
Abstract
Recurrent vulvovaginal candidiasis (RVVC) affects millions of women worldwide, severely impairing their quality of life. Despite the existence of multiple induction and maintenance therapeutic strategies, mainly based on antifungals, relapse rates are still high. Palomacare® is a vaginal gel containing, among others, hyaluronic acid and Centella asiatica, with repairing and moisturizing properties. A series of 5 clinical cases showed that symptoms improved and even disappeared in women with RVVC receiving Palomacare®. None of the patients experienced recurrence after the treatment, having their vaginal health restored, suggesting that the non-hormonal Centella asiatica, hyaluronic acid and prebiotic-based gel is effective for preventing RVVC relapse in women of reproductive age.
Introduction
Vulvovaginal candidiasis (VVC) is a symptomatic inflammation of the vagina (vaginitis) frequently involving the vulva and caused by Candida yeast infection. 1 It is characterized by vulvar erythema, excoriation, pruritus, and an abnormal vaginal discharge, which can be “cheese-like” or watery. 2 Differential diagnosis from other forms of vaginitis requires the observation of yeast on microscopy of vaginal fluid. 1 It is estimated that around 75% of women develop VVC at least once in their lifetime. 3 Although most of them experience at most 2 episodes per year, others suffer multiple annual recurrence. 2 Recurrent VVC (RVVC) is defined as 4 or more episodes of VVC within a year and 5% to 8% of adult women endure it during their reproductive period.1,4,5 It affects approximately 138 000 000 women worldwide annually and 492 000 000 over their lifetimes, with a higher prevalence in the group age of 25 to 34 years.3,6
Besides pruritus, soreness and discomfort, women with RVVC frequently present with loss of self-esteem and confidence, inability to carry on with their normal physical activities, along with difficulties with their sexual life and intimate relationships. 3 Overall, RVVC is a debilitating, long-term condition greatly associated with stress which may severely alter the quality of life of affected women.3,7 Several factors such as the use of contraceptives or antibiotics, immunodeficiency, mechanical irritation of vulvovaginal area, sexual transmission, commercially available solutions for cleansing of external genitalia or vaginal douching, or inadequate treatment have been linked to RVVC. Additionally, diabetes mellitus is also considered a predisposing factor for RVVC, with its type, severity and degree of glucose control considered as potential risk factors.8,9 Hyperglycemia enhances the ability of Candida albicans, the most commonly identified species in patients with VVC, to bind to vaginal epithelial cells. 8 Besides Candida albicans, there are cases of VVC and RVVC due to non albicans Candida (NAC), where other species such as Candida glabrata, identified in around 10% to 20% of cases, or less frequent ones are present.10,11 Of note, many of these NAC species are identified more often in complicated VVC and are resistant to conventional treatment.10,12
In fact, the frequency of azole antifungal resistance is increasing in both Candida albicans and NAC species, mainly due to increased azole therapy exposure. 13 There are numerous strategies for treating RVVC and yet the relapse rates remain high. 14 Palomacare® (Procare Health Spain SL, Barcelona, Spain; CE marking #1849/MDD) is a vaginal gel composed of hyaluronic acid (HA) and beta-glucan niosomes, Centella asiatica fytosomes, α-glucan oligosaccharide (BioEcolia®), and Aloe vera extracts. Besides vaginal dysbiosis, this product might be used for treating nonspecific vulvovaginitis, cervicitis, genitourinary syndrome, vulvovaginal atrophy, during peripartum and post-chemotherapy/radiotherapy, and post-laser treatment. We present 5 case studies of women with RVVC treated with this non-hormonal Centella asiatica, hyaluronic acid and prebiotic-based vaginal gel. As it is usually done in routine clinical practice, adverse events were monitored during medical consultations through direct questions addressed to the patients. To ensure anonymity, patient-specific information was deidentified; therefore, patient consent was not required.
Case 1
This case describes a 36-year-old woman who developed RVVC (8 episodes of VVC during the last 6 months) after intensive antibiotic treatment due to a urinary infection. Throughout that period, the patient was treated with 5 different therapeutic strategies that included vaginal ovuli and creams, and oral treatment, even with probiotics. The patient experienced an initial improvement in all episodes, but recurrence always appeared around day 15. She felt very frustrated due to the limitations it implied in her daily life. Physical examination showed vulvar erythema with white discharge impregnation. Speculoscopy revealed macroscopically erythematous vagina and cervix, together with abundant whitish lumpy leukorrhea attached to the walls that was consistent with candidiasis. The most probable diagnosis was mycotic vulvovaginitis. Vaginal culture presented a large growth of Candida albicans. Treatment with Palomacare® was prescribed as follows: one daily vulvovaginal application for 6 days and one application every other day during the subsequent 3 weeks. Also, a daily application for 6 days post-menstruation for 6 months was indicated. Follow-up was performed after 15 days, 1 month, and 6 months through a clinical and vaginal culture evaluation. The patient was asymptomatic at all visits and microbiology results were all negative.
Case 2
In October 2021, a 28-year-old woman attended a medical appointment due to leukorrhea, pruritus, and vulvar and vaginal irritation for the third time in 9 months. This time, she also experienced dyspareunia during sporadic sexual intercourse (SI). The patient had been previously treated with several rounds of antifungals and probiotics. She was nulliparous, had no stable relationship, and had undergone an appendectomy at 9 years old. The symptoms, which had started in January 2021, improved with antifungal therapy but recurrence appeared usually after subsequent menstrual cycles. Vulvovaginal erythema was observed during physical examination, as well as a marked lumpy whitish leukorrhea consistent with VVC (Figure 1A). A vaginal culture performed in August 2021 stated the presence of Candida albicans. A single 600 mg dose of antifungal vaginal suppository was prescribed along with the vaginal gel once daily for a week, followed by every other day application thereupon. After 2 months, the patient reported having kept using Palomacare® monthly after menstruation since she noticed a considerable symptom improvement. Currently, the patient remains asymptomatic, even when having SI, and shows no signs of candidiasis (Figure 1B).
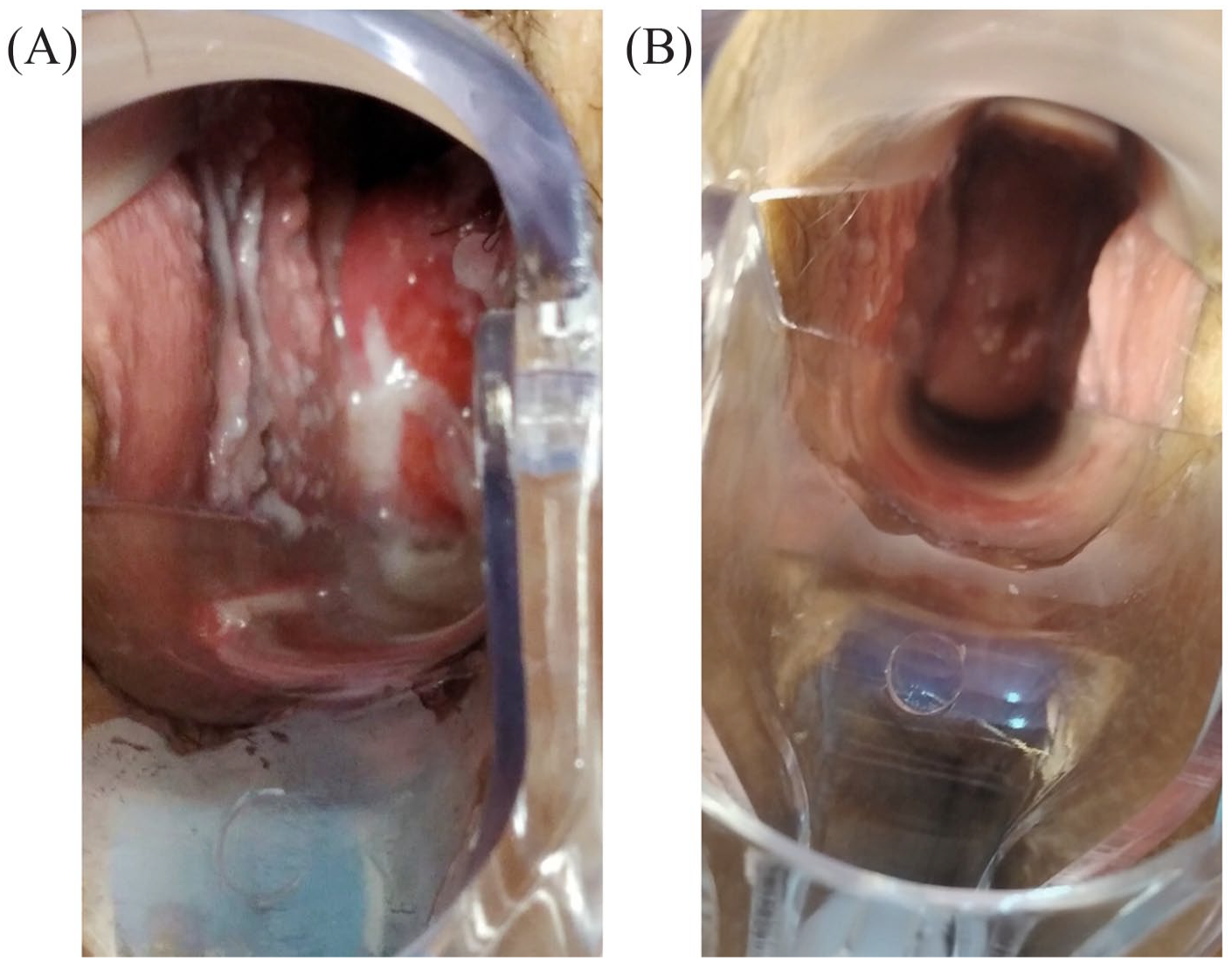
Macroscopical appearance of vulvovaginal tissue during speculoscopy from case 2 patient (A) before and (B) after treatment with the non-hormonal Centella asiatica, hyaluronic acid and prebiotic-based vaginal gel.
Case 3
The 35-year-old woman depicted here underwent normal vaginal delivery at 32 years old and presented normal menstrual cycles. During the previous year, the patient went to the doctor 6 times referring vulvovaginal pruritus and whitish lumpy leukorrhea that was not malodorous. The first episode started after taking amoxicillin with clavulanic acid to treat an acute tonsillitis. Also, the patient was going through a stressful period. Despite all VVC episodes being treated with local or oral antifungals, symptoms kept reappearing after a while, affecting her quality of life. External genitalia and vagina were erythematous and slightly edematous and were accompanied by candidiasis-looking lumpy leukorrhea. Vaginal discharge showed Candida albicans presence in every VVC episode. A fungigram performed during the last recurrence showed azole sensibility. The patient was then prescribed a 6-month episodic therapy consisting in 150 mg oral fluconazole weekly, together with the application of Palomacare® daily for 6 days after menstruation. Since that treatment was initiated, the patient did not present any other candidiasis episode and remained asymptomatic after finishing the therapy until now.
Case 4
A 28-year-old female complained about recurrent episodes of vaginitis caused by Candida the past months despite various medical oral and vaginal treatments. The patient had been using oral contraceptives for 3 years, those being well tolerated. Physical exam showed a swollen erythematous vulva and a vaginal fluid consistent with Candida (Figure 2A). Cervical-vaginal cytology and vaginal culture confirmed VVC diagnosis. Treatment was prescribed as follows: 150 mg oral fluconazole once a week for 4 weeks then once a month for 4 months, together with weekly 500 mg vaginal clotrimazole for 14 days and topical clotrimazole twice a day for 14 days. Afterward, non-hormonal Centella asiatica, hyaluronic acid and prebiotic-based vaginal gel therapy was established once per night for 6 days followed by twice a week for 6 weeks. Four months later, the patient reported a marked improvement of her symptoms along with a normal vaginal discharge and culture (Figure 2B).

Macroscopical appearance of vulvovaginal tissue during speculoscopy from case 4 patient (A) before and (B) after treatment with the non-hormonal Centella asiatica, hyaluronic acid and prebiotic-based vaginal gel.
Case 5
A 26-year-old female with diabetes initiated at 23 years old developed RVVC after starting to have SI with a new partner following 2 years of sexual inactivity. She presented a marked vulvar erythema and whitish thick leukorrhea. Response to topical antifungal treatment was poor. Therefore, the vaginal gel was added to her therapy: for 8 weeks she used 150 mg of fluconazole once a week together with constant Palomacare® application during 3 menstrual cycles. The patient presented a satisfactory evolution and remains asymptomatic.
Clinical Overview
RVVC is a condition that affects millions of women of reproductive age around the world causing non-negligible impairments in quality of life. Despite the use of antifungals for induction and maintenance therapy following the clinical guidelines, the relapse rates remain quite high (approximately 30%-60% of patients experience relapse after 12 months) and resistance to current therapy is increasing.13,14 Therefore, there is a need for treatments capable of reducing those rates.
The only guideline that suggests a therapy beyond antifungal therapy is the International Union against Sexually Transmitted Infections and the World Health Organization (IUSTI/WHO) which, as general advice, includes the application and wash off with vulval moisturizer to dry skin as a soap. 15 Oral probiotics and lactoferrin have also been linked to a reduction in recurrence. 16 Beta-glucan, 17 Centella asiatica, 18 and Aloe vera 19 are known moisturizers. Moreover, asiaticoside, an active component of Centella asiatica, and Aloe vera promote skin wound healing.20 -23 Besides tissue hydration, 24 HA has an anti-Candida activity shown to be dose-dependent, with all the tested Candida strains in the study being susceptible to HA, some even to the lowest dose used (0.25 mg/mL). 25
Consistent with the aforementioned findings, the case reports demonstrate that Palomacare® has a beneficial effect on RVVC. In cases 2, 3, 4, and 5 the treatment was concomitant with antifungals whereas the patient in case 1 was treated exclusively with Palomacare®. In all the cases, the use of the vaginal gel produced symptom improvement and in cases 1, 2, 3, and 5 patients were asymptomatic after the treatment. The marked improvement in symptoms reported in case 4 was accompanied by normal vaginal discharge and culture that reflected the potential vaginal health restorative properties of Palomacare®. The non-hormonal Centella asiatica, hyaluronic acid and prebiotic-based gel treatment in case 1 was maintained for 6 months and the patient remained asymptomatic, which implies that the regimen used for maintained prophylaxis, that is, application for 6 days post-menstruation each cycle, was suitable to avoid relapses. The same regimen was indicated for case 3 patient, along with oral antifungals, suggesting it is an appropriate therapy for RVVC. Moreover, the cases of RVVC here presented appeared in different circumstances (eg, stress, diabetes, antibiotic treatment, SI, nulliparous or not) in women with ages ranging from 26 to 36 years old and Palomacare® showed effectiveness invariably. These results are in accordance with a previous clinical study from Palacios et al. that showed a cytology normalization and an improvement in colposcopic epithelization after treatment with the non-hormonal Centella asiatica, hyaluronic acid and prebiotic-based vaginal gel in women with nonspecific vaginitis. 26 Finally, the Satisvag survey showed that Palomacare® is well tolerated and has a comfortable application, with a 98% of patients reporting good or excellent overall satisfaction with the vaginal gel. 27 In line with those results, our patients used the product as prescribed, even for a long 6 month-period in cases 1 and 3, and the woman from case 2 kept using it beyond the prescribed period.
Conclusion
The featured case studies showed that using the non-hormonal Centella asiatica, hyaluronic acid and prebiotic-based vaginal gel helped avoid VVC relapses in women that had previously been treated with several rounds of other therapies. This efficacy might be due to the repairing, moisturizing and anti-Candida properties of its components, mainly HA. After treatment with Palomacare®, patients managed to become asymptomatic and had their vaginal health restored, resulting in a marked improvement in quality of life. As case studies are not enough to justify a change in clinical practice, randomized controlled trials to evaluate the efficacy of Palomacare® versus current therapy with azoles in VVC and RVVC are needed.
Learning Points
Relapse rates of VVC remain quite high and resistance to current therapy is increasing despite the use of antifungals according to clinical guidelines.
Palomacare® is a non-hormonal vaginal gel composed of hyaluronic acid and beta-glucan niosomes, Centella asiatica fytosomes, α-glucan oligosaccharide (BioEcolia®), and Aloe vera extracts.
Adding Palomacare® to the standard of care for VVC can be useful to prevent recurrences in women prone to them.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
M.A., J.C.M.P., M.E., M.S., M.G.M., G.A.B., and P.L. participated in the methodology, data collection and analysis, investigation process, and review of the manuscript. J.C. was involved in the methodology, supervision, writing, and review of the manuscript.