
Abstract
Background:
Blue Rubber Bleb Nevus syndrome (BRBNS) is a rare disorder, that results in congenital cutaneous hemangiomas of the skin and gastrointestinal tract. Although asymptomatic, the nevi present as soft, non-mobile, dark blue, compressible papules. Clinically it presents as iron deficiency anemia due to occult gastrointestinal bleeding.
Case presentation:
A 22-year-old female patient presented with complaints of shortness of breath, fatigue, and palpitation for 2 months. On examination, she had a pale effect and widespread hemangiomas on her lips, hands, and feet. Laboratory results revealed iron deficiency anemia with hemoglobin (Hb) of 2.1 gm/dl and histopathology results of the hemangioma specimen showed angiokeratomas. Based on clinical manifestations and laboratory results, the patient was diagnosed with a case of BRBNS. The patient was transfused with red cell concentrate her symptoms improved but on the first follow-up visit her Hb again dropped to 8.6 mg/dl.
Conclusion:
A high suspicion of BRBNS diagnosis should be considered if a patient presents with iron deficiency anemia and multiple cutaneous hemangiomas. Further screening should be done to explore internal bleeding and hemangiomas.
Introduction
Blue Rubber Bleb Nevus syndrome (BRBNS) is characterized by hemangiomas and malformations in the venous system of the skin and visceral organs. 1 These malformations may be severe enough to cause hemorrhage and death. BRBNS manifests as button-like bluish papules at birth or early childhood with a predilection for the tongue, face, trunk, and extremities. 2 The gastrointestinal tract is a commonly affected area (occurring in 76% of cases), with multiple GI hemangiomas leading to friability and bleeding of the colon. 1 Iron-deficiency anemia, torsion, and intussusception are noted in the literature as rare complications of BRBNS. 1 The syndrome is aptly named due to its unique appearance of rubbery cutaneous lesions, which are soft, non-mobile, dark blue, compressible veins that become wrinkled when blood is elicited in the area. 2 Although most hemangiomas involute over the course of an individual’s lifetime, these nevi display no evidence of regression. In fact, analyses of these patients show further progression and recurrence of these cutaneous manifestations.3,4 Histopathologically, BRBNS is visualized as a cluster of dilated, irregular spaces abutted by a single layer of endothelial cells surrounded by various amounts of fibrous connective tissue. 1
Currently, as there is little research with only around 200 cases reported in the literature, there is no curative treatment.1,2 Physicians have attempted to utilize systemic steroids to diminish the rate of hemangioma growth in the intestinal tract, as well as biologic response modulators (such as interferon-alpha) to resolve resulting coagulopathies in these patients. 3
Herein, we present a case of BRBNS in a 22-year-old woman in critical condition who suffered from GI bleeding, nausea, and severe anemia for years. The patient underwent an emergency blood transfusion on the first day of hospitalization.
Case Presentation
A 22-year-old female presented to the emergency unit of a tertiary care hospital with complaints of shortness of breath, palpitations, and fatigue for 3 weeks. She had a history of multiple transfusions in the past and received her last transfusion 6 years ago. On examination, she had pale conjunctiva and widespread hemangiomas, namely on her lips, hands, and feet (Figure 1).

Venous malformations presenting as cutaneous cavernous hemangiomas of the lips (A), hands (B), and feet (C and D).
The patient had these lesions at birth, and she also noted that the lesions increased in size as well as in number over the past 6 years.
The vital signs of the patient on arrival were a blood pressure of 70/40 mmHg, a pulse of 100 beats per minute, oxygen saturation of 65% on room air, a temperature of 98.6°F, and a Glasgow coma scale of 13/15. The rest of the examination was unremarkable. She was resuscitated with intravenous fluids and baseline investigations were ordered (Table 1).
Initial investigations.
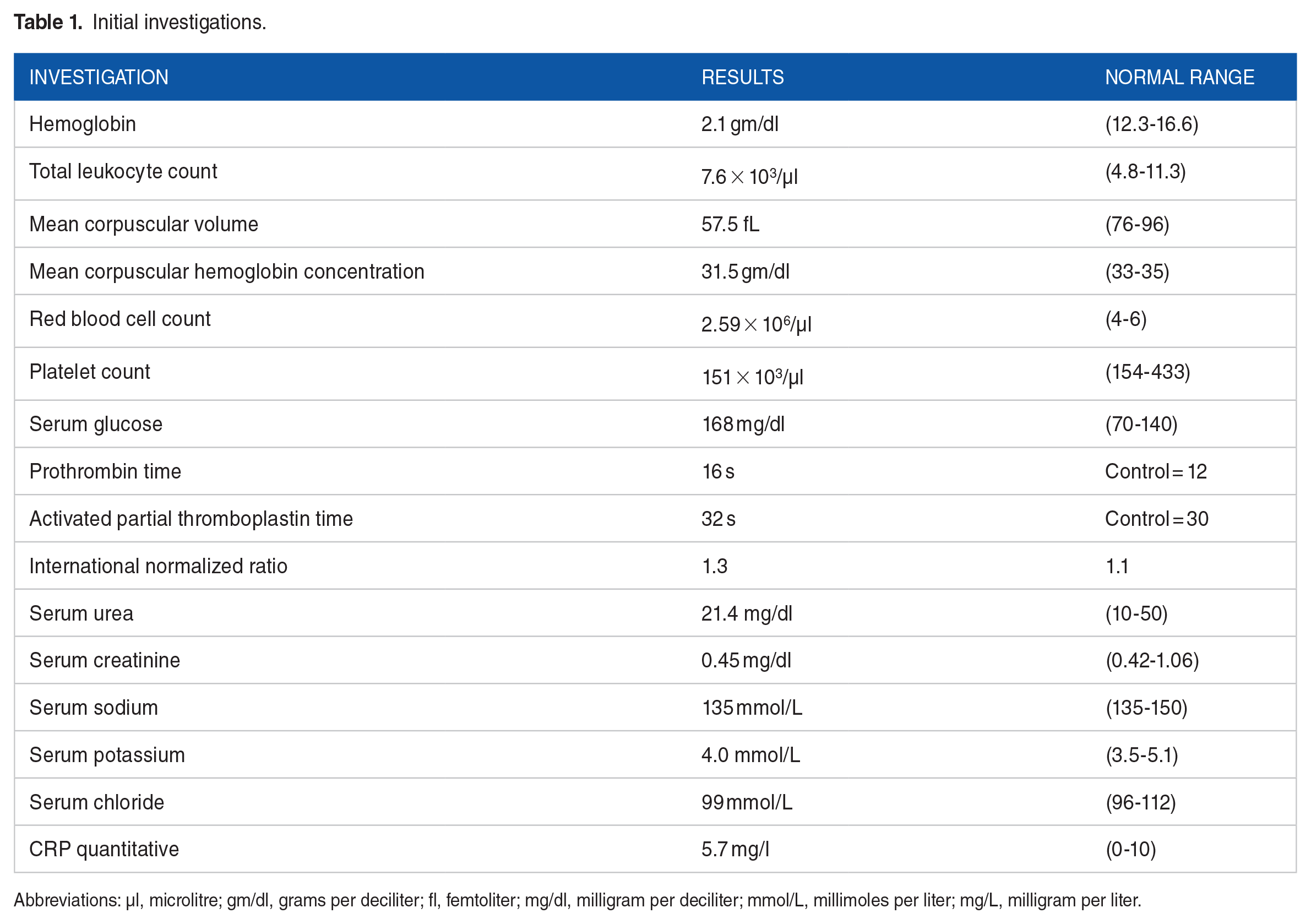
Abbreviations: µl, microlitre; gm/dl, grams per deciliter; fl, femtoliter; mg/dl, milligram per deciliter; mmol/L, millimoles per liter; mg/L, milligram per liter.
Further workup for anemia was initiated and a peripheral smear was sent, and the patient was started on a packed red blood cell transfusion. Her peripheral blood smear displayed hypochromic microcytic anemia prompting an endoscopic evaluation which displayed a vascular hemangioma-like lesion in the esophagus in addition to multiple vascular hemangioma-like lesions extending to the duodenum. On colonoscopy, several hemangioma-like lesions were noted in the colon up to the splenic flexure. Lastly, a colonic biopsy displayed an acute self-limited colitis.
On further investigation she had been following a balanced diet, having regular menstrual cycles, and she did not have any positive family history of blood disorders nor did her family have a history of similar condition. Additionally, a specimen was collected for skin biopsy from the hemangioma lesions which revealed angiokeratoma. Based on the clinical presentation and biopsy results, the patient was diagnosed with a case of blue rubber bleb nevus syndrome (BRBNS).
During her stay at the hospital, she received a total of 8 pnt of packed red cells, intravenous fluids, tranexamic acid, and vitamin K. On the 7th day of admission, the patient’s hemoglobin rose to 10.1 gm/dl, was vitally stable and was discharged home on tablet ferrous sulfate plus folic acid (525 mg/800 mcg). The patient was educated on her rare genetic syndrome, symptom management, the importance of genetic counseling, and was asked to follow up after 4 weeks. The patient was also made aware of the need for potential future surgeries as well as sclerotherapy to treat her lesions if her lesions worsen. Other treatment options were discussed for her cutaneous lesions such as on the first follow-up, the patient’s symptoms improved but her hemoglobin dropped to 8.6 mg/dl.
Discussion
A BRBNS diagnosis is very rare with an estimated prevalence of 1 in 14 000 births. 2 The hallmarks of the BRBNS are venous malformations presenting as cutaneous cavernous hemangiomas and gastrointestinal hemangiomas. 1 Subsets of cases have involved other organs such as the liver, heart, eyes, and central nervous system.5 -7 BRBNS is predominant in Caucasians and has no sex predominance. An autosomal familial history of chromosome 9p has been reported in 6 cases, although this could also be sporadic.8-10 Studies have reported somatic mutations in TIE2 and TEK as potential causes of BRBNS. 2
BRBNS presents with a unique presentation allowing for the syndrome to be diagnosed generally through a clinical examination. Multiple cutaneous lesions in BRBNS tend to appear early in life with a predominance for the trunk and upper limbs. 2 Clinical manifestations of BRBNS differ depending on the organ involved. It has been shown that the cutaneous lesions are asymptomatic with 5% of patients suffering from painful lesions and 2% complaining of hyperhidrosis.11,12 The cutaneous nevi are noted to be painful at night, preventing proper sleep habits, and can range from 1 to 10 mm in size.6,7 BRBNS can present as GI lesions and is the most common in the small intestine which increases the risk of bleeding. 2 Upper endoscopy, colonoscopy, and computed tomography barium studies have been employed to diagnose and visualize the extent of bleeding and treat active bleeds. The bleeding seen in BRBNS often leads to an iron deficiency that is associated with occult fecal bleeding, with hematochezia and melena rarely seen.6,7 Regarding BRBNS’s gastrointestinal lesions, there is also a predilection for the descending colon and rectum, making defecation painful. 13 Given a large amount of blood loss from the intestinal tract, transfusions of blood are commonly instituted. These transfusions, however, may lead to secondary complications such as iron overload or toxicity. 13 In rare cases, complications of BRBNS may include blood coagulation, thrombocytopenia, or disseminated intravascular coagulopathy. 14
The differential diagnosis of BRBNS includes glomangiomatosis, Osler-Weber-Rendu Syndrome (OWRS), Mafucci Syndrome, and Klippel-Trenaunay-Weber Syndrome. To distinguish BRBNS from glomangiomatosis, one must visualize both pathologies histologically as glomangiomatosis appears as numerous thin-walled blood vessels invested with abundant bland epithelioid cells with distinct cell membranes and large variably sized vessels whilst BRBNS presents as venous cavernous angiomas with clusters of dilated, irregular spaces.15,16 BRBNS is easily distinguished from OWRS by the typical appearance of OWRS’s hallmark nevus flammeus (port-wine-stain) patterns and its histological pattern of capillary hemangiomas.13,17-21 When distinguishing between BRBNS and Mafucci Syndrome, one must visualize Maffuci Syndrome with diffuse vascular malformations in both the skin and soft tissue in addition to bone malformations and chondrodysplasia in addition to vascular lesions in the gastrointestinal tract leading to the presence of venous malformation in the esophagus, stomach, duodenum, and ileum.22,23 Mafucci Syndrome is characterized grossly by enchondromas and bone deformities. Klippel Trenaunay-Weber syndrome has distinguishing factors of hemangiomas with hypertrophy of associated bone and soft tissue in addition to venous swellings in the involved extremities and arteriovenous malformations. Distinguishing factors between BRBNS, glomangiomatosis, OWRS, Maffuci, and Klippel Trenaunay Weber Syndrome are listed in Table 2.
Distinguishing factors between BRBNS, glomangiomatosis, Osler-Weber-Rendu Syndrome, Mafucci Syndrome, and Klippel Trenaunay-Weber Syndrome.

Conclusions
A high suspicion of BRBNS should be considered if a patient presents with multiple hemangiomatous lesions on the skin and iron deficiency anemia. Early screening for internal mucosal bleeding is needed to prevent further complications. Treatment must be patient-centered and includes conservative management, medical treatment, and various surgical options available to minimize intestinal loss and internal bleeding.
Footnotes
Acknowledgements
None.
Correction (May 2024):
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Q.A.K, A.K, and Z.U conceived the idea, Q.A.K evaluated the patient, Q.A.K and A.K were responsible for data collection and acquisition of data, C.F, P.A, M.A, E.K, F.A, and S.P did the literature review and wrote the manuscript. Q.A.K. and C.F. reviewed and critically revised the manuscript. All authors have approved the final manuscript.
Ethical Approval
Not required.
Registration Number
Not applicable.
Guarantor
Dr. Qaisar Ali Khan.
Consent
Written informed consent was obtained from the patient to publish this case report and any accompanying images. Consent can be provided upon Editor’s request.
Provenance and Peer Review
Externally peer-reviewed, not commissioned.