
Abstract
Background:
Systemic lupus erythematosus (SLE) is an autoimmune disorder affecting multiple organs with different degrees of severity. SLE is typically diagnosed based on the presence of antinuclear antibodies (ANA) in the serum. However, seronegative SLE is rare and is diagnosed by clinicians when the patient’s ANA is negative but fulfills other diagnostic criteria.
Case report:
We report a case of a 15-year-old South Asian female with SLE who had negative antinuclear antibodies yet displayed the typical clinical presentations of photosensitive maculopapular rash, joint pain, alopecia, anemia, and thrombocytopenia. Clinical evaluations in conjunction with lab results were used to establish a diagnosis of ANA-negative SLE.
Conclusion:
ANA positivity is an entry criterion for SLE; rarely, cases of ANA-negative SLE may present. A typical clinical presentation may help determine the diagnosis in such a scenario. However, still, the physician should rule out immunodeficiency and other systemic illnesses before reaching a diagnosis of ANA-negative pediatric SLE.
Introduction
Pediatric systemic lupus erythematosus (SLE) is a multisystemic autoimmune condition mainly affecting children below the age of 18 years. 1 The incidences of pSLE range from 0.36 and 2.5 per 100 000 children, with a prevalence of 1.89 to 34.1 per 100 000. 2 Pediatric SLE is an aggressive condition and has increased morbidity and mortality as compared to adult-onset SLE. The most prevalent causes of increased morbidity and mortality are known to be the longer duration of the disease in children and immunosuppressive medication overburden. 3 Overall pediatric SLE has a grimmer prognosis, but it has been improved recently and the 10-year survival rate ranges from 80% to 90%. 4
Anti-nucleosome antibodies (ANA) are associated with various immunological conditions including SLE. The presence of ANA in the serum of a patient with other supporting laboratory values and clinical features favors the diagnosis of SLE. The clinical feature of SLE includes malar rash, fever, malaise, arthralgias, myalgias, headache, anemia, pericarditis, oral ulcers, petechiae, and loss of appetite and weight. 5 Seronegative SLE is a condition in which the patient the patient’s clinical features and laboratory values are consistent with SLE, but serology is negative for ANA. Both seropositive and seronegative SLE presents similarly and the diagnosis of seronegative SLE is challenging due to the concomitant signs and symptoms with seropositive SLE.
Different diagnostic criteria are being used for the diagnosis of SLE, some require serology positivity while others only rely on clinical features and laboratory values. Other conditions associated with ANA include ANA-associated rheumatic diseases (AARD), such as systemic sclerosis, mixed connective tissue disease, and Sjogren’s syndrome, which are characterized by the presence of autoantibodies against nuclear autoantigens and other intracellular autoantigens. Relying solely on ANA as a marker for SLE (or any of the AARDs) increases the risk of underdiagnosing ANA-negative lupus, which can delay diagnosis and treatment. If the patient fulfills the criteria for SLE despite seronegative, the diagnosis should not be delayed.6,7 We herein, report a case of a 15-year-old female diagnosed with systemic lupus erythematosus due to its rare occurrence the in pediatric age group.
Case Report
A 15-year-old female patient presented to the outpatient department of tertiary care hospital with an erythematous rash on the face, easy fatiguability, and joint pain for 2 months. The rash began over her face and spread to bilateral upper extremities and was photosensitive and pruritic. On further inquiry, the patient also has pain in the small joints of her both hands that are associated with joint stiffness more prominent at night and remained for less than 20 minutes. There was no associated fever, weight loss, and no proximal muscle weakness. The patient was an 8th-grade high school student with no significant past medical history. Family history was unremarkable for malignancies or rheumatologic disorders. She had regular menses with normal flow and has been taking a balanced diet. The patient used oral non-steroid anti-inflammatory drugs (NSAIDs) for joint pain. On examination, the patient was vitally stable with the vital signs of blood pressure of 120/80 mm Hg, a pulse rate of 88 beats per minute, a respiratory rate of 17 breaths, and a temperature of 37°C. There was an erythematous maculopapular malar rash on the face involving the forehead, nasal bridge, and bilateral cheeks with sparring of nasolabial folds (Figure 1).
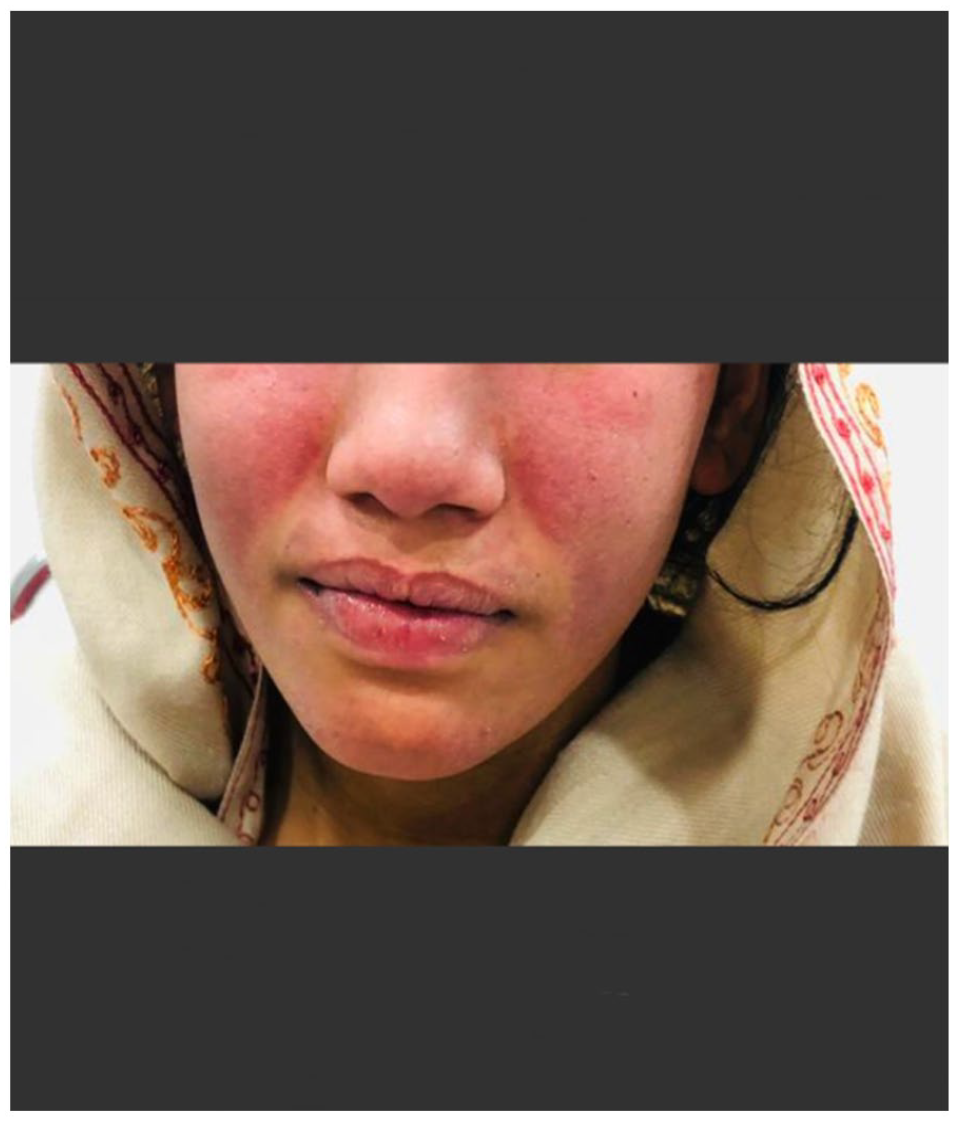
An erythematous rash involving the forehead, nasal bridge, and bilateral cheeks with sparing of nasolabial folds.
Palmar erythema and an erythematous violaceous, slightly scaling, densely set confluent papules with sparring of the articular regions were also noted on fingers, dorsum of the hand, and ventral and dorsal surfaces of both forearms (Figure 2).

(A) Palmar Erythema of both hands, (B) erythematous violaceous, slightly scaling, densely set confluent papules with sparring of the articular regions on the dorsum of hands, (C) ventral surface of the forearm, and (D) dorsal surface of the forearm.
Joint examinations revealed mild swelling of the dorsal and palmar aspects of the fingers affecting the metacarpophalangeal joints with sparing the interphalangeal joints. Periungual swelling was observed, and hyperpigmented patches were present on her knee joints with no grotton’s papules. Upon examination there was no lymphadenopathy or visceromegaly. The rest of the systemic examination was unremarkable. Laboratory evaluation revealed normocytic anemia, thrombocytopenia, and elevated erythrocyte sedimentation rate (ESR). Her immunological tests including ANA and other antibodies related to SLE were negative (Table 1).
Laboratory evaluation.

Abbreviations: µL, microliter; ALT/GTP, alanine aminotransferase/glutamic-pyruvic Transaminase; aPTT, Activated Partial Thromboplastin Clotting Time; CMV, cytomegalovirus; CRP, C- reactive protein; dsDNA, double stranded deoxy ribonucleic acid; EBV, Ebstien-barr virus; ESR, erythrocyte sedimentation rate; fL, femtoliter; g/dL, gram/deciliter; HCT, hematocrit; HCV: hepatitis C virus; HDL, high density lipoprotein; HIV, human immunodeficiency virus; INR, international normalised ratio; IU/L, international units per liter; LDL, low density lipoprotein; LDH, lactate dehydrogenase; MCH, mean corpuscular hemoglobin; MCV, mean corpuscular volume; mEq/L, milliequivalents per liter; mg l−1, milligrams per litre; mg/dL, milligram/deciliter; ng/dL, nanograms per deciliter; PCNA, proliferating cell nuclear antigen; pg, picogram; PT, Prothrombin time; Sm, smith; U/L, units per liter.
Peripheral blood smear showed normocytic normochromic anemia and urine analysis was unremarkable for hematuria, pyuria, proteinuria, and/or cellular casts, and her echocardiography revealed preserved left ventricular function with no valvular abnormalities. Skin biopsy was not performed due to lack of affordability. Liver and renal function tests and urinalysis were within normal limits. Chest X-ray and electrocardiography revealed no abnormality. Blood culture was negative for bacterial infection. Ophthalmologic examinations were also normal. Coombs test was negative. The patient was diagnosed with a case of ANA-negative SLE in accordance with ACR criteria 1997. Patient fulfilled 4 out of 11 characteristics, that is, malar rash, photosensitivity, arthritis and anemia. ACR criteria includes 11 features for diagnosis of SLE, that is, includes malar rash, discoid rash, photosensitivity, oral ulcer,arthritis,serositis, renal disease, neurologic disorder, hematologic disorders (anemia, leukopenia, thrombocytopenia, lymphopenia), immunologic disorder and ANA test positive. Four of the 11 features listed are necessary for a diagnosis. 11 She was given a tablet of prednisolone 5 mg two tablets TDS for one-month, topical fluticasone ointment (appropriate 10 g) twice daily for one month, a tablet of calcium and vitamin D for one month, a tablet of hydroxychloroquine 200 mg one tablet twice daily, tablet Naproxen 250 mg one tablet twice daily and capsule pantoprazole 40 mg once daily for one morning. At 4 week follow up the patient described marked improvement in the joint pain and photosensitivity the oral steroid therapy was tapered, and topical steroids, naproxen, and pantoprazole were stopped and she was continued with hydroxychloroquine. At 8 weeks the patient’s rash decreased in severity and he was continued with hydroxychloroquine for 6 months.
Discussion
Pediatric SLE is one of the most common autoimmune conditions affecting children with the peak incidence at the age of 12 years. The disease incidence before the age of 10 years is rare, and the condition is more common in female children as compared to males. The prognosis of pediatric SLE is not favorable in comparison to adult-onset SLE because of the prolonged course of the disease in children, early involvement of the multi-systems, and the side effects of systemic therapy. 8
Common laboratory findings in children with SLE include anemia and thrombocytopenia, decreased vitamin D level, and elevated Erythrocyte sedimentation rate (ESR). In addition, autoantibodies such as antinuclear antibodies (ANAs), double-stranded DNA (dsDNA) antibodies, antibodies to the extractable nuclear antigens (ENAs), and antiphospholipid antibodies (aPLs) are expected to present in the serum of children with SLE. 8
In most series, 100 percent of children with SLE are ANA positive. Occasional cases of “ANA-negative” SLE are described, although the concept is controversial, and an ANA-negative child should be vigorously evaluated for alternative diagnoses.8,9 Studies have suggested that a positive ANA may disappear in some SLE patients over time, with sensitivity dropping to 76% and positivity dropping from 98% to 71% in patients with established SLE. ANAs have a sensitivity of 33.6%, while anti-dsDNA has a sensitivity of 57.1%, indicating that a significant portion of SLE cases may be missed based on these markers alone. Sero-negativity in lupus patients may be due to technical failure or entrapment of ANA in circulating immune complexes yet patients exemplify similar clinical presentations to their ANA-positive counterparts. 9 Additionally, autoantibodies such as anti-dsDNA and anti-Smith (anti-Sm) help to confirm the diagnosis of SLE but are not uniformly present. All these antibodies may also be found in children who do not fulfill the classification criteria for SLE. Some of these children will go on to develop SLE, others will develop other rheumatic diseases, and some will remain asymptomatic. 10
SLE typically presents with a variety of complications, such as vascular, cardiac, nervous system, pulmonary, and renal involvement, as well as positive ANA and or patients with seronegative ANA tests have a higher prevalence of positive Ro factor antibody. However, there were no further systemic symptoms or the presence of these antibodies in our patient. Also, the lack of a biopsy made the diagnosis more challenging, although the patient still exhibited the typical clinical signs of SLE, including photosensitive maculopapular rash, arthralgia, joint pain, and scaly pruritic plaques over limbs. The diagnosis of SLE in our patient was made based on the ACR criteria. Our patient fulfilled 4 of 11 ANA-negative criteria. These include Malar rash, photosensitivity, arthralgia, and hematological evidence of anemia and thrombocytopenia.
Differential diagnosis of pediatric SLE includes infectious causes such as CMV, Brucella and parvovirus B19. These are characterized by disease specific clinical features as well as disease specific antibodies. Other differential diagnosis such as hematological malignancy (leukemia, lymphoma) and other autoimmune conditions such as Juvenile idiopathic arthritis (JIA) and juvenile dermatomyositis (JDM) are characterized by specific CBC profile and clinical features such as leukocytosis, positive Anti SM antibodies, antiphospholipid antibodies, and positive Ro factor, grotton’s papules and heliotrope rash with progressive muscle weakness. However none of these were present in our patient.
The diagnosis of SLE can be made by combining clinical and laboratory findings but there is no criterion available now for early identification of the disease. ACR published the first, preliminary, criteria for SLE in 1971, which were revised in 1982 and later validated. The second revision from 1997 (ACR-97), although unvalidated, has been the most widely used criteria set to date. The 1997 American College of Rheumatology (ACR) criteria and its complementary criteria; the 2012 systemic lupus international collaborating clinic (SLICC) criteria are designed for the classification of SLE but not for the diagnosis. 11 Children who fulfill the American College of Rheumatology (ACR) criteria, Systemic Lupus International Collaborating Clinics (SLICC) criteria, or 2019 European Alliance of Associations for Rheumatology (EULAR; formerly known as European League Against Rheumatism)/ACR criteria, are considered to have definite SLE. 8
There are several cases of juvenile seronegative SLE reported previously (Table 2)
Reported cases of ANA-negative SLE in the pediatric group.

It appears that ANA negative SLE is a subgroup of sle that has not received enough attention. Clinicians need to be aware that certain patients may have ANA test results that are consistently negative.
Conclusion
Seronegative pediatric SLE is a rare condition that manifests similarly to seropositive SLE. In the case of ANA-negative SLE, the typical clinical features may serve as diagnostic clues for the disease by the application of the ACR-97 criteria of SLE classification. If the patient fulfills the criteria for SLE despite seronegativity, the diagnosis should not be delayed. Early diagnosis, management, and screening for complications can improve the outcomes of the patient.
Footnotes
Acknowledgements
None
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Contributions
Qaisar Ali Khan and Tehmina Khan conceived the idea of the case report. Qaisar Ali Khan was responsible for data collection and acquisition of data. Parsa Abdi, Christopher Farkouh, Michelle Anthony, and Faiza Amatul performed the literature review and wrote the manuscript. Sumaira Iram, Qaisar Ali Khan, and Tehmina Khan reviewed and critically revised the manuscript. All authors have approved the final manuscript.
Informed Consent
Written informed consent was obtained from the patient’s father to publish this case report and any accompanying images.