgical, or familial history. Despite treatment for peptic ulcer disease, his symptoms progressed to early satiety and dyspepsia, without fever or vomiting. On physical examination, the abdomen was soft and tender, with mild tenderness in the epigastrium and left upper quadrant. Laboratory investigations demonstrated H. pylori positivity and elevated amylase levels (twice the normal value), indicating pancreatic involvement. A serological test performed at the time of diagnosis was positive, aligning with a suspected parasitic infection. Other laboratory parameters were within normal limits. (Table 1). Imaging tests, such as a CT scan and ultrasound, revealed multiple cystic lesions. A pancreatic hydatid cyst, approximately 6 × 6 × 8 cm, was located above the left kidney (Figure 1). Additionally, several lung cysts were identified, including 1 in the left lung apex measuring approximately 2 cm in diameter (Figure 2). Laboratory studies included a CA19-9 to exclude malignancy, which was normal, as well as Widal and Wright tests, both negative. Due to cost constraints, confirmatory ELISA testing was not performed, though the clinical and imaging findings strongly supported the diagnosis. Given the patient’s rural residence (high-risk exposure to Echinococcus granulosus), clinical presentation, and imaging findings, the differential diagnosis included pancreatic pseudocyst, pancreatic neoplasm, and pancreatic hydatid cyst. The combination of elevated amylase levels, lung cysts, positive serology, and imaging confirmed echinococcosis with pancreatic involvement. Surgical intervention was performed to excise the cysts and prevent dissemination. A laparotomy drained the pancreatic hydatid cyst, while lung cysts were removed minimally invasively (Figure 3). Postoperatively, the patient was initiated on Albendazole 400 mg daily for 3 months, after which the treatment was discontinued. The patient recovered well and was discharged in stable condition. Following surgery, we monitored the patient both clinically and radiologically for approximately 6 months, during which time he showed no signs of complications or recurrence.
Laboratory values.

CT scan and Echo demonstrating a 6 cm × 6 cm × 8 cm cyst with thick walls and homogenous fluid content has formed at the level of the tail of the pancreas and superior to the left kidney.

An X-ray shows signs of chronic bronchitis, along with fluid-filled cysts in the left lung field. The largest cyst is located in the left lung apex, measuring approximately 2 cm, with a homogeneous fluid content and well-defined borders.

Surgical procedure involved aspiration, incision, and drainage of the cyst, followed by removal of the proliferating membrane.
Discussion
PHCs are exceedingly rare, accounting for 0.14% to 2% of hydatid disease. 12 The parasite Echinococcus granulosus typically reaches the pancreas through the bloodstream after passing through the liver and lungs. 12 While hematogenous spread is most common, lymphatic or direct intestinal routes are also possible. 13 PHCs are predominantly solitary, with a predilection for the pancreatic head due to its richer blood supply. 14 However, our case presented an uncommon location - the pancreatic tail. Cyst size can range from millimeters to centimeters, residing either within (35%) or adjacent to (65%) of the pancreatic tissue.6-13 PHCs are often asymptomatic, with clinical manifestations depending on cyst size, location, and complications. Symptomatic PHCs typically present with upper abdominal pain, vomiting, and a palpable mass. 13 Pancreatic head cysts can cause obstructive jaundice by compressing the common bile duct, 12 while body or tail cysts may remain asymptomatic until an abdominal mass is discovered. 14 Notably, our patient’s only symptom was consistent epigastric pain, likely due to the cyst’s size (5 × 8 cm). Potential complications include cholangitis, pancreatitis, pancreatic abscess, and pancreatic fistula. 13 Additionally, body or tail cysts might cause splenomegaly, portal hypertension, or rupture into the peritoneal cavity or gastrointestinal tract. 14 Clinical examination is often the initial diagnostic step for primary hydatid cysts, but the clinical picture can be non-specific and variable, depending on the cyst’s characteristics. In many cases, the infection is asymptomatic. Our patient’s main symptoms and signs were weakness, epigastric pain, and left upper quadrant tenderness. Due to their rarity, PHCs are frequently misdiagnosed as other cyst types like pancreatic cystadenoma, cystadenocarcinoma, or pancreatic pseudocyst. 12 Accurate diagnosis of PHCs typically relies on imaging techniques. Methods like MRI, CT, and ultrasound are commonly used to visualize cysts, and assess their size, location, and relationship to adjacent structures. 15 In our case, ultrasound revealed the cystic formation in the pancreatic tail. While serum anti-echinococcal IgG antibodies can be supportive, a significant number of case reports suggest they might be negative in hydatid cyst infections. 16 Surgical excision is generally the preferred treatment approach for PHCs. Surgical treatment is recommended for symptomatic hydatid disease, as well as patients with active or complicated hydatid disease. 16 The surgical therapy of pancreatic hydatid cysts (PHCs) requires an effective plan that considers the cyst’s location, size, and complications. 17 Techniques used in surgery include: Drainage of the cyst: This method works well for superficial cysts, but if albendazole, an antiparasitic medication, is not taken, there is a chance of recurrence. 18 Whipple’s pancreaticoduodenectomy, distal pancreatectomy, or partial pericystectomy: in cases when the cyst connects with the main pancreatic duct, this approach is appropriate if the cyst is deep and buried in the pancreatic duct, but if the surgeon is not skillful and experienced, there is a chance that the patient may develop a pancreatic insufficiency.16,17 Robotic or laparoscopic surgery: For peripheral cysts, this non-invasive technique is becoming more and more popular.17,18 This decreases infection and recurrence rates while also speeding up healing, It is also used to treat lung cysts, where video-assisted thoracoscopic surgery (VATS) is the optimal surgical strategy, 13 in keeping with current studies and trends favoring non-invasive and minimally invasive procedures for Extrapancreatic hydatid cyst therapy.19,20 In our situation, surgical excision was the preferred therapy method. This case report provides valuable insights into the diagnosis and management of pancreatic hydatid cysts. However, the retrospective nature of the study and the small sample size limits the generalizability of the findings. Further research is needed to explore the optimal management strategies for PHCs, particularly in different clinical settings. While surgical intervention remains the mainstay of treatment, as demonstrated in this case, ongoing efforts to develop less invasive techniques and improve post-operative outcomes should be prioritized. Future studies could investigate into long-lasting consequences of PHC patients, including the risk of recurrence and potential complications. In our instance, it emphasizes how crucial it is to take hydatid disease into account when making a differential diagnosis for pancreatic cystic lesions, particularly in areas where it is endemic. For optimal outcomes for patients, early diagnosis and appropriate surgical intervention are essential.
Conclusion
This case exemplifies the rarity and diagnostic complexities associated with PHCs. While uncommon, they have to be included in the differential diagnosis in patients who have pancreatic cysts, especially in areas that are not endemic. A precise diagnosis necessitates a combined approach utilizing imaging techniques and serological assays to distinguish hydatid cysts from other pancreatic disorders. Effective management strategies encompass a dual-modality of antiparasitic treatment and surgical intervention to avert complications and minimize the risk of recurrence. This case underscores the critical need for comprehensive evaluations for parasitic infections in patients who have pancreatic cysts, especially those with pertinent epidemiological histories.
Footnotes
Acknowledgements
We hope to thank SMSR Team Lab. for their efforts and for bringing our team together.
Ethical Considerations
Ethics approval is not required for case reports deemed not to constitute research at our institution
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author Contribution
S.M. wrote a part of the manuscript.
S. Z. wrote a part of the manuscript.
M. L. wrote a part of the manuscript.
M. A. wrote a part of the manuscript.
A. A. wrote a part of the manuscript.
M. S. wrote a part of the manuscript.
A. ALW. wrote a part of the manuscript.
All authors approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Research Registration Number
Not applicable because our article is a case report.
Guarantor
Mais Alreem Mohaisen
Methods
The work has been reported in line with the SCAR criteria.