
Abstract
Immunoglobulin G4-related disease (IgG4-RD) is an autoimmune-mediated disorder with heterogeneous multiorgan manifestations. Early identification and treatment of IgG4-RD are crucial for organ function recovery. Rarely, IgG4-RD manifests as a unilateral renal pelvic soft tissue mass that may be misdiagnosed as urothelial malignancy, resulting in invasive surgical intervention and organ damage. Here we present a 73-year-old man who had a right ureteropelvic mass with hydronephrosis detected by enhanced computed tomography. Right upper tract urothelial carcinoma and lymph node metastasis was highly suggested based on the image findings. However, IgG4-RD was suspected due to his past history of bilateral submandibular lymphadenopathy, nasolacrimal duct obstruction, as well as a high serum IgG4 level of 861 mg/dL. The ureteroscopy with tissue biopsy showed no evidence of urothelial malignancy. His lesions and symptoms improved after glucocorticoid treatment. Hence, a diagnosis of IgG4-RD was made, with the phenotype of classic Mikulicz syndrome with systemic involvement. The manifestation of IgG4-RD as a unilateral renal pelvic mass is rare and should be kept in mind. A ureteroscopic biopsy and serum IgG4 level measurement can help in the diagnosis of IgG4-RD in patients with a unilateral renal pelvic lesion.
Introduction
Immunoglobulin G4-related disease (IgG4-RD) is an autoimmune condition characterized by chronic inflammation, tissue fibrosis and organ dysfunction. 1 The incidence of IgG4-RD ranged from 0.28 to 1.08 per 100 000 people, which is underestimated owing to its nonspecific presentation. 2 Patients with IgG4-RD typically have elevated serum IgG4 levels as well as one or multiple organs involvement. The histopathological characteristics of the affected organ include IgG4-positive plasma cell-predominant lymphoplasmacytic infiltration, fibrosis, and an increase in eosinophils. 3 IgG4-RD progresses insidiously and may go undiagnosed for an extended period of time. However, delayed therapy for IgG4-RD increases the risk of irreversible organ dysfunction, such as diabetes mellitus or exocrine pancreatic insufficiency. 4 Hence, early identification and treatment for IgG4-RD are critical for healing the inflammation and fibrosis, and restoring the organ function.5,6
IgG4-RD can affect virtually every organ and typically presents as soft tissue mass and organ enlargement. The salivary glands, pancreato-biliary structures, lymph nodes, retroperitoneum, lungs, and kidneys are common organs involved by IgG4-RD, with enlargement and dysfunction of the salivary gland, autoimmune pancreatitis, lymphadenopathy, retroperitoneal fibrosis and the pulmonary mass as clinical manifestations. 5 The most common presentations of IgG4-related kidney disease include IgG4 tubulointerstitial nephritis, membranous nephropathy, hypocomplementemia and obstructive nephropathy induced by retroperitoneal fibrosis.6,7 Rarely, IgG4-RD can manifest as a unilateral renal pelvic or ureteropelvic mass. Patients with IgG4-RD may undergo nephrectomy if the lesion is misdiagnosed as urothelial malignancy. Here we present a case of 73-year-old man who had a unilateral ureteropelvic junction (UPJ) mass and lymphadenopathy. The diagnosis of IgG4-RD was made based on other distinct symptoms, a high serum IgG4 level, and the exclusion of urothelial malignancy via ureteroscopic biopsy. The patient responded well to glucocorticoid treatment and avoided nephroureterectomy.
Case Presentation
A 73-year-old man presented with bilateral submandibular lymphadenopathy, a clogged sensation around the inside corner of his eyes, and excessive tearing 5 months ago. He had essential hypertension based on the medical history and there was no family history of malignancy. The patient underwent ultrasonography-guided lymphadenopathy aspiration; the cytology result revealed benign epithelial cells and inflammatory cells. Three months later, the patient began to experience right flank pain. Ultrasonography and ureteroscopy performed at a local hospital revealed the right UPJ stricture and hydronephrosis. A double-J stent implantation for right UPJ stricture was performed. However, right UPJ stricture persisted after removal of the stent. He was then referred to our nephrology department for help.
On physical examination, there was knocking tenderness at the right costovertebral angle, as well as bilateral submandibular lymphadenopathy. The laboratory tests showed impaired renal function with a serum creatinine level of 1.54 mg/dL, and there was no evidence of hematuria, pyuria, or proteinuria in the urine examination. There was no eosinophilia, with an eosinophil count of 179/cumm. The serum levels of C3 and C4 were 64.7 and 7.6 mg/dL, respectively. The urine cytology revealed no evidence of malignancy. An enhanced computed tomography (CT) of the abdomen was performed, indicating a 3.3 cm irregular soft tissue mass with contrast enhancement at the right UPJ, right hydronephrosis, and lymphadenopathy over the left common iliac and iliac chains (Figure 1A and B).
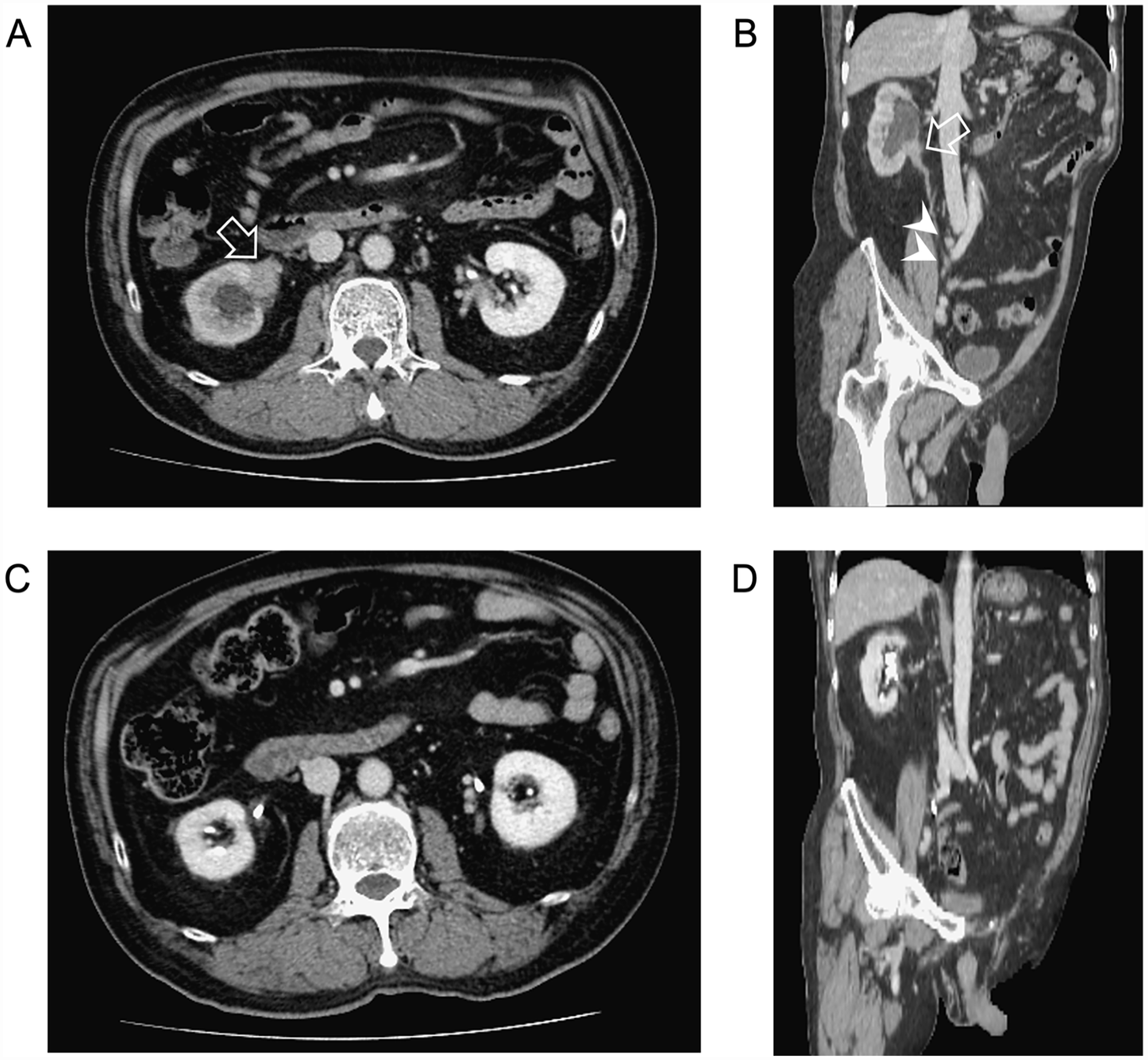
(A and B) Enhanced abdominal CT showed an irregular soft tissue lesion with contrast enhancement at right UPJ causing hydronephrosis (arrow) and lymphadenopathy over right common iliac and iliac chains (arrowheads), which was suggestive of right upper tract urothelial carcinoma with obstructive uropathy and lymph node metastasis. (C and D) Repeated enhanced CT 3 months after prednisolone treatment revealed resolution of the soft tissue mass and lymphadenopathy.
Right upper tract urothelial carcinoma with obstructive uropathy and lymph node metastasis was highly suggested based on the image findings. However, because the UPJ lesion, submandibular lymphadenopathy, and symptoms of nasolacrimal duct obstruction coexisted, IgG4-RD should be examined clinically. The serum IgG4 concentration was measured and found to be as high as 861 mg/dL. The patient underwent ureteroscopic biopsy on the right UPJ stricture instead of nephroureterectomy. The histopathologic results revealed chronic inflammation with no evidence of malignancy.
Based on the findings described above, IgG4-RD was diagnosed. Prednisolone at 0.6 mg/kg/day was administered to the patient. His right flank pain, bilateral submandibular lymphadenopathy, and nasolacrimal duct obstruction improved gradually. Follow-up abdominal CT 3 months after treatment revealed regressive change of soft tissue mass at the right UPJ and lymphadenopathy (Figure 1C and D). The serum IgG4 level declined to 328 mg/dL and his renal function improved with the serum creatinine level decreasing to 1.19 mg/dL (Figure 2).
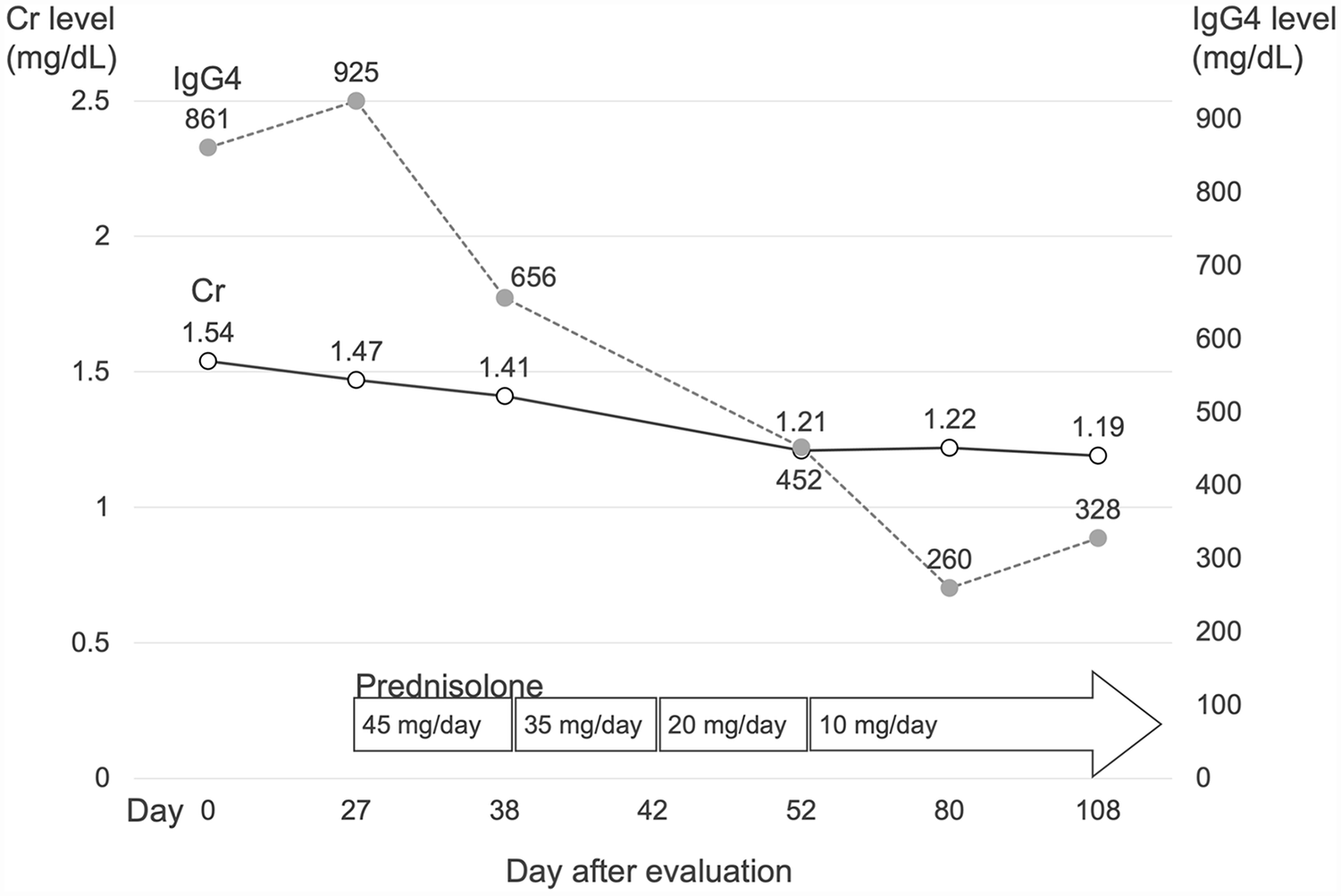
Serial serum creatinine and IgG4 concentrations before and after prednisolone treatment in the patients with IgG4-RD.
Discussion
We described a case of IgG4-RD, with the presentations of submandibular lymphadenopathy, nasolacrimal duct obstruction, 8 as well as a right UPJ mass causing obstructive uropathy. The patient had a high serum IgG4 concentration and no evidence of urothelial malignancy in the tissue histopathology. Furthermore, he responded effectively to the glucocorticoid treatment, as his symptoms and lesions resolved. According to the classification criteria for IgG4RD made by the American College of Rheumatology and the European League Against Rheumatism (ACR/EULAR), the diagnosis of IgG4-RD was confirmed in our case who met the classification criteria for IgG4-RD with total points of 25. 6
IgG4-related kidney disease may present as hypocomplementemia, bilateral renal cortex low-density patches, unilateral or bilateral renal pelvic wall thickening or soft tissue mass, and obstructive nephropathy due to retroperitoneal fibrosis. IgG4 tubulointerstitial nephritis and membranous glomerulopathy are the most common forms of renal cortex low-density patch histopathology.6,7 Among them, a unilateral renal pelvic mass is a rare presentation of IgG4-RD which could be misdiagnosed as urothelial cancer. We searched PubMed for literature review and summarized clinical characteristics of 8 patients, including our case, in Table 1.9 -15 The average was 66 years old. There were 62.5% male patients. Renal lesions were discovered incidentally in 50% of the patients. All of them had elevated serum IgG4 levels. Six out of 8 patients (75%) received invasive surgical interventions, indicating that physicians were unaware of IgG4-RD with this rare manifestation prior to surgery. Taken together, current evidence consolidates that identification of this uncommon form of IgG4-RD is important for patients to avoid unnecessary treatment. A ureteroscopic biopsy to exclude malignancy is suggested when IgG4-RD is suspected in patients with a unilateral renal pelvic mass. Serum IgG4 level measurement is also helpful in areas where tissue biopsy is unavailable.
Summary of reported cases of IgG4-RD mimicking unilateral urothelial malignancy.

In order to better recognize IgG4-RD, the ACR/EULAR IgG4-RD classification criteria committee identified 4 IgG4-RD groups with distinctive characteristics including pancreato-hepato-biliary disease, retroperitoneal fibrosis and/or aortitis, head and neck-limited disease, and classic Mikulicz syndrome with systemic involvement. 5 The clinical appearance of our patient was compatible with classic Mikulicz syndrome with systemic involvement, which is more prevalent in Asians and men. 5 The renal involvement and a high serum IgG4 level are also consistent with this phenotype.
Glucocorticoid has been suggested as the first line treatment for IgG4-RD. 16 The treatment response for IgG4-RD is evaluated based on the alleviation of clinical symptoms, the decrease in mass, or the restoration of organ function. The optimal glucocorticoid treatment dose and the treatment duration for IgG4-RD remain inconclusive. Ghazale et al proposed an induction therapy of prednisone 40 mg/day for 4 weeks, decreasing by 5 mg per week, and terminating the steroid treatment within 11 weeks. 17 However, the relapse of IgG4-RD is common after discontinuation of therapy. 18 The Japanese consensus guidelines by Kamisawa et al recommended an induction treatment of prednisolone 0.6 mg/kg/day for 2 to 4 weeks, decreasing by 5 mg per one to two weeks over 2 to 3 months, followed by a maintenance dose of 2.5 to 5 mg/day for up to 3 years.19,20 Our patient experienced regression of the right UPJ soft tissue mass as well as remission of submandibular lymphadenopathy 3 months after prednisolone treatment. However, we tapered the prednisolone dose at a relatively fast rate due to the patient’s complaints about steroid adverse reactions. The prednisolone dose will be maintained at 10 mg/day and the patient’s clinical condition including renal function will be monitored to determine the timing of decreasing to the maintenance dose or adding additional immunosuppressive agents.
The serum IgG4 concentration declined from 861 to 328 mg/dL. However, serum IgG4 level is not a reliable predictor of disease activity. Patients may experience disease recurrence even if their follow-up serum IgG4 levels are within normal range. 21 The IgG4-RD responder index is a validated tool for assessing IgG4-RD disease activity.22-24 However, the complexity of the IgG4-RD responder index scoring system may limit its application in routine clinical practice.
In conclusion, IgG4-RD manifesting as a unilateral renal pelvic mass is rare. Physicians need to recognize it to avoid unnecessary treatment. A ureteroscopic biopsy and serum IgG4 level testing can aid in the identification of IgG4-RD in patients with a unilateral renal pelvic lesion.
Footnotes
Acknowledgements
We thank the patient for granting permission to publish this information.
Author Contributions
C.W.H contributed to the conception and design of the study, analysis, and interpretation of data, and drafting the article with final approval of its completed form. C.L.C contributed to collection, analysis, and interpretation of data with final approval of its completed form. Y.C.C contributed to the drafting the article with final approval of its completed form.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for Publication
Written informed consent was obtained from the patient for publication.