
Abstract
Introduction:
Today, surgical errors are becoming less and less frequent, thanks to the development of new techniques and the choice of different approaches. Nevertheless, they are still possible, and it is important to mention them in order to prevent them and avoid their recurrence.
Case Presentation:
We report a case of intravesical textiloma, rarely observed in urological surgery, in an 80-year-old patient who underwent laparoscopic inguinal hernia repair and presented to a urological consultation with hematuria and irritative lower urinary tract signs. Abdominal ultrasound revealed a hyperechoic tissue-like formation in the posterior wall of the bladder. The diagnosis of a bladder tumor was therefore raised, and cystoscopy was performed, which revealed an intravesical textiloma. All foreign bodies were removed endoscopically, and the patient had a good post-operative outcome.
Conclusion:
The rarity of the urological location of textilomas and the importance of their prevention remain a goal in surgery, whatever the specialty.
Introduction
Textiloma, or Gossypiboma, is the presence of a foreign body consisting of surgical pad(s) or drape(s) left behind in an operative site. It is a rare surgical complication, most often observed in gynecological and digestive surgery, and exceptionally in urology. 1
Although most often asymptomatic and discovered by chance during radiological examinations, textiloma can nevertheless be the cause of complications, particularly infectious ones, in which surgical treatment is indicated in the majority of cases.
We report a case of intravesical textiloma in a patient who underwent laparoscopic inguinal hernia repair.
Case Presentation
This 80-year-old patient, a chronic 30-pack-year smoker, was admitted to the urology department of the Cheikh Khalifa hospital in Casablanca with a 3-week history of clotting hematuria associated with irritative lower urinary tract signs of pollakiuria and urgency.
He had undergone a laparoscopic right inguinal hernia repair 5 months previously, with no postoperative abnormalities. The patient had no particular pathological history.
On examination, the patient was in good general condition, and the clinical examination was unremarkable apart from the presence of a laparotomy scar in the right inguinal region.
Investigations
In view of the hematuria, a urinary ultrasound scan was performed, which revealed a hyperechoic tissue-like formation in the posterior wall of the bladder. The diagnosis of a bladder tumor was the first to be made, given the clinical presentation and the fact that the patient was an active smoker.
The indication for transurethral resection of the bladder tumor was given, and endoscopic exploration revealed whitish filaments characteristic of textiloma, associated with diffuse inflammation of the bladder mucosa, predominantly in the left lateral wall (Figure 1).
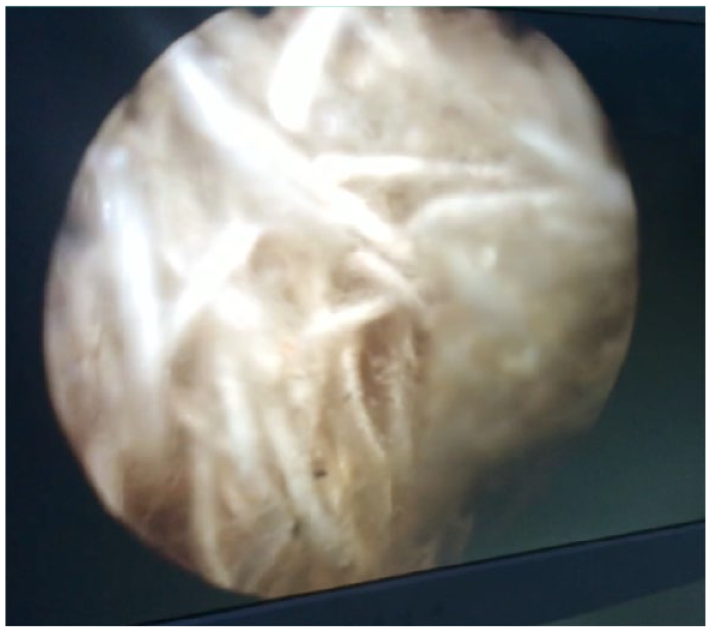
Characteristic whitish filaments of textiloma in the bladder visualized by cystoscopy.
Biopsies of the peri-lesional bladder wall were taken, with no evidence of malignant lesions. In addition, the patient underwent complete endoscopic resection and extraction of the textiloma (Figure 2).

Textiloma appearance after extraction.
The patient progressed well postoperatively, with disappearance of irritative signs and hematuria within 48 hours. Antibiotic therapy was initiated with Cefixime 400 mg in 2 doses over 7 days.
Discussion
Textiloma is an acquired, iatrogenic lesion resulting from the omission of a foreign body of textile origin during surgery, most often dressings or surgical drapes.
Our case report presents notable strengths, including the rarity of the documented intra-bladder textiloma, which contributes to the limited body of literature on this condition. Additionally, the unpublished experience of managing such a complication adds to the existing knowledge base. However, the study is limited by the lack of high-quality perioperative images, preventing a comprehensive evaluation of the bladder wall condition and the assurance of complete foreign body removal. Addressing these limitations in future research would enhance the validity and thoroughness of the findings.
Its actual incidence is difficult to predict for medico-legal reasons. 2 According to reports, gossypiboma occurs in 1/4000 cases. The incidence of foreign bodies after surgery is between 0.01% and 0.001%, with textilomas accounting for 80% of cases. 3
Mainly intraperitoneal (52%) and gynecological (22%), intravesical textiloma is relatively rare, as very few isolated cases have been reported. 4 A number of factors have been reported as contributing to the omission of material, such as emergency surgery, long-term surgery, obesity, unexpected intraoperative factors and high intraoperative blood loss. 5
Patho-physiologically, clinical manifestations are mainly caused by the body’s inflammatory response to the foreign body. According to a recent meta-analysis, the most common symptoms were pain (73.8%), a palpable mass (47.6%), vomiting (35%), followed by abdominal distension and fever. 6 Urologically, bladder gossypiboma can present at any time in the postoperative period. 3 Typical presentations include urethral discharge, recurrent urinary tract infections, wound dehiscence and adhesions. 7 However, our case reported none of these symptoms, but rather episodes of hematuria and urinary irritative signs such as pollakiuria and urgency.
Most often slow-growing and asymptomatic, the diagnosis of textiloma is difficult. Ultrasound signs may correspond to an echogenic area with a posterior shadow cone, a cystic mass containing wavy hyperechoic structures, or a complex non-specific mass that may mislead the diagnosis of a bladder tumor. 8 A CT scan is recommended prior to cystoscopy, usually showing a central mass with high attenuation, a spongiform pattern of air bubbles and a well-enhanced, hyper-dense rim. 9 Nevertheless, the diagnosis of certainty remains cystoscopy, which enables the textiloma to be appreciated in a minimal invasive way.
Gossypiboma is treated surgically by endoscopy, if possible, as in our case, or by median laparotomy under the umbilicus in the event of difficulty in extracting the mass endoscopically. However, in view of the various possible complications and the need for repeat surgery, the best treatment for textiloma is prevention.
There are various methods available to prevent gossypiboma, including counting swabs at the end of the operation and using marked swabs. In most countries, surgical dressings contain radio-opaque material that can be easily identified in X-ray and CT images, facilitating their detection. On the other hand, a surgical safety protocol, such as the WHO checklist, is a simple and effective method that promotes communication between team members, can form part of institutional policies to improve surgical safety and patient care, and prevent complications such as textilomas. 10
Conclusion
Intravesical textiloma is a rare complication posing a medico-legal problem, and its treatment is based on its removal, at best endoscopically. The circumstances in which it is discovered are variable, and may mimic a tumor or cause indeterminate pain in patients, leading to sepsis and death. Thus, the best approach to preventing such problems requires appropriate communication between members of the operating team to avoid textiloma or other surgical errors.
Footnotes
Abbreviations
CT, computed tomography; WHO, World Health Organization
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Material
On request, email the corresponding author.
Code Availability
Not applicable
Consent to Participate
Orally
Consent for Publication
Orally
Ethical Approval
Not applicable