
Abstract
Introduction:
Cerebral venous sinus thrombosis (CVST) is a rare but highly fatal neurological condition mostly caused by prothrombotic conditions like antiphospholipid syndrome, factor V Leiden, and G20210A prothrombin polymorphism. Snake bites are a rare cause of cerebral venous sinus thrombosis that must be recognized and treated promptly to improve survival.
Case presentation:
We present a case of a 25-year-old male who developed headaches and seizures following a Viper snake bite. The diagnosis was made based on a magnetic resonance venogram (MRV) showing transverse sinus thrombosis with sigmoid sinus stenosis. Initially, the patient was treated with antivenom and supportive treatment for disseminated intravascular coagulation (DIC). After the diagnosis of CVST, the patient was treated with rivaroxaban and levetiracetam. The patient improved within 1 week of treatment and was advised to follow up in 3 months.
Conclusion:
A high index of suspicion for cerebral venous sinus thrombosis is required if the patient presents with headaches, seizures, or abnormal vision following a snake bite. Early diagnosis and management can prevent further neurological damage.
Introduction
Snake bites are a dangerous incidence afflicting thousands of individuals in rural areas of tropical nation’s leading to the World Health Organization (WHO) labeling snake bites as a neglected tropical disease in 2009. 1 Snake bites from venomous species can cause various symptoms, including superficial puncture wounds with associated pain and swelling, nausea with vomiting, dizziness, and dyspnea. 2 If snake bites are to go untreated, hemorrhagic blisters, cellulitis, and necrotizing fasciitis can result, potentially even leading to life-threatening complications such as shock, and coagulopathy.2,3 Cerebral venous sinus thrombosis (CVST) is an uncommon and deadly condition characterized by non-specific clinical symptoms such as headaches and nausea, creating difficulty in an accurate diagnosis. Autopsy studies indicate that CVST incidence is approximately 3 to 4 cases per million, with a 3:1 female-to-male ratio. 4 Aside from a female predominance, CVST is also known to affect children and young adults in developing countries. The dural venous sinuses, transverse, and superior sagittal sinuses are mostly involved in thrombosis.1 -6 CVST is subdivided into 3 subtypes based on the individual’s onset of symptoms: acute CVST is used to describe symptom onset for 48 hours or less; subacute CVST is for when symptoms have been present for at least 48 hours but less than 1 month; and chronic CVST for when symptoms have been present for longer than 1 month. Subacute CVST accounts for most cases of CVST, whilst chronic CVST is reported to be the least common. Imaging advancements have made it possible to detect CVST at an earlier stage, increasing its incidence. This early detection is crucial for treating CVST and has led to increasing survival rates. 6
Any prothrombotic condition that causes vessel wall injury and subsequent hypercoagulability due to blood stasis increase the risk of CVST. 4 The most frequent risk factor includes antiphospholipid syndrome, factor V Leiden, and G20210A prothrombin polymorphism. 4 Other conditions predisposing to cerebral venous sinus thrombosis are hereditary thrombophilia, birth control, pregnancy, head and neck infections, vasculitis, cancer, dehydration, and obesity. 5 The pathophysiological of CVST is poorly understood. Still, it is proposed that thrombosis leads to increased intracranial pressure, which leads to a cascade involving cytotoxic and vasogenic edema, parenchymal hemorrhage, and hemorrhagic infarction. 4
The common presenting symptoms of cerebral venous sinus thrombosis include signs of increased intracranial pressure, including headache, papilledema, abnormal vision, focal neurological deficits, and seizures.4,5 Headache is a prominent symptom seen in 80% of patients with CVST. Motor weakness is a commonly observed neurological deficit. Seizures are primarily observed in patients with acute CVST presenting with focal neurological deficits. CVST can manifest in unusual ways, including recurrent falls, weakness, tingling, numbness, and cognitive impairment without any positive neurological findings. 6 The gold standard for diagnosis of CVST is imaging with non-contrast computed tomography (CT) of the head recommended as the initial technique. 4 Snake-bite-induced cerebral venous sinus thrombosis is rare and has not been well reported in the literature.4,5 Here, we report a case of a 25-year-old male farmer who presented with CVST 1 day after a snake bite.
Case Report
A 25-year-old male presented to the emergency room reporting having been bitten by a Viper snake on his left leg 1 day ago. He was unable to identify the species of the snake when prompted but noted severe left leg pain associated with swelling of the leg shortly afterward. He received his initial management of wound cleaning in the form of washing the wound with tape water and injection ketorolac for pain local basic health unit and the patient was advised against the movement while shifting to the tertiary care hospital for further management. On arrival, the patient was in shock with the vital signs, blood pressure of 90/60 mm of Hg, pulse rate of 118 beats per minute, respiratory rate of 25 breaths per minute, and oxygen saturation of 93%. The patient also had 3 episodes of hematemesis and a complaint of diplopia. Initial laboratory investigations were sent, and the patient was resuscitated in the emergency department, and he received three 10-mL polyvalent anti-snake venom, an injection of ceftriaxone 2 g, and tetanus toxoid. On examination, the left leg was found to have superficial puncture wounds consistent with fang marks just above the ankle, swelling (2 cm greater than the right leg), and bruises at the site of the cannula. The rest of the neurological examination was normal. Initial lab results displayed elevated international normalized ratios (INR), bilirubin, D-dimers, leukocytes, and thrombocytopenia (Table 1). The patient was admitted to the medical unit and treated as a case of disseminated intravascular coagulation. On the first day of his admission to the hospital, his left leg swelling increased and extended to the mid-thigh. Shortly afterward, he developed a severe headache and had 2 episodes of a generalized tonic-clonic seizure. From a clinical standpoint, he improved significantly, as shown by the improvement from initial labs (Table 1). A doppler ultrasound of the left lower limb excluded venous thrombosis. His magnetic resonance imaging (MRI) did not reveal any abnormalities while his magnetic resonance venogram (MRV) showed transverse sinus thrombosis with sigmoid sinus stenosis (Figure 1) and (Figure 2). Further workup for thrombophilia and secondary causes of hypercoagulability revealed no abnormalities (Table 2). He was started on tablet rivaroxaban (initially 15 mg twice daily for 3 weeks then 20 mg once daily) and tablet levetiracetam (500 mg twice daily). The patient’s was advised to follow up with MRV after 3 months. The patient has one seizure episode after 2 months of treatment due to noncompliance with the antiepileptics and was advised to take the same treatment same treatment for the next 3 months. The patient failed to follow up after 2 months, and a follow up MRV was not done which was planned at 12 weeks.
Initial laboratory investigations.

Abbreviations: PT, prothrombin time; aPTT, activated partial thromboplastin time; INR, international normalized ratio; mg/dL, milligram per deciliter; g/dL, gram per deciliter; ng/mL, nanogram per milliliter; µL, microliter.

Magnetic Resonance Imaging (MRI) of the brain showing normal brain with no evidence of stenosis or thrombosis.
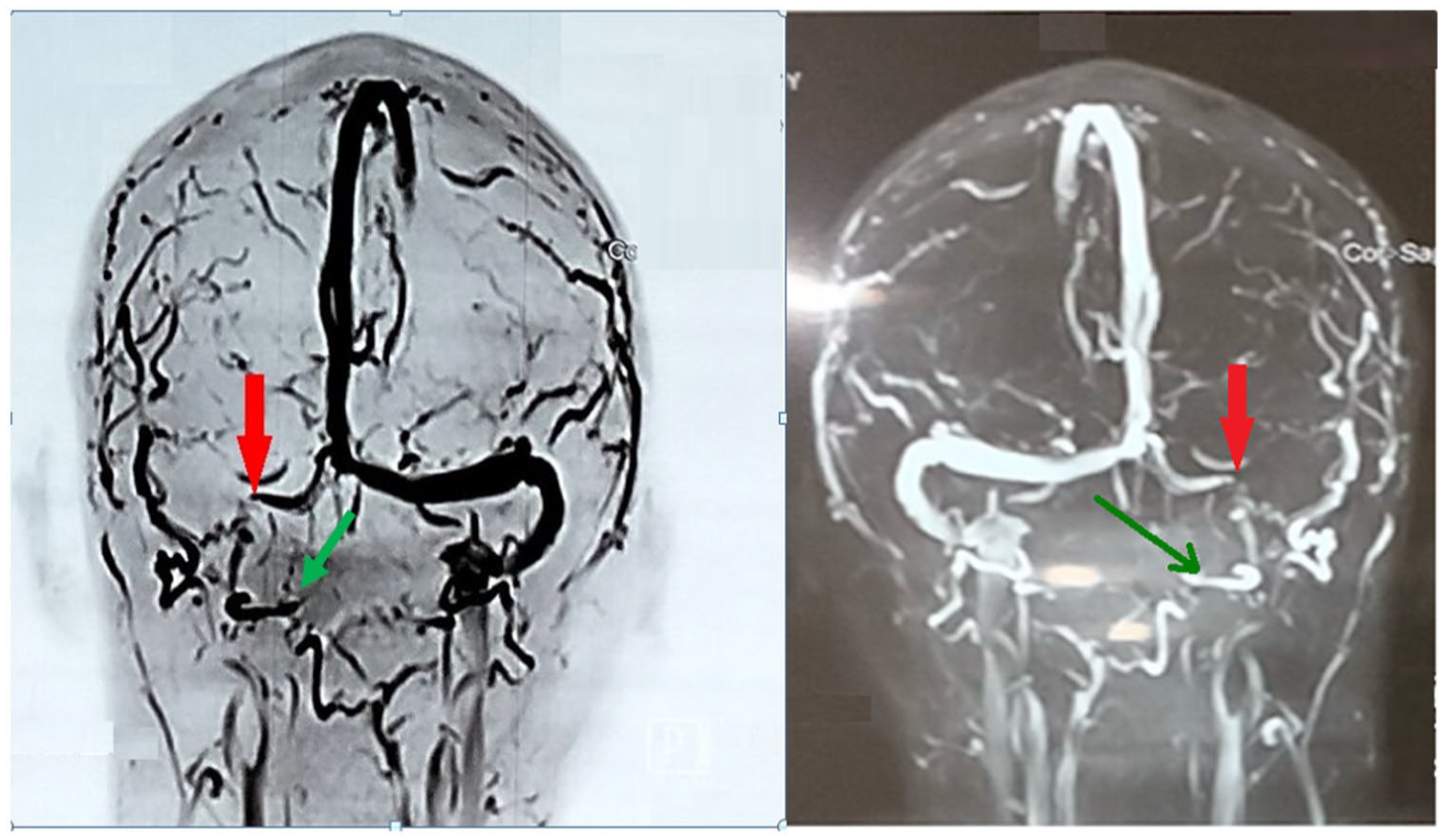
Magnetic resonance venogram (MRV) showing transverse sinus thrombosis (Red arrow) and sigmoid sinus stenosis (Green arrow).
Thrombophilia screen.

Discussion
It is critical for early recognition of thrombosis of the venous sinuses of the brain despite its rarity, as intervention can have a significant impact on mortality. 7 A wide range of cerebral venous sinuses can be affected, but the most affected sinuses are the transverse sinuses and superior sigmoid sinuses. 4 Cerebral venous sinus thrombosis can present as headache, seizures, focal neurological deficit, cranial nerve syndromes, visual abnormalities, or pseudotumor cerebri-like syndrome. 4 A long list exists of causes and risk factors associated with cerebral venous sinus thrombosis, including, but not limited to, inherited and acquired thrombotic state, infections, inflammatory diseases, hematological conditions, and certain pharmacological drugs. Inherited thrombotic conditions are the most common causes in developed countries 4 whereas snake bites are a rare cause of cerebral venous sinus thrombosis.4,5 The summary of similar cases with same conclusion has been evident from literature search as shown in Table 3
Summary of the literature search.

Snake bites are a common yet neglected trauma prevalent in tropical countries such as India and Pakistan. Unfortunately, it can cause significant mortality and morbidity with several complications following a snake bite, including thrombosis. 12 Arterial thrombosis following a snake bite is a widely encountered and studied complication of snake bites, while venous thrombosis is rare and less commonly encountered. The mechanism for snake bite-induced venous sinus thrombosis is direct endothelial injury, stasis, or hypercoagulability, best described by Virchow’s triad.12 -15
In this report, we observe a case of snake bite in a young male patient whose initial presentation was concerning due to disseminated intravascular coagulation. However, he developed a headache and generalized tonic-clonic seizures throughout his treatment which was concerning for an accompanying neurological condition. MRI and MRV, the gold standard of diagnosis of CVST, revealed transverse sinus thrombosis, an uncommon and rare presentation of a snake bite.16 -19 Cerebral venous sinus thrombosis usually manifests with headache, visual abnormalities, and seizures.16,17 Non-contrast CT can visualize a thrombus as a dense clot and string or cord sign and can also visualize accompanying cerebral edema and intracranial hemorrhage. 4 Prompt treatment is necessary with anticoagulation and rarely with endovascular procedures; otherwise, it can result in disability and death. Acute CVST has a mortality rate of 5.6%.4,17
Given the above case report, a snake bite can present with cerebral venous sinus thrombosis. Hence a high index of suspicion should be kept if the patient develops a headache, seizures, or abnormal vision.
Conclusion
The risk of cerebral venous sinus thrombosis following a snake bite is relatively low. If diagnosed and treated early, it has a good prognosis, but if left untreated, it can significantly impact morbidity and mortality. As such, headaches, seizures, or abnormal vision after a snake bite should raise a high index of suspicion for CVST.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.