
Abstract
Background:
The giant cell tumor of the tendon pod is a benign neoplasia that can be present in any bone or tendon pod. Its etiology is unknown. Nevertheless, it is related to a chronic inflammatory process. It usually occurs in women between the third and fifth decade as a palpable and painless mass and slow growth, although it can be deformed and lead to limb loss.
Case presentation:
In this report, we present the case of an 11-year-old male patient, which began on June 21, 2020, with a blunt trauma. An ultrasound was performed, reporting compatible data with synovial sarcoma. Magnetic resonance was requested, with mass evidence in soft tissues in central and planting portions. A surgical procedure with a split and biopsy of the mass was carried out. The specimen was sent to the Pathology Department, leading to a diagnosis of a giant cell tumor of the tendon pod.
Conclusions:
The giant cell tumor of the tendon pod is rare. However, in some cases, it is crucial to consider it as a differential diagnosis. The surgical management of this entity has proven to reduce recurrence rates.
Background
Tendon Sheath Giant Cell Tumor (TSGCT), also called tendon-synovial giant cell tumor, is a slow-growing, benign tumor in the tendon sheath or bursa. TSGCT is a type of tumor that mainly occurs in the hand. A previous study reported that only 3% to 5% of TSGCT cases are detected in the foot and ankle. 1 It is considered a benign tumor of slow and expansive growth originating in the tendon sheath or soft tissue. It was described by Chassaignac in 1852, 2 and encompassed in the descriptions of Jaffe et al. 3 The spectrum ranges from pigmented fleece synovitis lesions to, in rare cases, pigmented villonodular. It can be localized or diffuse histopathologically. It presents multinucleated giant cells, histiocytes, and hemosiderin deposits. 4 The etiology of this tumor is unknown. The most accepted theory establishes the presence of the development of reactive hyperplasia associated with a chronic inflammatory process related to trauma predominantly. It is also related to lipid metabolism alterations, osteoclastic proliferation, and vascular infection disorders. 5 Its most frequent presentation is in the hand when it is localized. Otherwise, when it is in its diffuse form, it appears in joint areas that support the load. The prevalence varies between the third and fifth decade of life, predominantly in women, 6 representing around 1.6% of the total soft tumors. 7 It is presented as a palpable mass, painless, of slow growth, pain, and functional disability. These types of tumors are rare in pediatric ages. They are of slow growth, but with locally aggressive behavior, being able to invade adjacent structures, generating deformities and, therefore, if they are not handled promptly, they can generate limb loss or affected site.
Case Presentation
The case was an 11-year-old male who began with his condition on June 21, 2020, presenting direct trauma at the level of the thirrd toe of the right foot. It started with pain, increased volume, and hyperemia. It was managed with a topical analgesic without clinical improvement (Figure 1). A USG was requested, reporting data compatible with probable synovial sarcoma. Also, a magnetic resonance study (RM) was carried out (Figure 2).

Plantar (A) and dorsal (B) vision of the right foot, show an increase in middle finger volume.
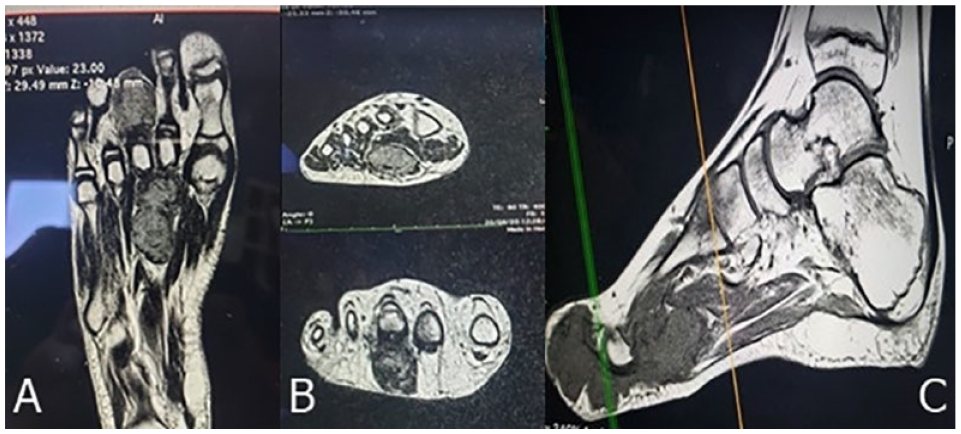
Coronal (A), axial (B), sagittal (C) planes, in sequence T2 where 2 components are appreciated at the central level, peritendinous at the level of the third and second toe, corresponding to tumor mass.
On September 20, 2020, an RM study was carried out in which the presence of mass in soft tissues in the central portion and planting of the foot was corroborated, with 2 peritendinous components, lobed, surrounding the flexor tendons in a circumferential form with predomination in the third toe, displacing the flexor tendon of the second toe in a medial direction. In a T2 sequence study, it was observed hyperintensity in the bone marrow of the tarsus and metatarsal bones. A vascular assessment was not performed (Figure 2).
A surgical protocol was performed with tumor exeresis and biopsy, finding two 3 × 2 and 2 × 1.8 cm2, soft, whitish, cystic, with a peritendon involvement (Figure 3).

Growth tumor view during surgery. A plantar approach was performed, with exposed tumor mass.
It was sent to the Department of Pathology (Figure 4), corroborating histopathologically and immunohistochemically the diagnosis of giant cell tumor of the synovial sheath with the following characteristics: the histological type was a synovial pod giant cell tumor; the tumor size for histological study was a fragment greater than 3 cm in the major axis; it was grade 1 according to Fédération Nationale des Centres de Lutte Contre le Cancer; in mitosis was classified as grade 1 (0-9 mitosis per High Power Fields); the lymphovascular invasion was no identified; Vimentin+/CD68+/Ki67+/CD34−/S100− was the result of immunochemistry (Figure 5).
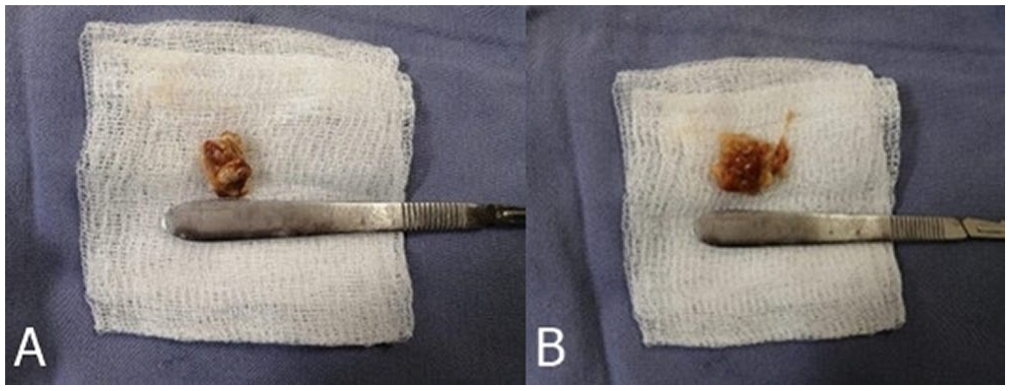
Macroscopic view of tumor pieces: (A) 2 cm × 1.8 cm piece and (B) 3 cm × 2 cm piece.
Figure 4 shows 3 histopathological cuts.

Histological cuts examined in the pathology department. It is observed a lesion formed of cells of histiocytic aspect with ill-defined borders, nuclei with fine chromatin, and scant cytoplasm. There are also multinucleated giant cells of regular distribution and several collagenized areas. (A) It shows a panoramic of the cut. (B) It shows an x40 zoom. (C) It shows positivity to an immunohistochemical CD68 study.
The patient was discharged without any associated complication, monitoring the external consultation with radiographic and clinical controls, ultimately presenting on June 15, 2022, to consultation at the time without presenting recurrence data of the lesion (Figure 6), maintaining plantigrade, without support, absence of pain, adequate healing of the surgical site as well as satisfactory incorporation into their daily activities, currently in follow-up, without eventualities and, without recurrence data at the time of its last assessment.

Plantar vision almost 2 years after surgery.
Discussion
The TSGCT is a soft tissue tumor that comes from the tendon sheath complex and the periarticular tissue of the small joints in the hand. It is the second most frequent benign tumor of the ganglion. 7 It affects individuals between 30 and 50 years, with a predominance in women. 3 The etiology of this entity is not well defined. It is more related to reactive hyperplasia associated with a chronic inflammatory process related to direct trauma on the limb. 5 It can also be associated with a deficit in lipid metabolism, osteoclastic proliferation, infection, vascular condition, and other immune mechanisms. 7 In the series of cases reported by Di Grazia et al 3 and Zhang et al, 8 the most frequent site of this lesion is in the hand. Nevertheless, they have been observed to a lesser extent at the foot and ankle. This tumor can be local or diffuse, presenting a nodular or multilobular growth pattern predominantly affecting joint or tendon movement. 9
The diagnosis of this pathology can be carried out in a clinical form, presenting an increase in volume, functionally, and occasionally immunohistochemical. 10 Clinically, this entity is manifested as a palpable, painless, slow growth. Pain is rare. Nevertheless, according to Piamo-Morales et al, 7 its prevalence was up to 21%. Histopathologically, we can consider the following transoperative characteristics: a tissue of gummous consistency, lobed, with an average size between 3 and 3.5 cm, brown color considering the predominantly as blood trace data, taking as reference the characteristics described in the series of cases of Zhang et al. 8 In the immunohistochemical study it is noteworthy that in our case the S100 marker is negative, presenting results like the series of cases published by Mizuno et al. 11 Therefore, based on the bibliography consulted, the management of choice for this pathology is the complete excision of the tumor and surveillance of the same since a prevalence of recurrence of up to 45%.11,12
Conclusion
The TSGCT is a rare tumor in the pediatric ages. However, based on the presentation site and its clinical manifestation, it is possible to make a differential diagnosis concerning other tumor pathologies. Surgical management of this pathology is the procedure that has proven to reduce the recurrence rate. Even so, it is necessary to follow up on these patients since, due to the type of injury, they may have recurrence and more aggressive behavior.
Footnotes
Author Contributions
Carlos Enrique Grimaldi-Valencia participated in the patient care, in the collection of data of the file, and wrote the first draft. Alberto Celis-Ochoa participated in the patient care, in the collection of data of the file, and wrote the first draft. José Juan Ramírez-García participated in the patient care and participated in to write the first draft. Gilberto Flores-Vargas conducted the critical review of the article and the adaptation to the journal’s requirements. Nicolás Padilla-Raygoza conducted the critical review of the article and the adaptation to the journal’s requirements. All authors reviewed the final version of the manuscript and approved it.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There is not funding for this case report. If it is accepted, the Institute of Public Health from Guanajuato State will pay the fee for Open Access.
Ethics Approval and Consent to Participate
It is a review of medical files of the patient in Hospital General Leon from the Institute of Public Health from Guanajuato State.
Consent for Publication
The mother signed the informed consent to publish clinical data and images of her child. The patient gave his assent to publish clinical data and images from him.