
Abstract
Introduction:
Allergic contact dermatitis (ACD) is a rare but clinically significant hypersensitivity reaction to certain medications, including enoxaparin, a commonly used low-molecular-weight heparin (LMWH) for venous thromboembolism (VTE) prophylaxis.
Case Presentation:
We report the case of a 27-year-old woman who developed pruritic, erythematous eruptions localized to enoxaparin injection sites following sleeve gastrectomy. Symptoms emerged 6 days after initiating enoxaparin and were confirmed as ACD via clinical assessment and histopathological analysis, which revealed spongiotic dermatitis with eosinophilic infiltration. The patient responded well to topical mometasone ointment, with complete resolution of symptoms within 4 weeks.
Conclusion:
This case underscores the importance of recognizing enoxaparin-induced ACD and emphasizes the role of histopathology and individualized treatment strategies in optimizing patient care.
Keywords
Introduction
Allergic contact dermatitis (ACD) is a delayed-type hypersensitivity reaction that develops upon skin contact with specific allergens, leading to localized inflammation. This inflammatory response is mediated by T-cells that recognize the allergen as foreign, resulting in erythema, itching and vesiculation at the contact site. 1 Though ACD is commonly triggered by allergens such as metals, preservatives, and fragrances, certain medications can also provoke these responses. Among these, injectable medications like enoxaparin, a low-molecular-weight heparin (LMWH) used widely for its anticoagulant properties, have occasionally been associated with localized allergic skin reactions.2 -4 Enoxaparin is frequently prescribed to prevent venous thromboembolism (VTE) in high-risk patients, especially post-operatively. 2 However, adverse reactions such as ACD remain underrecognized due to their rarity and the often-mild nature of symptoms, which may go undiagnosed.
While ACD is generally common, cases specifically involving enoxaparin are rarely documented. A 2023 case report of Saraiva et al, identified a limited number of reported instances of ACD triggered by these agents, with systemic hypersensitivity reactions like urticaria, angioedema, and anaphylaxis more commonly reported. 3 The nonspecific and subtle nature of localized allergic reactions can lead to misdiagnosis, often as a simple irritant contact dermatitis rather than a true allergic response. The actual frequency of ACD due to enoxaparin injections may thus be underestimated in clinical practice. 4
The limited literature on enoxaparin-related ACD cases suggests that these reactions may manifest days to weeks after the initiation of therapy, typically confined to the injection sites. 5 Enoxaparin itself contains additional compounds, such as preservatives and stabilizers, that can contribute to sensitization in some patients. 6 However, recent research focuses on severe hypersensitivity reactions to LMWHs, and data on ACD specifically is sparse. Few studies explored the underlying mechanisms that could make certain patients more susceptible to developing ACD upon enoxaparin exposure. As a result, there remains a need for thorough documentation of these cases, which could improve understanding of risk factors, symptoms, and management options. 7
Current gaps in knowledge about ACD related to LMWHs are significant, as reactions of this type can interfere with patient adherence to necessary anticoagulant therapy. 8 Patch testing plays a role in diagnosing allergic contact dermatitis but has limited applicability in routine clinical practice for LMWH-related reactions, often requiring alternative methods like intradermal or provocation testing for accurate diagnosis. 9 As a result, cases like these may not only remain undetected but also untreated, with potential consequences for patient outcomes, especially when anticoagulant therapy is needed for extended periods. To address these issues, in this case report, we discuss a unique case of enoxaparin-induced ACD in a young woman with a history of polycystic ovarian syndrome (PCOS) and hidradenitis suppurativa, who was undergoing VTE prophylaxis following sleeve gastrectomy.
Case Presentation
This is a case of a 27-year-old Saudi woman with a history of PCOS and hidradenitis suppurativa, who recently underwent sleeve gastrectomy and was on a 21-day prophylactic enoxaparin 40 mg/day subcutaneous injection for venous thromboembolism. She presented to our dermatology outpatient clinic with a 1-month history of itchy skin lesions on her lower thighs and left upper shoulder, corresponding to the sites of enoxaparin injections. These skin lesions developed on the sixth-day after starting enoxaparin therapy. Her medication history included doxycycline 100 mg/day, which was discontinued post-surgery. Skin examination revealed localized ill-defined erythematous edematous plaques with fine scales on bilateral lower thighs (Figure 1A) and the left upper shoulder (Figure 1B). A 4 mm skin punch biopsy for hematoxylin and eosin (H&E) staining to further evaluate the skin lesions and revealed spongiotic dermatitis with eosinophils (Figures 2 and 3). Considering the clinical findings in addition to the histopathology results, a diagnosis of allergic contact dermatitis was established. The patient was informed about the nature of the skin allergy and was advised to discontinue enoxaparin, with arrangements for an alternative to be made by her primary team if needed. She was prescribed topical mometasone ointment twice daily for 2 weeks. On 4-weeks follow-up, the patient had no active lesions.
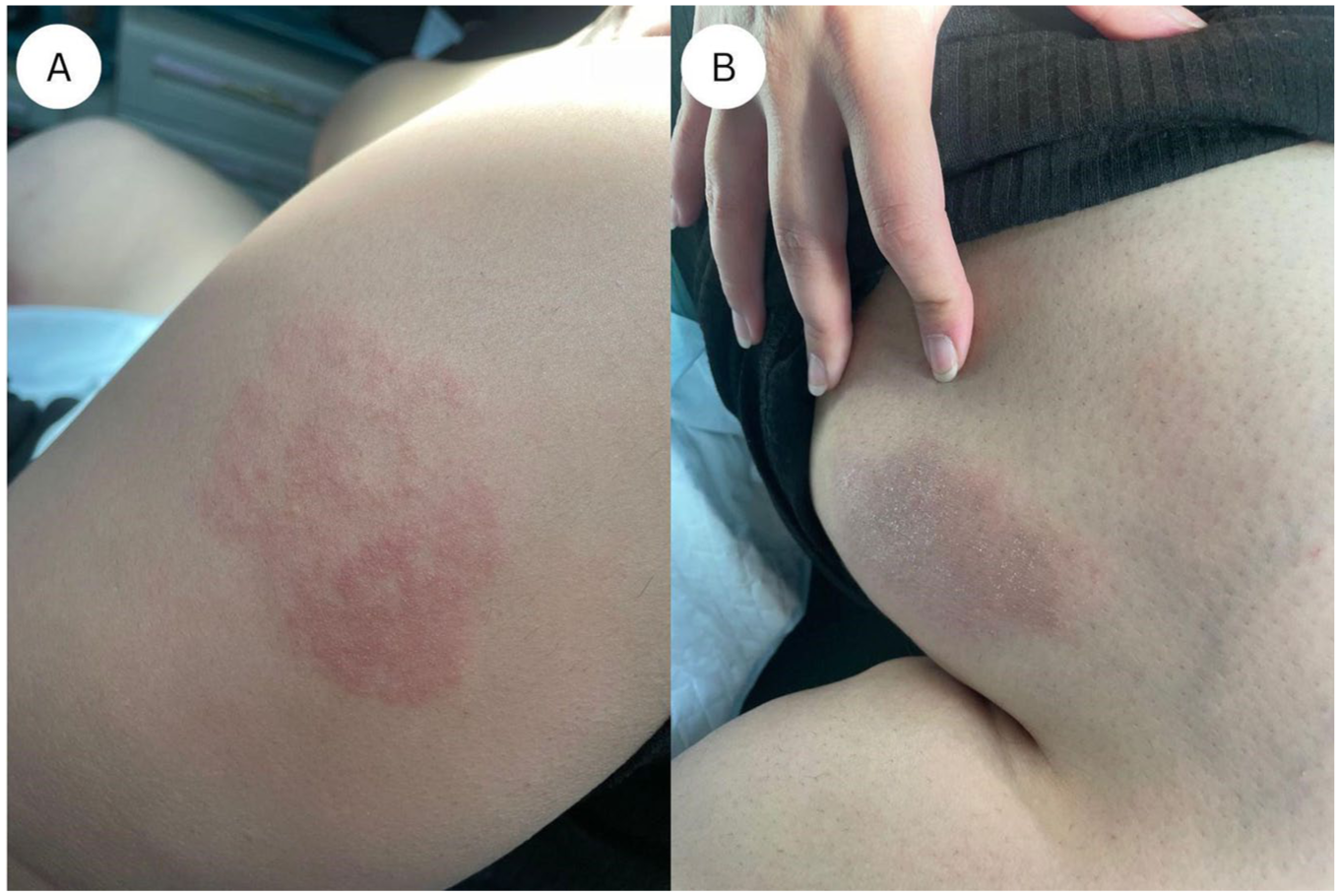
Localized ill-defined erythematous edematous plaques with fine scales over the (A) shoulder and (B) thigh.

Photomicrograph of the skin punch biopsy exhibits parakeratosis, acanthosis and mild spongiosis (H/E stain, original magnification × 40).
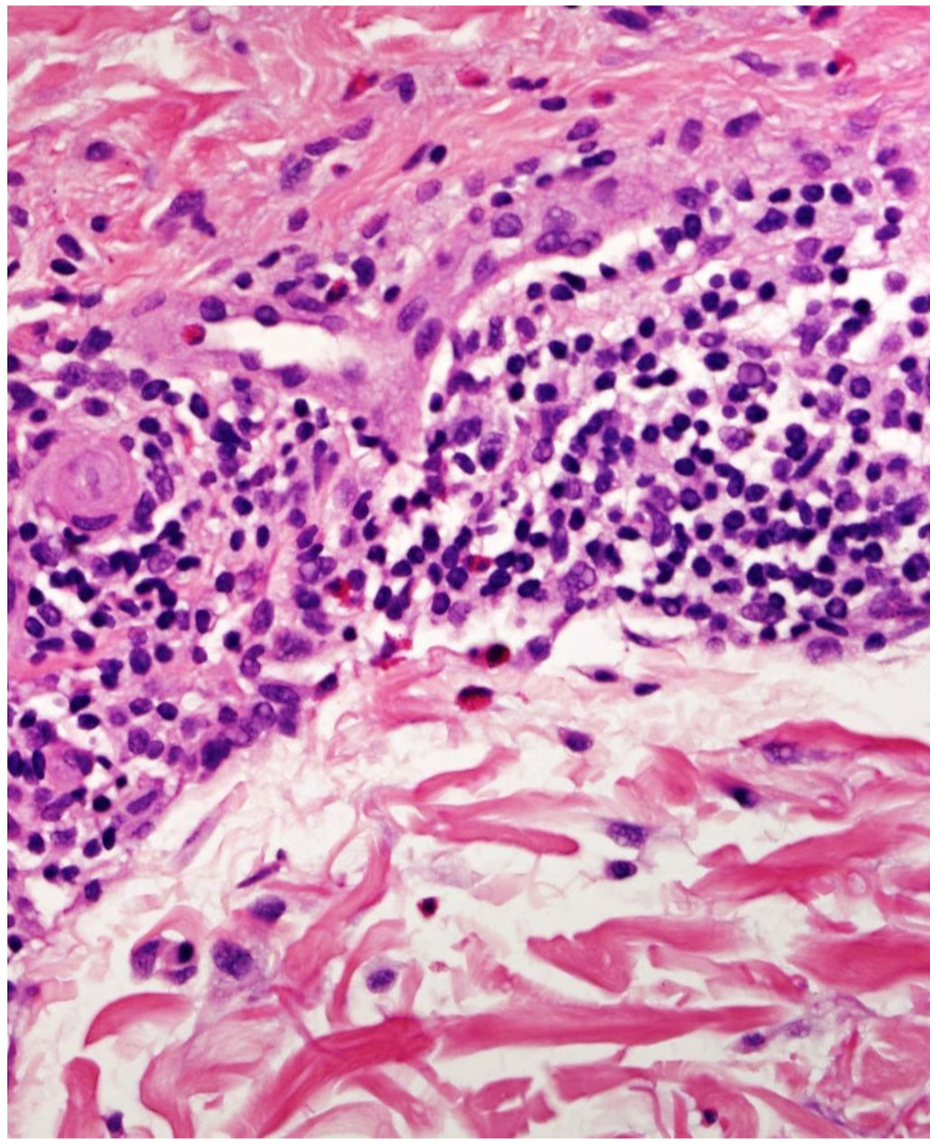
High power view reveals superficial perivascular lymphocytes and scattered eosinophils (H/E stain, original magnification ×400).
Following the resolution of lesions, patch testing was conducted, which showed sensitivity to nickel. No reaction to enoxaparin was detected on patch testing.
Discussion
Allergic contact dermatitis (ACD) resulting from subcutaneous enoxaparin injections is an uncommon yet clinically significant condition that requires recognition, particularly in patients requiring long-term anticoagulation therapy. This case report describes a 27-year-old woman who developed pruritic, erythematous skin lesions localized to the injection sites after initiating enoxaparin for venous thromboembolism (VTE) prophylaxis. These findings contribute to the limited number of documented cases of enoxaparin-induced ACD, underscoring the need for increased awareness among healthcare providers about this rare but important adverse reaction.
The prevalence of hypersensitivity reactions to LMWHs varies across patient populations. One study reported rates of 1.9% in orthopedic patients, 7.5% in medical patients, and 19.8% in obstetric patients, indicating a higher risk in certain groups. 10 Additionally, hypersensitivity reactions to LMWHs are often underreported, with most cases focusing on systemic rather than localized reactions. 11 This case emphasizes the importance of identifying localized reactions, as the dermatitis in our patient was confined to injection sites and lacked systemic involvement, supporting a diagnosis of ACD.
Histopathological examination in this patient revealed spongiotic dermatitis with perivascular lymphocytic infiltration and eosinophils, a hallmark feature of LMWH-induced ACD. 12 The presence of eosinophils in spongiotic dermatitis has been suggested as a characteristic finding in LMWH-related ACD, distinguishing it from irritant contact dermatitis, which lacks immune-mediated changes.12,13 This highlights the diagnostic value of histopathology in confirming ACD cases when clinical presentation is unclear.
Patch testing, commonly used to identify allergens in ACD, demonstrated limited utility in this case. While nickel was identified as a potential allergen, patch testing failed to confirm sensitivity to enoxaparin, a limitation consistent with earlier reports. 8 Negative patch test results are not uncommon in delayed-type hypersensitivity (DTH) to LMWHs, likely due to the test’s inability to fully replicate in vivo conditions. In such cases, intracutaneous testing or controlled challenge tests may provide greater diagnostic sensitivity and should be considered when clinical suspicion remains high. 8
Management of enoxaparin-induced ACD in this case was achieved using mometasone alone, with resolution of symptoms within 4 weeks. These findings align with previous reports recommending topical corticosteroids to alleviate symptoms and prevent progression. 14 However, recurrent or severe reactions may warrant transitioning to alternative anticoagulants. According to Kavut and Koca, patients with LMWH hypersensitivity may benefit from unfractionated heparin (UFH) or other anticoagulants, though these alternatives carry variable risks and require careful clinical management. 15 LMWHs are distinguished from Unfractionated Heparins (UFHs) by their molecular weight, which ranges from 4 to 6 kiloDaltons (kD), compared to 10 to 20 kD for UFHs. 16
Delayed-type hypersensitivity reactions often exhibit cross-reactivity among LMWHs, UFH, danaparoid, and fondaparinux, complicating the selection of alternative anticoagulants. Hirudins, which have a distinct chemical structure, are less likely to demonstrate cross-reactivity and represent a safer option. 17 Transitioning to a hirudin or fondaparinux can serve as an effective interim solution while awaiting the results of further allergological testing 17 (see Table 1).
Summary of Reported Cases of Delayed-Type Hypersensitivity Reactions to Enoxaparin.

This case contributes to the limited but expanding body of literature on enoxaparin-induced allergic contact dermatitis (ACD). It underscores the importance of considering ACD in the differential diagnosis when patients present with localized eczematous eruptions at injection sites. Early recognition and appropriate management are critical, particularly in the context of the widespread use of low-molecular-weight heparins (LMWHs) in anticoagulation therapy.
In this case, patch testing was performed and yielded a negative result for enoxaparin. The patient did test positive for nickel sensitivity; however, this finding was considered clinically irrelevant due to the absence of any known exposure or correlation with the affected injection sites. It is important to recognize that negative patch tests do not definitively exclude the diagnosis of ACD, particularly with LMWHs such as enoxaparin. Also, the epicutaneous patch testing may have limited sensitivity in detecting LMWH-related hypersensitivity reactions.22,23
Although the clinical features, temporal correlation with drug administration, and histopathological findings (notably spongiotic dermatitis with eosinophils) were suggestive of ACD, the lack of more specific confirmatory testing, such as intradermal testing or site-specific patch testing over previously affected areas, represents a significant limitation. Moreover, the histopathological findings, while supportive of a hypersensitivity reaction, are not pathognomonic and can be seen in a range of inflammatory dermatoses. Given these limitations, the diagnosis of ACD in this case remains plausible but not definitive. Nonetheless, documenting such presentations, even when diagnostic certainty is limited, can help raise awareness of rare cutaneous adverse reactions to enoxaparin and encourage more comprehensive diagnostic evaluation in future cases.
Conclusion
Enoxaparin-induced ACD, while rare, is an important adverse effect that clinicians should consider in patients presenting with localized skin reactions at injection sites. Histopathological analysis and appropriate diagnostic testing are essential to confirm the diagnosis and identify the causative agent. Early recognition and management, including the use of alternative anticoagulants when necessary, can prevent complications and improve patient outcomes. This case highlights the need for increased awareness and reporting of such reactions to enhance understanding and guide future management strategies.
Footnotes
Abbreviations
ACD: Allergic Contact Dermatitis; LMWH: Low-Molecular-Weight Heparin; VTE: Venous Thromboembolism; PCOS: Polycystic Ovarian Syndrome; H&E: Hematoxylin and Eosin; UFH: Unfractionated Heparin; nDTH: Delayed-Type Hypersensitivity.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
The patient gave her consent for the publication of this case report.
Consent for Publication
Written Informed Consent was obtained from the legal guardian of the patient for the publication of this case report.
Author Contributions
Hend M. Alotaibi and Alhanoof Alajlan: Conception of the case report, clinical assessment, and data acquisition. Abdulrahman Alluhaybi: Literature review and manuscript drafting. Ahmed A. Alhumidi: Histopathological evaluation, image interpretation, and critical revision. All authors have read and approved the manuscript. Furthermore, all ICMJE requirements for authorship have been met, and this work represents an original and honest work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.