
Abstract
Background:
This report presents a unique case of subacute BCS in a patient with systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), and multiple inherited thrombophilic disorders No previous history and lack of inciting events meant extensive investigation had to be done to figure out the underlying pathology. The amalgam of thrombophilias presenting initially as Sub-Acute Budd Chiari syndrome is very rare to find in the literature and highlights the importance of early screening and diagnosis to prevent complications of Thrombosis.
Case Presentation:
The patient presented with a 3 months history of progressive abdominal distension, hematemesis, and altered consciousness. The diagnosis made was Sub-Acute Budd Chiari Syndrome. The patient was managed with anticoagulation, diuretics, and symptomatic treatment. After stabilization the patient was discharged for follow-up after 2 weeks.
Conclusion and Key Take-Away Lessons:
This case highlights the diagnostic challenges of BCS, particularly in patients with hereditary hypercoagulability. Early recognition and management are critical in preventing severe complications of thrombosis. Moreover, it underscores the impact of limited healthcare access in rural settings, emphasizing the need for improved screening, awareness, and targeted interventions for thrombophilic disorders with a set diagnostic criteria for sub-acute presentation.
Introduction
Budd-Chiari syndrome (BCS) is a rare disorder characterized by hepatic venous outflow obstruction anywhere from the hepatic venules to the junction of the inferior vena cava (IVC) to the right atrium. It occurs in .001% or 1/100 000 of the population worldwide. 1 Data specific to Pakistan is scarce, however, large-scale studies depict that the number of cases with BCS is larger in Asia than in the West, highlighting potential regional differences in disease prevalence and awareness. 2 Systemic lupus erythematosus (SLE) is an autoimmune disease in which the pathogenesis is via numerous self-reacting antibodies or autoantibodies in serum. Concurrent presentation with Anti-Phospholipid Syndrome (APS) may occur in which the patient presents with recurrent episodes of thrombosis, thrombocytopenia, spontaneous miscarriages and, as in this case, Budd-Chiari Syndrome. 3 Here, we report a case of subacute Budd-Chiari syndrome as the initial presentation in the clinic for a patient with SLE and APS, along with a series of clotting factor abnormalities including antithrombin III deficiency, Factor V Leiden mutation and protein C deficiency. This case has been reported following the CARE criteria. 4
Case Presentation
A 35-year-old female from Dadu District with no known comorbidities presented to Civil Hospital Karachi Department of Medicine outpatient clinic with the complaint of abdominal distension for 3 months. The onset of the distention was insidious and progressively increasing. It was associated with abdominal pain, hematemesis, melena, and an altered level of consciousness. There was no fever, weight loss, generalized weakness, cough, or chest pain. History of tattooing, IV drug use, recent dental procedures, or blood transfusions was negative. She was not pregnant when she arrived and has 3 healthy kids all delivered via spontaneous vaginal delivery. She had a history of 1 miscarriage in the 2nd month of pregnancy 14 years prior due to an unknown cause.
On general physical examination, the patient appeared pale, poorly nourished and had pedal edema. She had a blood pressure of 121/72 mmHg, regular pulse, heart rate of 84 beats per minute, respiratory rate of 16 breaths/minute, and temperature of 98.6 F. Systemic examinations performed included an abdominal examination showing a distended abdomen, liver enlargement with a span of 20 cm in the midclavicular line extending up to the epigastric region with regular margins, smooth surface, and firm consistency. Shifting dullness and fluid thrill were appreciable, and gut sounds were audible and normoactive. Prominent veins, pulsations, tenderness, and masses were unremarkable. Based on history and examination, the patient was admitted to the general medicine ward with the differential diagnosis of decompensated chronic liver disease, infiltrative disorder, Budd-Chiari syndrome, connective tissue disorder, or abdominopelvic malignancy. Initial baseline markers and investigations carried out are contained in Table 1.
Initial Testing.

Further examination via ultrasound of abdomen and a Doppler ultrasound of IVC hepatic and portal veins revealed liver enlargement measuring 17.4 cm with altered echotexture, irregular margins, and gross abdominopelvic ascites. Doppler ultrasound revealed reverse flow in the hepatic vein while IVC and portal vein showed normal flow. Since the imaging investigations were highly suggestive of Budd-Chiari syndrome, contrast Computed Tomography (CT) scan of the chest, abdomen and pelvis was ordered to confirm the diagnosis Figure 1.

Axial sections of abdominal contrast-enhanced CT scans at different levels show thrombosis of the IVC (arrowhead in A), caudate lobe hypertrophy and inhomogeneous enhancement of liver parenchyma (white and black arrowheads in B, respectively), thrombosis of the hepatic veins (arrowhead in C) and a network of compensatory dilated veins presenting as anterior collaterals (arrowhead in D).
The CT scan showed the right lobe moderately enlarged measuring 24 cm with reduced parenchymal enhancement in arterial phase and heterogeneous patchy parenchymal enhancement in the venous phase giving a mottled appearance. The caudate lobe was also hypertrophied. A filling defect was seen in the right hepatic vein and distal tributaries suggesting hepatic venous thrombosis. Numerous small varices were seen in the esophageal wall, epigastrium, and splenic hilum. BCS can be caused by multiple pathologies including acquired thrombophilia, inherited thrombophilia, systemic factors, and hormonal factors 1 as displayed in Table 2. Therefore as part of further investigation, Thrombophilic and lupus profiles were sought, the findings of which are displayed in Table 3, showing positive Anti-Nuclear Antibody (ANA) and Anti Double Stranded DNA (Ds DNA) antibody with hypocomplementemia suggesting SLE. Thrombophilic profile showed abnormal levels of Protein C, Antithrombin III, Factor V Leiden (APC Resistance Ratio), Lupus Anticoagulant and Anticardiolipin IgG/IgM antibody, suggesting APS and Clotting factor deficiency. Paired with the massive ascites, these findings confirmed the diagnosis of subacute Budd-Chiari syndrome.
Causes of Budd Chiari Syndrome.

Thrombophilic and Lupus Profile.

Management and Outcome
The patient was initially started on enoxaparin accompanied by spironolactone 100 mg once daily and furosemide 40 mg once daily, titrated up with a 100:40 mg ratio, ceftriaxone, omeprazole and carvedilol 3.25 mg once daily. On the second day, warfarin 5 mg once daily was initiated along with enoxaparin injections daily and the Prothrombin Time/International Normalized Ratio (PT/INR) was monitored. On the third day, warfarin dose was reduced to 2.5 mg once daily because the PT/INR went up to 5. In the next 5 days her PT/INR dropped to 3 and warfarin was continued while enoxaparin was discontinued. On follow-up after 2 weeks, the abdominal distension showed minimal improvement so the dose of diuretics was increased from Once Daily to Twice Daily. On the next follow up 2 weeks later, the abdominal distention decreased significantly and her symptoms showed improvement. Warfarin dose was reduced to 1 mg Once Daily. No additional symptoms were reported. During her stay, the patient was offered Transhepatic Intrajugular Portosystemic shunt (TIPS) and a liver transplant. The transplant was refused due to financial constraints, and the TIPS could not be performed because the patient was initially unstable and later developed hepatic encephalopathy.
Outpatient Follow-Up
The patient was counselled on the need for regular monitoring of PT/INR due to warfarin use and its teratogenicity and its implications on future pregnancy plans. She was encouraged to report any new abdominal distention immediately to the nearest physician to avoid further exacerbations. Warfarin 1 mg once daily, omeprazole 20 mg once daily for GI protection and carvedilol 3.125 mg once daily for varices, with regular INR and abdominal imaging every 3 to 6 months was advised.
Literature Review
Comparative Analysis
The incidence of BCS varies from 0.2 to 4.1 per million inhabitants per year; prevalence is estimated to be between 2.4 and 7.7 per million for Asian countries and between 1.4 and 4.0 per million inhabitants in Western countries. 5 A female predilection was found in Western data ≈ 50% to 70% while a male predilection ≈ 50% to 70% was seen in Asian studies. 5 Median Age of diagnosis in the west and Europe was estimated to be late 40s to mid 50s while patients in Pakistan, Nepal and Egypt reported in their mid 20s. 5 An observational study which ran over 10 years in Pakistan reported median age of diagnosis to be 26 and with 58% males and 42% females. 6 This 10 year cohort with only 45 patients is the most detailed study available in the literature, highlighting the under representation of Pakistani clinical data and resultant guidelines such as “Asian Pacific Association for the study of the liver (APASL)” being extrapolated from East or Central Asian data. 7 Notably, in Western countries, myeloproliferative disorders constitute a major risk factor for primary BCS. In contrast, obstruction of the IVC is a greater risk factor in Asia, while myeloproliferative diseases are rare. 2
Clinical Presentations and Diagnostic Challenges
In acute BCS, hepatic necrosis and ascites develop rapidly within a few weeks, while venous collaterals are not yet apparent. Fulminant liver failure is a common sequela and is characterized by elevated liver enzymes, jaundice, coagulopathy and eventual hepatic encephalopathy. 8 In subacute BCS, it usually takes up to 3 months for clinical symptoms to appear. Ascites and hepatic necrosis are minimal due to the development of venous collaterals. Patients with chronic BCS will present with cirrhosis related complications and venous collaterals. 8 Obstruction of the hepatic veins in Budd-Chiari syndrome leads to sinusoidal congestion which causes an increase in liver volume. The clinical manifestations can be variable but most commonly include hepatomegaly and ascites. 9 When the presentation is asymptomatic, large venous collaterals are usually present. A multicenter prospective study showed that in patients diagnosed with BCS, 83% had ascites, 67% had hepatomegaly, 61% had abdominal pain, 58% had esophageal varices, and 5% had GI bleeding. 10 This broad spectrum of clinical manifestations most likely corresponds to the duration of hepatic vein thrombosis development and progression. A mild thrombosis that forms gradually could be accompanied by the emergence of hepatic venous collaterals which serve to shunt blood away from the liver and prevent symptoms of portal hypertension from manifesting, a clinical presentation that is true for up to 15% of patients. On the other hand, if left untreated, a large and rapidly forming thrombosis can result in a severe form of liver failure that includes coagulopathy, renal impairment, and eventually death. 11
It is challenging to diagnose BCS that presents with subtle symptoms since most doctors only use the patient’s medical history to distinguish between the acute and chronic versions of the disease. As a result, CT, magnetic resonance imaging (MRI), and Doppler ultrasound are required to diagnose BCS and distinguish acute from chronic. 12 15% to 20% of cases of BCS may be asymptomatic. This is linked to either venous outflow being carried by vast hepatic vein collaterals or only 1 hepatic vein being thrombosed. 13 The CT and Doppler findings in this case report exemplify this phenomenon and highlight the need for higher suspicion of BCS in populations particularly susceptible, such as those with underlying hypercoagulable disorders or SLE. A cross-sectional study from Lahore, Pakistan, evaluated the initial presenting manifestations of SLE in 61 patients from a tertiary care hospital and reported patterns demonstrated in Figures 2 and 3. 14
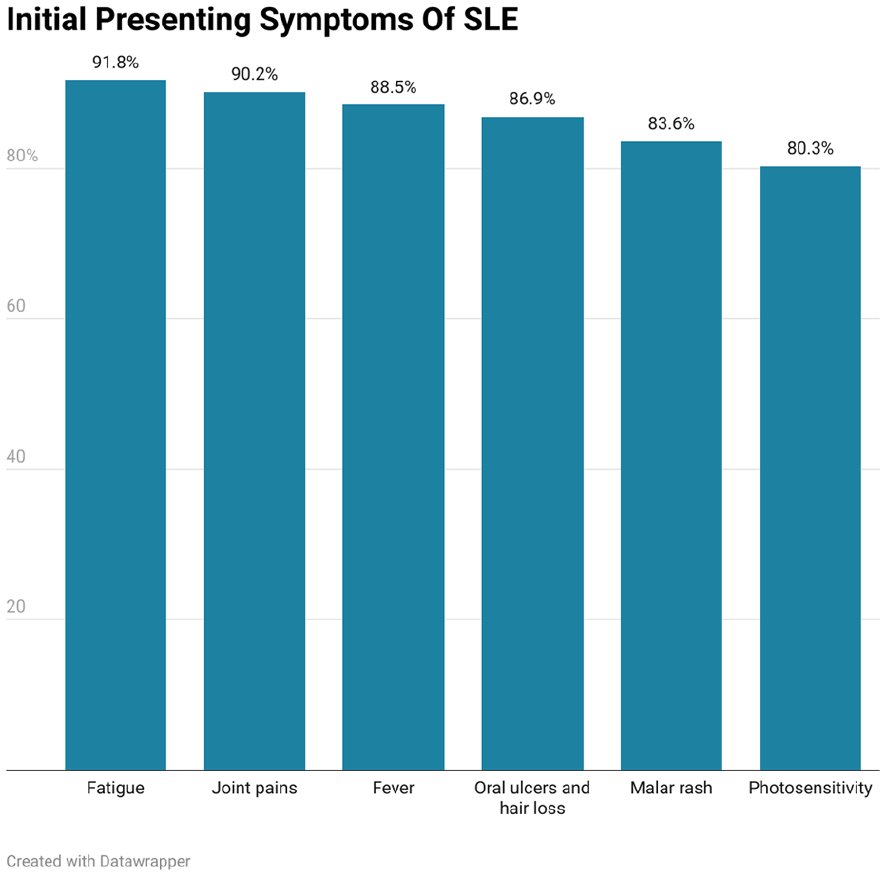
Initial presenting symptoms of SLE.

Other initial presenting symptoms of SLE.
It is very rare to see BCS as an initial presentation of SLE and only a few case reports exist in the literature (Table 4).3,15,16 The absence of classic symptoms of SLE coupled with the development of venous collaterals posed a diagnostic challenge in this case. Data on the prevalence of BCS in Pakistan secondary to APS is scarce even though it is a known risk factor for BCS, and there have been no reports of BCS as the initial presentation in a patient of SLE with co-existing APS in Pakistan to the best possible knowledge attained via literature review.
Previous Cases with BCS as Initial Presentation.

Pathophysiology of BCS and SLE-APS
Budd-Chiari Syndrome (BCS) develops when there is obstruction of the hepatic veins, the most common etiology being thrombosis. This venous outflow obstruction leads to hepatic congestion, dilation of sinusoids, ischemia, followed by fibrosis and necrosis of the liver.1,8 Patients with prothrombotic conditions are particularly susceptible to developing BCS.2,17 Common conditions include Factor V Leiden mutation, protein C or S deficiency, antithrombin III deficiency, myeloproliferative disorders, and acquired conditions such as antiphospholipid syndrome (APS).1,2,17 The patient in this case tested positive for antiphospholipid antibodies secondary to SLE. This autoimmune condition predisposes the patient to a prothrombotic state. Additionally, a co-existing factor V Leiden mutation significantly increased the risk of thrombosis in this patient. In APS secondary to SLE, circulating lupus anticoagulant and anti-cardiolipin antibodies activate platelets and endothelial cells, which increases the expression of tissue factor, ultimately inducing a hypercoagulable state which leads to blood vessel thrombosis.18,19
Management Strategies and Guidelines
The current management of Budd Chiari syndrome follows stepwise guidelines backed up by both APASL and the “European Association for the Study of the Liver (EASL).” Additional management is required for concomitant autoimmune disorders.
Lifelong Anticoagulation and Diuretics
Initiated promptly in all patients. Early anticoagulation has been shown to reduce the progression of thrombosis, promote partial or complete recanalization of occluded hepatic veins, and decrease the risk of future thrombotic events. Both guidelines recommend low molecular weight heparin followed by vitamin K antagonists/direct oral anticoagulants as long-term therapy options in appropriately selected patients. Importantly, anticoagulation is started even in idiopathic Budd Chiari syndrome which is true in 25% of cases.10,20 Furosemide and spironolactone are first-line diuretics used in the management of ascites. Non-selective beta blockers (carvedilol) are the preferred agents to prevent variceal bleeding and reduce portal hypertension. 10 In patients with active SLE, immunosuppressive therapy—particularly glucocorticoids—may be necessary to control systemic inflammation and reduce further endothelial injury, as reported in case studies of SLE-associated BCS successfully managed with steroids alongside anticoagulation,15,16 and supported by clinical data showing immunosuppression is often required in BCS secondary to APS in the presence of autoimmune activity. 18 It was not required in this case due to limited systemic manifestations.
Angioplasty and Stent Placement
In patients with anatomically favorable lesions, “Percutaneous Transluminal Angioplasty (PTA)” with/without stent placement is the next step for higher management.9,20 This approach is particularly relevant in the Asian population, where membranous IVC obstruction is significantly more prevalent compared to the West.2,20 PTA can re-establish hepatic outflow and relieve venous hypertension, often leading to symptomatic improvement and disease stabilization. 9 Furthermore, a meta-analysis of Chinese patients also reported that “Routine stenting with angioplasty is superior to angioplasty alone for preventing restenosis in patients with BCS with short-length stenosis and is safe to use as part of first-line invasive treatment,” particularly relevant to a country like Pakistan where such a concomitant procedure may not be offered initially due to resource constraints. 21
“Transjugular Intrahepatic Portosystemic Shunt (TIPS).”
TIPS is indicated if anticoagulation and angioplasty are insufficient in patients, especially in those presenting with complications of portal hypertension. 10 TIPS creates a direct, low-resistance channel between the portal and systemic venous systems, bypassing the obstructed hepatic veins and reducing pressure on the hepatic sinusoids. 10 EASL strongly advocates for early TIPS intervention in patients unresponsive to anticoagulation, emphasizing that delays may worsen liver function and reduce transplant candidacy. 10 A meta analysis conducted by Giri et al. 22 covering 1395 patients across 33 studies reported TIPS technical success of ≈99%, clinical success ≈90%, but Hepatic Encephalopathy (HE) occurred in ≈12% and liver dysfunction in ≈40%. Hemodynamic instability was a common reason for deferral, as was the case in the patient in this report. 22 An American cohort following 124 TIPS patients (non-responsive to medical treatment or recanalization) for 13 years; up until death or Liver transplant reported a mortality of 13% and transplant requirement in 6.5%. The main cause of death was liver failure. The main indications for transplant were liver failure or recurrent HE. 23
Liver Transplant
“Orthotopic Liver Transplantation (OLT)” is reserved as the final definitive step for patients with decompensated cirrhosis, progressive hepatic failure, or hepatocellular carcinoma, in whom TIPS and other interventions are either contraindicated or unsuccessful. EASL and APASL both recommend early transplant referral in patients with high “Model for End-Stage Liver Disease” scores or signs of synthetic liver dysfunction.10,20 Studies show excellent outcomes with transplantation in this setting, with 5- and 10-year survival rates often exceeding 70% to 80%. 10 Issues faced by the general population of which our patient was not exempt was the cost. An average of 45 000 USD are required for the procedure including pre transplant tests, post op care and lifelong immunosuppression. 24 Non availability of cadavers leads to the requirement of living donor transplants, which Pakistan has fortunately dealt with and accustomed itself to very well with the overwhelming majority of cases being living donor transplants. According to a retrospective study between March 2019 and April 2023 carried out at one of Pakistan’s largest transplant centres; 415 out of 416 liver transplants were living donor transplants with only 1 cadaver transplant. However, lack of trained surgeons and cadaveric shortage along with financial considerations in a relatively emerging field are matters of future discussions in Pakistani healthcare. 25
Hepatic Encephalopathy
Hepatic encephalopathy in Budd-Chiari Syndrome results from the accumulation of neurotoxins, particularly ammonia, due to impaired hepatic clearance caused by venous outflow obstruction and hepatocellular dysfunction.8,10 Management focuses on reducing ammonia production, correcting precipitating factors, and optimizing hepatic perfusion. First-line therapy includes non-absorbable disaccharides such as lactulose, which trap ammonia in the gut and promote its excretion. Rifaximin, a gut-selective antibiotic, may be added to suppress ammonia-producing intestinal flora. Supportive care includes correction of electrolyte imbalances (especially hypokalemia), treatment of precipitating infections or gastrointestinal bleeding, and ensuring adequate nutritional intake. Temporary protein restriction may be employed in severe cases but is not recommended long-term. In patients with persistent or recurrent HE despite optimal medical therapy, consideration may be given to TIPS.10,22,23 Close clinical monitoring is essential, particularly in individuals with coexisting portal hypertension or progressive liver dysfunction.
Discussion
This patient was not documented for any autoimmune disorder, especially because she resides in a rural area. Upon lab workup the patient was found to be positive for SLE and APS. The lab results also demonstrated protein C and Antithrombin III deficiency, as well as a Factor V Leiden mutation, all of which are potential risk factors for BCS, 26 however it worthy to note that the Antithrombin III and Protein C deficiency may have been secondary to the active clot with which the patient presented. The patient’s history did not point to SLE besides a single second month pregnancy loss 14 years prior, after which she had 3 children. Abdominal ultrasound revealed an enlarged liver with massive ascites. Chronic decompensated liver disease was considered but was ruled out due to normal-range liver function tests. Ascitic fluid analysis revealed Serum-Ascitic Albumin Gradient (SAAG) > 3 and normal albumin, which pointed towards a diagnosis of portal hypertension rather than cirrhosis. Furthermore, Hepatitis B core antigen and serum ceruloplasmin were also normal, excluding a diagnosis of hepatitis or Wilson’s disease.
Along with the massive ascites, the diagnosis was confirmed to be subacute BCS due to the APS secondary to SLE and the inherited hypercoagulable state. The development of collateral circulation masked the BCS for a significant period. In subacute BCS, the onset is insidious, potentially taking up to 3 months for symptoms to manifest. 8 This gradual progression allowed time for decompressive collaterals to develop, which obscured the clinical presentation. Profuse anterior collaterals as revealed in the CT findings caused the patient to develop a delayed onset of symptoms, along with normal LFTs. 13 Although BCS in patients with APS is rather uncommon, the addition of multiple thrombogenic disorders; Protein C deficiency, Antithrombin III Deficiency, and a Factor V Leiden mutation added to the complexity of the case.18,19 Based off of APASL guidelines, the patient was initially started on anticoagulants along with supportive medications. TIPS and liver transplant were offered to the patient in the case where there was no improvement in symptoms from the medication alone. 20
Conclusion
This case highlights the complex diagnostics involved in BCS, particularly in patients from a rural background who have limited access to comprehensive medical evaluations and present symptomatically. The family history of this patient was not known, however it is documented that inherited hypercoagulability is more prevalent in rural populations due to the high incidence of consanguineous marriage leading to it disproportionately affecting economically disadvantaged individuals. 26 It highlights the importance of early thrombophilic disorder screening in patients with unexplained thrombotic events and subacute liver symptoms with no history of cirrhosis or other inciting events. Additionally, it highlights the need to enhance awareness of autoimmune conditions such as SLE and APS in underserved communities to facilitate timely intervention and improved clinical outcomes. Accessible anticoagulation therapy with structured follow-up measures will contribute to better outcomes. Implementing telemedicine solutions could provide a viable means of monitoring patients in remote areas, ensuring timely medical intervention and reducing the risk of further complications.
Footnotes
Acknowledgements
The authors would like to thank Dr. Usman Ghani from the Department of Radiology, Abbasi Shaheed Hospital for assistance with image interpretation and the staff of Civil Hospital Karachi, Department of Medicine for their support in managing the patient.
Consent to Participate
Written Informed consent was obtained from the patient for the research and the publication. Signed consent forms in both English and Urdu have been made available to the editor.
Author Contributions
Khadija Malik: Resources; Data Curation; Validation. Areeb Jawed: Resources;Data Curation; Writing – Original Draft; Validation. Muddassir Syed Saleem: Conceptualization; Methodology; Writing – Original Draft; Writing – Review and Editing; Project Administration; Supervision; Validation. Nidal Bin Kamran: Methodology; Software; Writing – Original Draft; Writing – Review and Editing; Visualization; Validation. Laiba Shahbaz: Resources; Data Curation; Validation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.