
Abstract
Ventricular septal defect (VSD) represents a severe complication that may manifest after a myocardial infarction (MI), typically occurring between 2 and 7 days later. Due to advancements in reperfusion management, the incidence of VSDs after MI has become very rare, occurring in approximately 0.2% of MIs. The current guidelines recommend urgent post-infarction VSD (PI-VSD) closure. We report a case of a patient with a VSD, which was diagnosed 2.5 years after MI. At the time of acute inferior MI, the patient was managed with primary percutaneous intervention in the culprit artery, and 1 month later coronary artery by-pass grafting (CABG) was completed. Twenty and thirty months after AMI patient presented with ventricular tachycardia (VT). Following the second VT episode patient was hospitalized for further examination. Echocardiography revealed the presence of VSD at the site of inferioseptal wall aneurysm. An ICD was implanted owing to recurrent malignant rhythm disorders. In conclusion, although the PI-VSD might have been overlooked and the patient missed the chance of concomitant CABG and VSD repair, this case has reached a 3-year survival, which appears to be the longest survival recorded in a medically treated patient with PI-VSD.
Introduction
Interventricular rupture represents a severe complication that may manifest after a myocardial infarction, typically occurring between 2 and 7 days later. Depending on the extent of the ruptured area, this condition causes significant clinical symptoms, including hypotension, heart rhythm disturbances, and dyspnea. During the pre-thrombolytic era, 1% to 3% of patients with acute myocardial infarctions (AMI) experienced this deadly consequence. 1 Due to advancements in thrombolytic therapy, the incidence of ventricular septal defect (VSD) after myocardial infarction has decreased to 0.4%, as indicated by the GUSTO-I study, which analyzed 41 021 patients across 1081 centers in 15 states over a 5-year period. 2 Following the implementation of reperfusion techniques such as PCI (percutaneous coronary intervention), the reported incidence of interventricular rupture has decreased even more. Acquired VSD presents a serious complication that requires prompt treatment and management. The current American College of Cardiology Foundation/American Heart Association (ACCF/AHA) and the European Society of Cardiology (ESC) guidelines recommend urgent post-infarction VSD (PI-VSD) closure, regardless of the patient’s clinical status. 3
We report a case of a patient who survived for 3 years with a PI-VSD and presented with ventricular tachycardia (VT).
Case Presentation
A 58 year old Caucasian male patient presented to our Emergency Center with complaints of rapid heartbeat and breathing difficulties. Patient reports that about 2.5 years earlier suffered AMI managed by primary PCI, followed by coronary artery bypass grafting (CABG) 1 month later. Medical documents revealed that patient had inferior AMI. Coronary angiography, at the time, discovered a triple vessel coronary artery disease, with culprit lesion in RCA, which was totally occluded in the proximal segment. A primary PCI was performed and one drug eluting stent was deployed. The left coronary system had the following stenosis: Left Main coronary artery: 50%, LAD: 95% in proximal segment, First Diagonal: ostial 95%, LCX: 75% in the proximal and mid segment and OM-1: ostial 85% stenosis. The discharge list from Cardio Surgery Clinic indicated that triple by-pass surgery was performed and he was taking the following medications: aspirin 100 mg/day, clopidogrel 75 mg/day, metoprolol 75 mg/day, furosemide 60 mg/day, and atorvastatin 40 mg/day.
Twenty months after the AMI he experienced an episode of rapid heartbeat, which was managed by Direct Current (DC) cardioversion in a regional hospital. Patient was released the same day with additional antiarrhythmic therapy (amiodarone 400 mg/day).
The patient also had a history of hypertension and was diagnosed with type 2 diabetes mellitus 2 years ago. Furthermore, he reported a positive family history for coronary artery disease.
Initial work up, revealed on lung auscultation bilateral crackles on the basal halves of the thorax. Auscultation of the heart discovered a holosystolic murmur with intensity 4/6, with punctum maximum at the lower left systolic border. Arterial pressure was 90/60 mmHg. In the ECG obtained at the Emeregency Center, ventricular tachycardia was demonstrated (Figure 1A). Patient was converted after several DC shocks (Figure 1B). The patient was admitted to the Cardiology Clinic for additional investigations due to VT and pulmonary edema. Biochemical tests, including Troponin and electrolyte levels were within reference range.
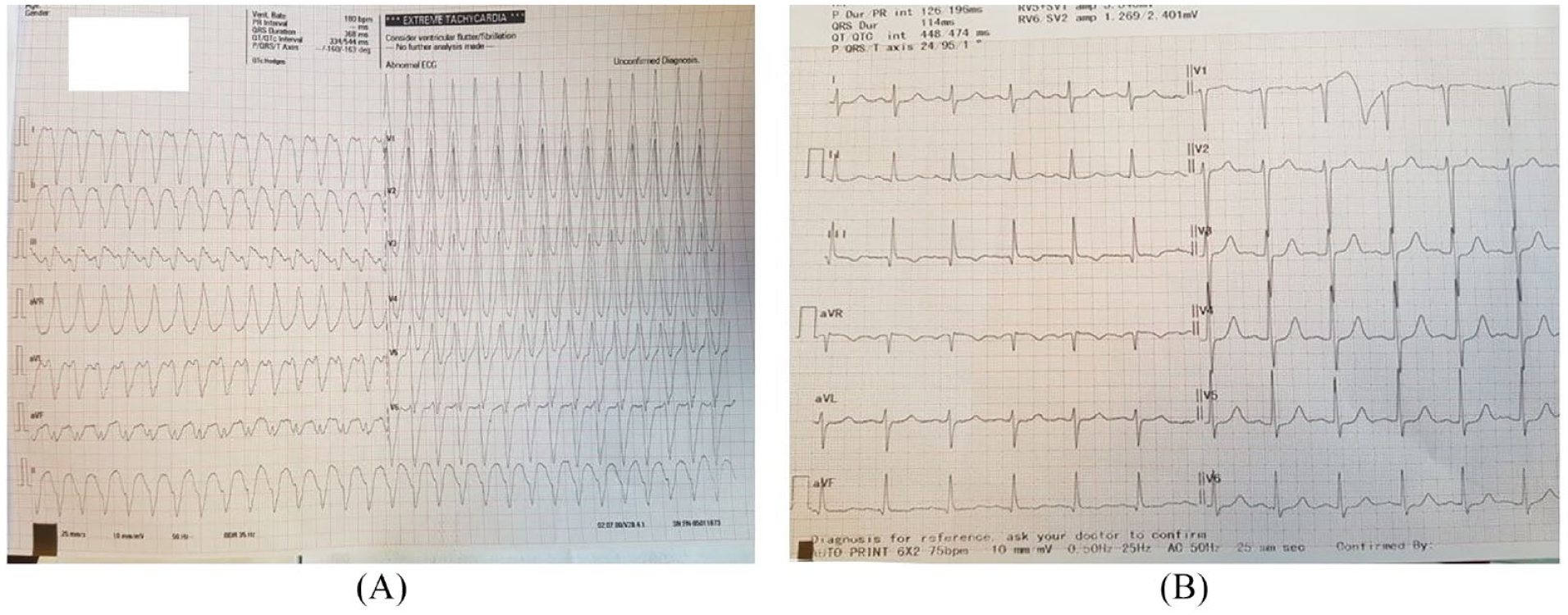
(A) ECG at admission shows ventricular tachycardia and (B) ECG obtained after DC cardioversion.
Echocardiography demonstrated a dilated left ventricle, with end-diastolic diameter of 63 mm, mildly reduced left ventricular ejection fraction of 45%, and pulmonary artery systolic pressure of 40 mmHg. It was notable a marked aneurysm of the basal segment of the inferoseptal wall. With a slight tilt of the ultrasound probe an interventricular defect within the aneurysm site was detected (Figure 2). Color Doppler illustrated blood shunting from the left to the right ventricle and a Qp:Qs = 2.7 was determined. Transesophageal echocardiography was also performed. At the level of the aneurysm (Figure 3), interventricular communication with dimensions up to 8 mm was confirmed, registered by 2D doppler, color doppler, and contrast administration (Figure 4). All heart chambers were dilated.

Transthoracic echocardiography using Color-Doppler shows the interventricular communication at the site of the inferoseptal aneurysm.

Transesophageal echocardiography showing the extent of the aneurysm.

Transesophageal echocardiography showing the “washout” phenomenon due to a dilution of right ventricular contrast medium resulting from left to right shunting.
PI-VSD and VT were the diagnosis related to the this hospitalization. In consultation with the Cardiac Surgery Team, the possibility for a re-operation was discussed. Nevertheless, given the elevated risk associated with re-operation and the patient’s stable clinical condition following in-hospital treatment (NYHA class I), the open-heart surgery was deferred at that time. The decision was made to proceed with the implantation of an ICD device owing to recurrent malignant rhythm disorders. However, if the patient’s condition deteriorates, surgical closure of the defect was recommended. Percutaneous closure of the VSD was not an option due to a lack of expertise in this procedure in our center.
One month later, the patient was admitted for ICD implantation. We advised the ICD implantation team to be very cautious during the lead positioning due to the interventricular aneurysm and defect. The procedure was carried out successfully and without any complications. (Figure 5). He was discharged from the hospital with the following medications: carvedilol 6.25 mg twice daily, furosemide 125 mg/day, spironolactone 25 mg/day, aspirin 100 mg/day, empagliflozin 10 mg/day, and insulin therapy.
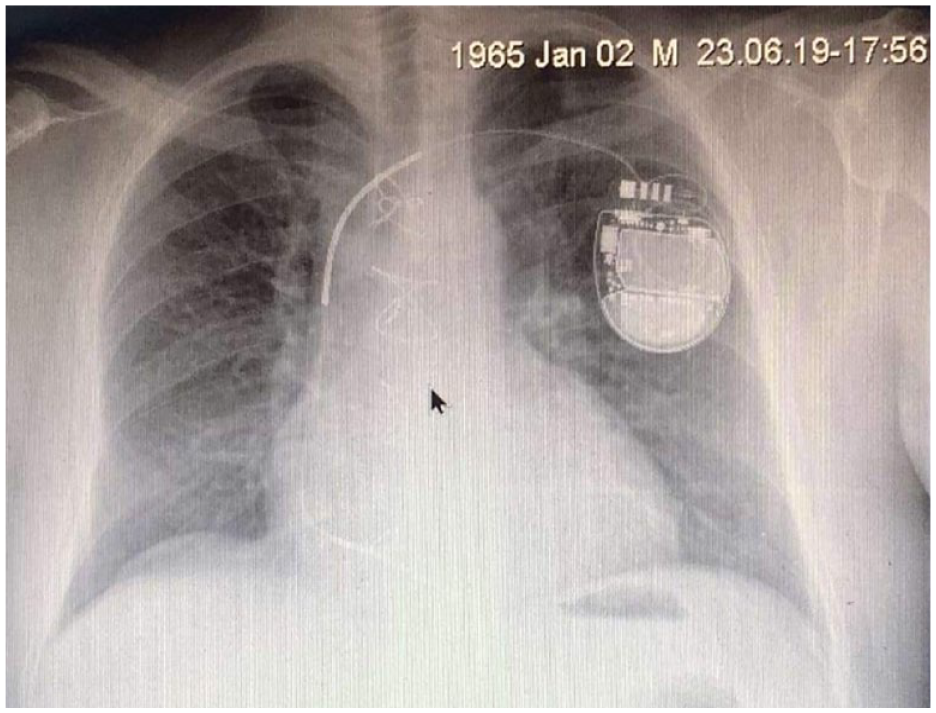
Chest X-ray showing the implanted ICD device.
Eight months later, the patient is in a stable condition, in functional NYHA class I and does not report any heart beat problems. The ICD routine check did not register any malignant rhythm events during this period. Patient remains with the same medical therapy.
Discussion
In the era of reperfusion therapy, Post-MI VSDs have become relatively rare, occurring in approximately 0.2% of myocardial infarctions. 4 Typically manifesting within the first 24 hours or between 3 and 7 days post-AMI, these VSDs are associated with significantly elevated morbidity and mortality rates. The in-hospital mortality rate remains above 90% with medical treatment and ranges from 19% to 60% with a surgical intervention. 5 The estimated survival stands at 8% after 30 days and drops to less than 3% at the 1-year mark. 6 Furthermore, a VSD occurring after an inferior myocardial infarction generally has a worse prognosis compared to a VSD associated with an anterior myocardial infarction. 2
Our case represents an exceedingly uncommon scenario wherein the rupture, as a complication of a myocardial infarction, identified 2.5 years after the acute coronary event. Remarkably, the patient not only survived but also underwent aorto-coronary bypass surgery before the rupture was eventually discovered. This unique condition underscores the complexity and subtleties involved in diagnosing and managing post myocardial infarction complications. The extended duration between the initial incident and the revelation of the rupture adds a distinctive dimension to this case, prompting further exploration into the factors contributing to such delayed manifestations, patient survival, and potential missed diagnosis. There might be a few explanations for the possible overlooked diagnosis of the PI-VSD. Firstly, the competence and the application of cardiac auscultation as a clinical skill has been greatly reduced in the last decades. As far back as 1963, Harold Nathan Segall suggested that by 2016, after 2 centuries of its clinical use, the classic stethoscope would become obsolete and replaced by new advanced techniques. 7 Reliance on technology for cardiovascular diagnosis seems to have reduced the importance of a thorough physical examination at the bedside. Numerous studies have revealed that the present proficiency in physical examination techniques, particularly cardiac auscultation, among both students and practicing clinicians, is surprisingly insufficient.8-10 This deficiency has notable implications for patient safety, medical decision-making processes, and the delivery of cost-effective healthcare, as it might be the case for our patient. Secondly, echocardiography needs to be performed cautiously in patients after myocardial infarction. The VSD in our patient was not readily noted. A particular angulation was required to be able to visualize it. It is specified that when assessing a VSD using echocardiography, proper angulation is crucial for accurately visualizing the defect and assessing its size, location, and hemodynamic significance. 11
The patient experienced 2 episodes of VT, which were converted with DC shocks. Arrhythmias are the leading cause of hospital visits for patients with ventricular septal defects, despite VT being less common in this group. 12 For these vulnerable patients, arrhythmias can be a sign of hemodynamic decompensation, or can themselves result in rapid decompensation. Given the normal levels of electrolytes and troponin, only mildly reduced left ventricular function, and the absence of proarrhythmic drugs, the VSD remained the most likely cause of VT in our patient. Management of patients with ventricular arrhythmias is complex. In outpatient or non-specialist settings prompt referral is important. In-hospital management requires multispecialty input in a dedicated specialist setting. 13 In this case presentation, the regional hospital team’s failure consisted in discharging the patient after the initial VT without conducting additional detailed examinations.
In our extensive research on reported cases of myocardial infarction and interventricular rupture complications, this particular case is unique. To date, no other instances akin to this one have been documented in the literature. What sets this case apart is the unexpected survival of the patient for a duration of 3 years post-myocadial infarction, especially considering that the rupture was discovered after the patient had undergone coronary aorto-bypass surgery, 1 month following the myocardial infarction. Knowing the time frame of occurrence of PI-VSDs, it is highly likely that the patient had this complication at the time of surgery. Subjects who undergo concomitant complete revascularization at the time of surgical repair of VSD, have better in-hospital and long-term survival, and improved cardiac function.14,15 Therefore, concomitant surgical revascularization should be performed whenever possible at the time of VSD repair.
This case may serve for prompting a reevaluation of existing paradigms and necessitating further exploration into the factors contributing to the prolonged survival and delayed discovery of the ventricular rupture.
Conclusions
This case draws several important conclusions. There are a few failures that need to be addressed. Lack of utilization of basic examination techniques, such as heart auscultation, which is unfortunately in large scale replaced with more advanced techniques and in general it is considered an essential clinical skill in decline. A high intensity holosystolic murmur wouldn’t be missed if the patient was methodically examined. Secondly, a meticulous echocardiography examination should be performed in all patients undergoing CABG. Several angulations are needed to depict certain abnormalities. Cardiac disorders occurring concurrently should be addressed and corrected in the course of the same operation. Thirdly, when ventricular tachycardia occurs, it is always important to investigate thoroughly the possible cause. However, despite the errors, our patient defied the odds and survived a condition with a very poor prognosis and a high mortality rate if medically treated. To the best of our knowledge, the patient has achieved a 3-year survival with a satisfactory functional status, which appears to be the longest survival recorded in a medically treated patient with PI-VSD.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AB played a primary role in diagnosing the patient and designing the manuscript. NR was responsible for managing the patient. All authors contributed equally to the writing of the manuscript.
Patient Consent
Written informed consent was obtained from the patient for publication of this case report. CARE guidelines were applied for this case.