
Abstract
Fahr Syndrome or Strio-Pallido Dentate Calcinosis is a rare neurological syndrome characterized by deposition of calcium in basal ganglia, which usually occurs secondary to other underlying endocrinological disorders like hypo/hyper-parathyroidism. Symptoms vary greatly and may range from psychiatric ones like confusion and hallucination to neurological like Tremors, Rigidity, with seizures being the rarest manifestation. Laboratory tests and brain imaging play a crucial role in establishing the diagnosis, while treatment primarily focuses on managing symptoms. Here, we report a case of a 17-year-old female diagnosed with Fahr’s syndrome secondary to hypo-parathyroidism, onset of the disease at such young age coupled with uncommon presentation of fits makes this case rather remarkable.
Introduction
Strio-Pallido Dentate Calcinosis, or famously known as Fahr syndrome, is rare degenerative neurological condition. The term Fahr’s syndrome was initially introduced by German neurologist Karl Theodor Fahr in 1930. It is prevalent in only 0.0001% of the general population and is characterized by deposition of calcium in the brain, primarily basal ganglia. Though basal ganglia is the most involved area, other parts such as thalamus, hippocampus and cerebral cortex can also show calcification. 1 The exact reason of these calcification is not yet established, but it is thought that disruption of Blood Brain Barrier (BBB) might be a contributing factor. 2
Often used interchangeably, Fahr syndrome and Fahr’s disease are 2 separate conditions which both involve calcium deposits in the basal ganglia. 3 However, they differ in their underlying causes and associated symptoms: Fahr’s disease is usually sporadic or genetic with no underlying cause whereas Fahr’s syndrome is a secondary condition, associated with endo-metabolic disorders such as hypo or hyperparathyroidism and vitamin D deficiency.
The symptoms usually appear later in life, around 40-50 years of age, and depend greatly upon the extent of calcification. These can range from that of Parkinsonism that is Tremors, Rigidity, Akinesia, Bradykinesia and Shuffling gait to other CNS signs and symptoms such as tetany, spasticity, dementia and depression, with seizures being the rarest manifestations.4,5
We present a case report of a 17-year-old female patient diagnosed with Fahr’s syndrome secondary to hypo-parathyroidism, who presented to ward with rare neurological manifestations of the syndrome that is seizures, also concomitant presence of malaria makes this a unique study.
Case Presentation
A 17-year-old south-Asian female presented with the complain of seizures, fever for 2 days and altered level of consciousness (ALOC) for 1 day. She was diagnosed with Epilepsy in her childhood, and was taking carbamazepine, but was non-compliant in taking medication. On admission, her GCS was 13 (E3M6v4) body temperature, blood pressure, respiratory rate, pulse and SPO2 were afebrile, 80/40 mmHg, 16 breaths per minute, 76 beats per minute and 93%, respectively. Moreover, her look was pallor, and she was anemic, other than that we found no evidence of edema, clubbing, cyanosis, dehydration or jaundice. No significant family history was present, all 6 siblings of her were fine except her.
Fever was gradual in onset, progressive in nature, initially low grade, which progressed into high, associated with burning micturition, headache, rigors and chills. Seizures were intermittent, generalized tonic-clonic associated with up-rolling of eyes, urinary retention, tongue biting and oral frothing, occurring every hour and lasting for about 5-10 minutes. The postictal phase comprised of generalized body weakness and ALOC. Further, ALOC was followed by fits, usually starting from irritability to crying. Fits remained an active complaint throughout her stay at the hospital.
During her 10 day stay at the hospital, Baseline laboratory investigations were ordered and results are shown in Table 1, other labs indicated a serum calcium was 6.8 (mg/dl) suggesting hypocalcemia, serum alkaline phosphatase was 279 μ/l. Serum Thyroid Stimulating Hormone (TSH) and Parathyroid Hormone (PTH) were ordered to rule out any endocrine cause. TSH levels were 0.901 μIU/ml and PTH were 6.49 pg/ml, respectively, indicating hypo-parathyroidism. Serological tests for malaria came back positive while dengue, hepatitis and HIV were negative. The patient was initially treated with Artemether and lumefantrine 80/480 mg for malaria and Paracetamol 1 g/100 ml for fever management. A 2cc dose of corticosteroids was administered, and Valproic Acid 500 mg was prescribed for seizure control, later substituted with Levetiracetam 500 mg. Ceftriaxone 1 g was initiated to address infection, and intravenous 10% Calcium Gluconate 200 mg was given to correct hypocalcemia.
Baseline investigations.
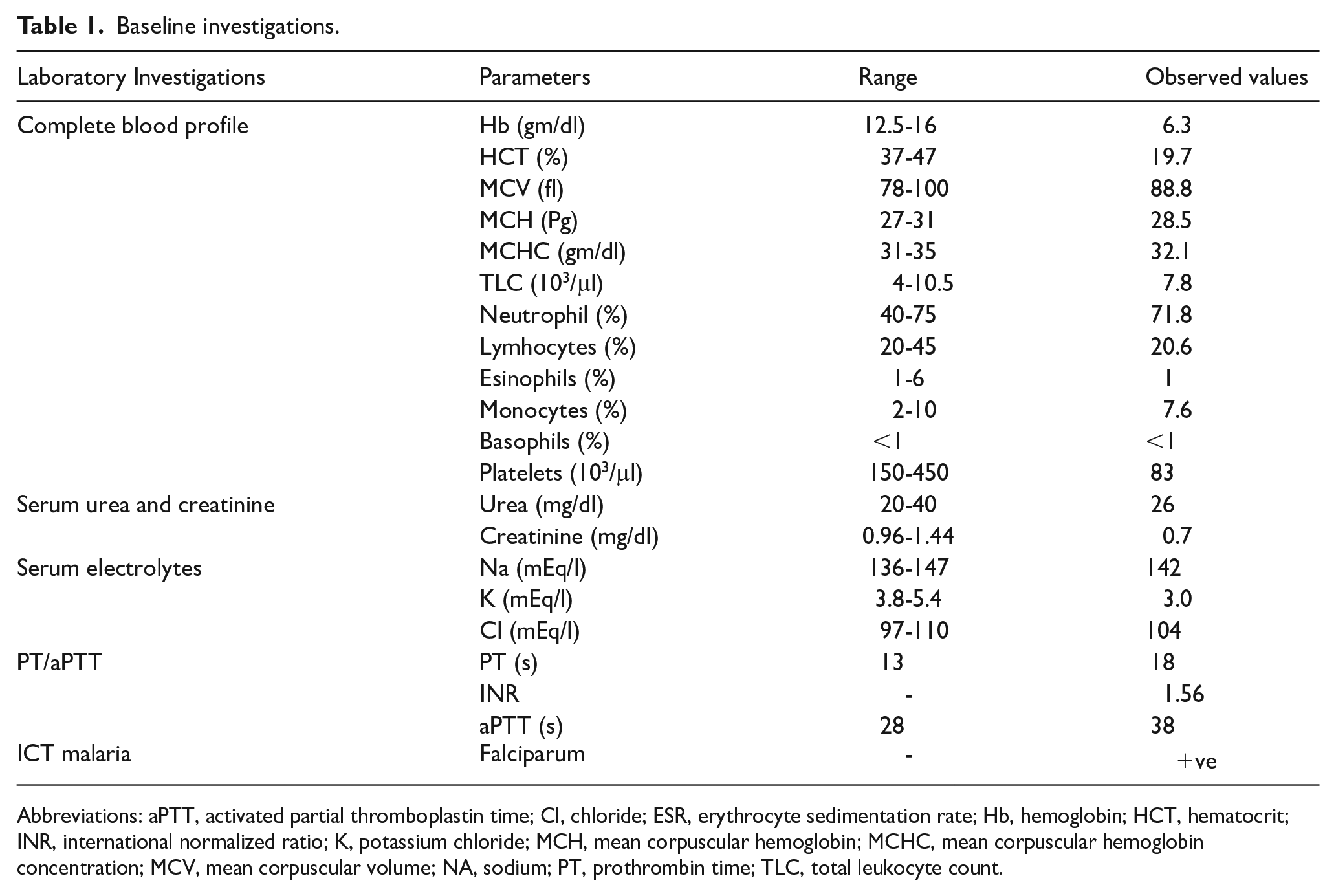
Abbreviations: aPTT, activated partial thromboplastin time; Cl, chloride; ESR, erythrocyte sedimentation rate; Hb, hemoglobin; HCT, hematocrit; INR, international normalized ratio; K, potassium chloride; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; NA, sodium; PT, prothrombin time; TLC, total leukocyte count.
Computed Tomography of the head showed bilateral hyper dense areas in basal ganglia and subcortical white matter as shown in Figure 1. Magnetic Resonance Imaging showed Abnormal T1, hypo intense signals in basal ganglia and subcortical white matter, confirming calcium deposition as shown in Figure 2.

Contrast enhanced CT scan showing hyper density in Basal Ganglia and subcortical white matter which indicates either calcifications or hemorrhage.

MRI of the patient showing T1 hypo intense area confirming calcium deposition in the basal ganglia and in the surrounding white matter.
Multiple differentials were made. At first Cerebral malaria was suspected due to altered mental status and positive falciparum strain. On the second day, her CBC and CT scan were received and Subarachnoid hemorrhage was kept as diagnosis due to radiology findings and low platelet count and patient was started on Triple H therapy. Later, MRI was done, and endocrinological workup along with serum calcium confirmed the diagnosis. But since Fahr’s syndrome diagnosis is made by exclusion, patients MRA was also done to rule out any intracranial hemorrhage, but the findings were unremarkable, and thrombocytopenia was considered to be due to malarial infection.
Hence, based on the above, a diagnosis of Fahr’s syndrome with hypoparathyroidism was made and the patient was started on 10% calcium gluconate and Vitamin D supplements. She was also prescribed carbamazepine for management of epilepsy. Upon discharge, the patient’s condition was well controlled, and no episodes of fits were noticed but the patient did not return for subsequent follow-up appointments and was therefore lost to follow-up.
Discussion
Fahr’s syndrome is reportedly more frequent among men in their 30-40s with male to female ratio of 2:1.5,6 Occurrence of Fahr’s syndrome is rare in children and patients often present with movement as seen in our case. 1 The syndrome is difficult to diagnose clinically, due to the multitude of symptoms it can present with, ranging from both neuropsychiatric to motor. However, based on existing literature, seizures seldom occur, which was yet another unique finding seen in this case.4,7 Mood disorders is the most common psychiatric symptom seen in such patients, our patient however demonstrated psychosis as she was reportedly seen crying, screaming and thrashing at random occasions. 8
Patients with Fahr’s syndrome are often misdiagnosed due to the rarity of the disease, 9 which was also the case with our patient, her history with epilepsy and co-existence of malarial infection also confused us, but CT scan reporting done by neurology department eventually led us to the diagnosis, Additionally, we also sought to rule out other causes that could potentially lead to same condition, such as pseudo-hypoparathyroidism, which was excluded due to a decreased level of PTH. Epilepsy was also eliminated as CT findings did not show any atrophy in brain parenchyma.
Different imaging techniques are used to make the diagnosis of Fahr’s syndrome, CT scan however is considered superior to MRI since it is more sensitive to calcifications, whereas MRI can act as a useful tool in predicting the progression of disease. In our case, Both CT scan and MRI were done to make a definite diagnosis. 10
Though perpetual with the disease, the exact reason for deposition of calcium in basal ganglia is not yet fully understood, it is thought that disruptive blood brain barrier, high cerebral flow and metabolic rate to this particular region could be the reason for this development.2,6 Calcium phosphorus abnormalities due to hypo-parathyroidism are found to be the most common cause for calcification, which was found consistent with our case, too. 11 However, the reason behind hypo-parathyroidism could not be figured out due to the lack of resources and non-compliance of the patient.
Another rare manifestation in our patient was the presence of thrombocytopenia, of which only one case is reported, 10 however we believe that malaria might be the real culprit behind the deranged platelet level since thrombocytopenia is one of hallmark of malaria fever, especially in falciparum subtype. 12
Additionally, psychiatric symptoms in this patient might be due to malaria too, as plasmodium falciparum is often associated with psychosis, 13 and since the patient did not show any similar symptoms in her earlier life and had no complaints other than seizures and recovered after few days also strengthened our suspicion.
Literature search suggests that both Fahr’s syndrome and hypo-parathyroidism are genetic or familial. Genes including SCL20A2, PDGFB, PDGFRB and XPR1 have been found to play a crucial role in the pathogenesis of Fahr’s syndrome, with SCL20A2 being the most involved one, followed by PDGFB and PDGFRB respectively. 14 Our suspicion also points toward genetic mutation since the patient had complaint of seizures from early childhood, but not familial since no one from her family developed such symptoms. Unfortunately, due to lack of advanced labs in our area, we could not run further genetic analysis.
Treatment for Fahr’s syndrome depends significantly on the extent of symptoms. The main goal of the treatment is to maintain the calcium and vitamin D levels, while simultaneously preventing further deterioration of the patient. For seizures, antiepileptics that is carbamazepine or Levetiracetam are prescribed, similarly for hypocalcemia, calcium and Vitamin D supplements are recommended. In some cases, Carbamazepine and Phenytoin are seen to worsen vitamin D deficiency, due to which Levetiracetam is prescribed. Calcium and vitamin D supplements are usually enough to maintain normal levels, but in severe hypocalcemia, IV calcium gluconate can also be given. 15
Multiple treatments options for treating the root cause; Hypoparathyroidism have been put forth which include human recombinant Pth and PTh 1-34, but their efficacy and safety is still questionable. 16
Conclusion
Though rare, it is imperative for researchers and practitioners to think and investigate for Fahr’s syndrome when coming across a patient presenting with vague CNS symptoms like seizures and psychosis. Additionally, the possibility of the said syndrome must not be ruled out only due to the lack of prevailing family history.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written Informed Consent was obtained from the legal guardian of the patient for the publication of this case report.
Author Contributions
Final approval of the version.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.