
Abstract
Background:
A gastric fistula (GF) is defined as an abnormal communication between the gastric mucosa and an adjacent anatomical structure.
Case Presentation:
We report a 30-year-old male patient who developed a subcardial gastric fistula after sleeve gastrectomy. It was successfully treated using the Over-the-Scope Clip (OTSC) system as a non-surgical approach.
Conclusion:
This case demonstrates the effectiveness and feasibility of the over-the-scope clip device for closure of post-bariatric gastric fistulas and highlights its applicability when surgical intervention carries significant risks.
Introduction
A gastric fistula (GF) is defined as a pathological tract that establishes communication between the epithelialized mucosa of the stomach and another anatomical structure. In adults, GF most frequently develops in the setting of malignant gastric disease; however, it may also occur as a postoperative complication—particularly after bariatric procedures—or arise secondary to trauma, infection, or chronic inflammatory processes. 1 The incidence of gastric fistulas after Roux-en-Y gastric bypass is reported between 1% and 6%. 2
The clinical manifestations of gastric fistula vary according to its etiology and location. Common symptoms include nausea, vomiting, fever, and epigastric pain; this condition may also be associated with marginal ulcers.3,4
Gastric fistulas are generally classified as internal (abnormal communication between the GI tract and an internal space) and external (connection between the GI tract and the skin surface). 5 They may also be classified by etiology, anatomy, and output volume: low-output (<500 mL/day) or high-output (>500 mL/day). 6
Understanding the etiology, anatomical characteristics, and location of a gastric fistula is essential, as these factors significantly influence the likelihood of successful endoscopic closure. While high-output fistulas are readily identified through imaging studies, the decision to pursue endoscopic therapy is not determined solely by output volume. 7 Endoscopic closure of gastric fistulas has been investigated for more than a decade, with the over-the-scope clip (OTSC) system demonstrating promising outcomes, achieving an initial closure rate of 81.1%. 8
The over-the-scope clip (OTSC) system is a hemostatic endoscopic device that was initially introduced for the management of non-variceal gastrointestinal bleeding. Made of elastic nitinol, it achieves complete closure by approximating tissue and was FDA-approved in 2010. Unlike standard through-the-scope (TTS) clips, OTSC can close defects larger than 2 cm in a single application.9,10
Herein, we present our clinical experience using OTSC to close a gastric fistula following bariatric surgery.
Case Presentation
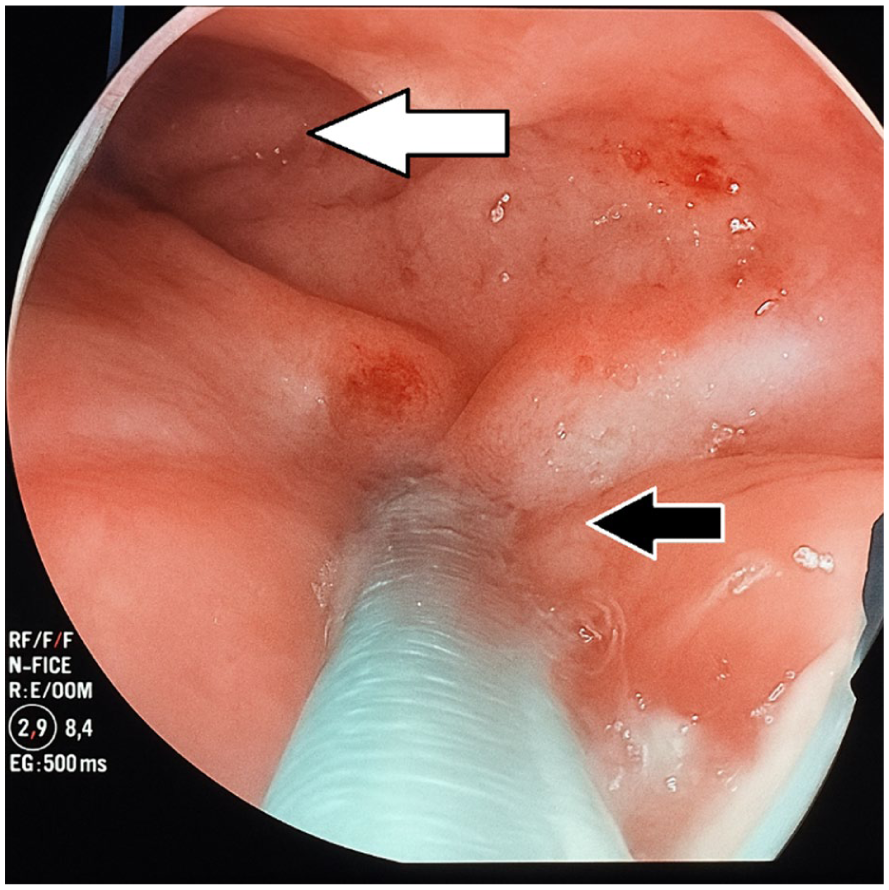
A 30-year-old male presented with a 1-week history of abdominal pain, fever, and intolerance to oral intake. His medical history was notable for obesity and hypertension, and he had undergone a sleeve gastrectomy 7 days earlier. On examination, he was tachycardic and tachypneic, with localized tenderness in the epigastrium and left hypochondrium. Initial laboratory tests revealed leukocytosis with a left shift and elevated acute-phase reactants. Computed tomography (CT) imaging demonstrated a small left pleural effusion and a subphrenic abscess. Upper endoscopy revealed a 1 cm posteromedial mucosal defect in the subcardial region, located 5 cm distal to the gastroesophageal junction, consistent with a gastric fistula. (Figure 1).

Endoscopic view of the sub-cardial region with sub-cardial fistula (black arrow), above the gastroesophageal junction (white arrow).
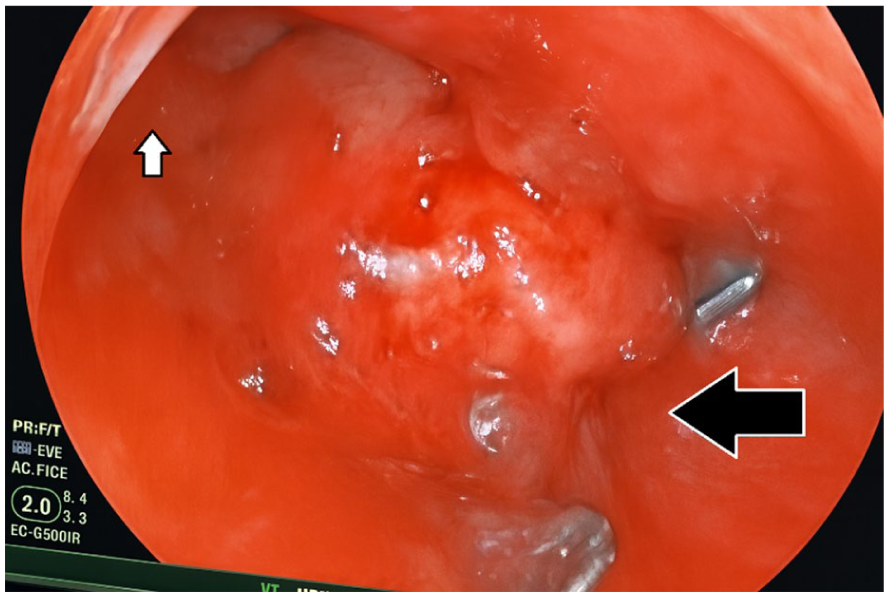
Initial non-operatory management, including nil per os, antibiotics, and parenteral nutrition, was unsuccessful. The patient subsequently underwent endoscopic placement of an over-the-scope clip (OTSC) using a Fujinon 250 gastroscope equipped with a pre-mounted device. (Figure 2 ). At 48 hours, endoscopy confirmed correct clip placement and complete closure of the fistula. (Figure 3). No leakage or complications were observed. The patient recovered and was discharged with favorable outpatient follow-up.
Endoscopic view of sub-cardial fistula with OTSC device (black arrow), above the gastroesophageal junction (white arrow).
Endoscopic view of sub-cardial fistula closed with OTSC Clip, above the gastroesophageal junction (white arrow).
Discussion
This case describes the successful management of a subcardial gastric fistula following sleeve gastrectomy using the OTSC system, demonstrating its role as a non-surgical alternative. Gastric fistulas after sleeve gastrectomy occur in 0.5% to 6% of cases and are often accompanied by abscess or pleural effusion.1-3
Endoscopic OTSC closure offers a less invasive option, potentially reducing reoperation rates and improving outcomes. 3 Compared to expandable stents, which have migration rates up to 47% and ulceration rates of 41% OTSC shows fewer complications.1,2
Mosquera-Klinger et al. reported a technical success rate of 100% and a clinical success rate of 78.6% in gastrointestinal perforations treated with OTSC in a tertiary center. 1 In Bogotá, a 2015 case series reported an 83.3% success rate in various GI lesions, including post-bariatric gastric fistulas. 9
These outcomes align with our findings. Factors such as early detection and timely intervention significantly enhance success rates. However, further large-scale studies are needed to evaluate long-term results, cost-efficiency, and help create evidence-based guidelines for OTSC use in this context.
Conclusion
The over-the-scope clip represents a safe and effective minimally invasive alternative to surgical re-intervention in post-bariatric gastric fistulas. However, broader studies are needed to establish its role as a first-line therapeutic option.
Footnotes
ORCID iDs
Consent for Publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Author Contributions
All authors created the initial manuscript draft, performed the relevant literature review, and edited the revisions and final draft. H.J.G.A. and I.J.R.A. made revisions while creating the drafts. All authors participated in the writing of the manuscript. All authors contributed enough to claim authorship of the manuscript and approved the final version of it.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.