
Abstract
Background:
The current literature focuses on the risk of infective endocarditis (IE) following transcatheter aortic valve implantation (TAVI). However, the risk of IE in patients waiting for TAVI is not well-studied. We present a unique case of a patient waiting for TAVI with decompensated heart failure who was found to have a large mitral vegetation, and consider risk factors for the development of IE in this population.
Case description:
We report the case of an 85-year-old male with severe aortic stenosis and recurrent small bowel angiodysplasias, requiring frequent blood transfusions and intravenous iron. He presented to a peripheral hospital in decompensated heart failure. Transfer was arranged to our center to expedite TAVI, under the premise that worsening aortic stenosis precipitated his decompensated state. Prior to TAVI, an echocardiogram was done, and demonstrated a 30 × 18 mm mass on the mitral valve with anterior leaflet perforation and severe mitral regurgitation. The findings were consistent with IE, and the TAVI was cancelled. Despite antibiotic therapy, the patient unfortunately deteriorated and palliative care was provided.
Conclusions:
This case highlights the need for further research regarding the risk of IE in patients waiting for TAVI. Current literature focuses on the development and management of IE following TAVI. Clinicians must understand that TAVI candidates have multiple risk factors for IE, including valvular disease, age, and comorbidities. IE should be considered as a possible cause for decompensated heart failure in patients awaiting TAVI.
Introduction
Infective endocarditis (IE) is associated with significant morbidity and mortality. 1 The presence of foreign material, such as a prosthetic valve, complicates the management of IE. A large multicenter registry examined outcomes in patients with IE following transcatheter aortic valve implantation (TAVI), and found an in-hospital mortality rate of 47.2% and a 1-year mortality rate of 66%. 2 Accordingly, current guidelines focus recommendations on patients with prosthetic material in situ, such as indications for antibiotic prophylaxis and the management of prosthetic valve IE. 3 However, there is a paucity of literature regarding the risk of IE in patients waiting for valve surgery. In accordance with the CARE reporting checklist, we present the case of a patient with severe aortic stenosis waiting for TAVI who was unexpectedly diagnosed with mitral valve endocarditis.
Case Presentation
History of presenting illness
An 85-year-old male was initially evaluated as an outpatient for aortic stenosis. His echocardiogram demonstrated a valve area of 0.8 cm2, mean gradient of 47 mmHg, peak gradient of 91 mmHg and aortic valve peak velocity of 4.76 m/s, in keeping with severe aortic stenosis. Mild mitral regurgitation and moderate mitral stenosis with significant mitral annular calcification were also demonstrated.
He endorsed shortness of breath on exertion, and was limited to slowly walking 100 m with a walker. This was also in the context of chronic anemia, with a baseline hemoglobin around 7.0 g/dL (normal 13.5-17.5). He was dependent on red blood cell transfusions twice per month, and a monthly course of intravenous (IV) iron sucrose. Previous upper endoscopies revealed recurrent angiodysplasias in the distal duodenum and proximal jejunum, which required clipping. In the context of severe aortic stenosis, this was suspicious for Heyde syndrome.
Intervention for his aortic stenosis was indicated given his New York Heart Association class II-III symptoms. Considering his age and comorbidities, he underwent evaluation for TAVI, and was deemed to be a candidate.
While awaiting TAVI, he presented to the emergency department (ED) at a peripheral hospital with orthopnea (Table 1). Initial vitals included a blood pressure of 113/54 mmHg, heart rate of 93 bpm, respiratory rate of 18 breaths per minute, oxygen saturation of 95% on 2 L/min, and temperature of 35.1°C. On auscultation, there was a late-peaking systolic murmur over the aortic area radiating into the carotid with an absent S2. He had bibasilar crackles and 2+ pitting edema bilaterally.
Timeline of events.
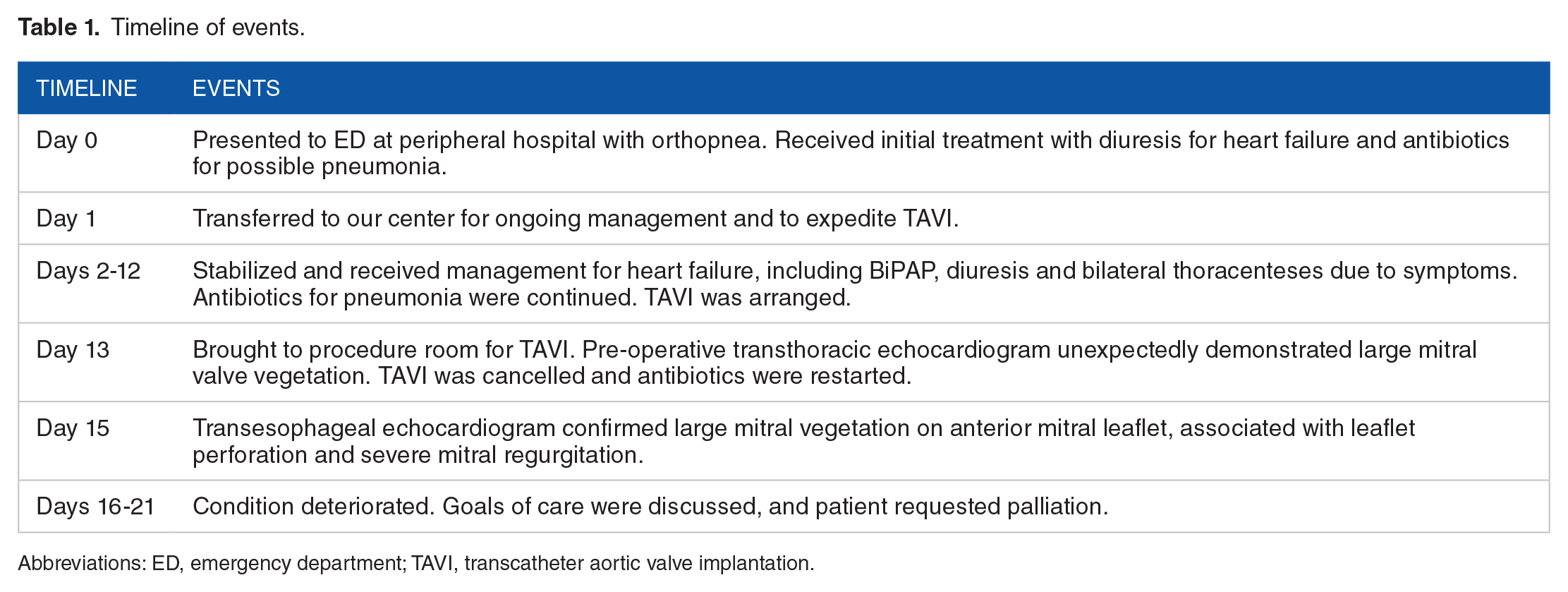
Abbreviations: ED, emergency department; TAVI, transcatheter aortic valve implantation.
Past medical history
In addition to severe aortic stenosis and recurrent small bowel angiodysplasias, the patient was also known to have hypertension, type 2 diabetes mellitus, peripheral vascular disease, and a prior laparoscopic low anterior resection for a sigmoid adenocarcinoma.
Differential diagnosis
The patient’s presentation was consistent with a heart failure exacerbation. The differential for his state of decompensation included valvular (eg, worsening aortic stenosis), infectious (eg, bacterial pneumonia, COVID-19) and ischemic triggers.
Investigations
Bloodwork revealed an elevated white blood cell count of 15.2 × 109/L (normal 4.0-11.0) and a low hemoglobin at 9.9 g/dL. Of note, the patient received 2 units of packed red blood cells the day prior. Troponin was elevated at 1.610 µg/L (normal < 0.012). COVID-19 nasopharyngeal swab was negative. Chest X-ray showed patchy bilateral opacities emanating from the mediastinum and moderate bilateral pleural effusions, in keeping with pulmonary edema. ECG showed sinus rhythm at 92 beats per minute, an incomplete left bundle branch block and left ventricular hypertrophy. There were no acute ischemic changes.
Management
The leading diagnosis was decompensated heart failure secondary to progression of aortic stenosis. The patient was admitted to hospital and diuresis was initiated. Overnight, he had worsening oxygen requirements and was placed on bilevel airway pressure (BiPAP). Given the mild leukocytosis, ceftriaxone and azithromycin were started for possible community-acquired pneumonia. Transfer to our center was arranged for ongoing management and to expedite his TAVI.
At our center, BiPAP, diuresis and antibiotics were continued. In the context of significant orthopnea, both pleural effusions were drained and analyses were in keeping with a transudative process—his known heart failure.
The patient’s condition stabilized, and a TAVI was arranged. In the procedure room, a pre-operative transthoracic echocardiogram was done, which unexpectedly demonstrated a large mass on the mitral valve. The TAVI was cancelled, and a transesophageal echocardiogram was arranged for further evaluation. It confirmed a 30 × 18 mm mass of the anterior mitral valve leaflet (Supplemental Video 1), associated with leaflet perforation and severe mitral regurgitation (Supplemental Video 2). Blood cultures were drawn given the concern for IE, but were negative. Importantly, the patient had completed a 5-day course of ceftriaxone and azithromycin by this point in time.
In the setting of IE, the patient was no longer eligible for TAVI. Despite restarting antibiotics, his condition deteriorated. A goals of care discussion was held with the patient and his family. He expressed that he did not want any further escalation of care. Transfer to his home hospital was arranged for palliation. He passed away days later with family at the bedside.
Discussion
We report the case of an 85-year-old male with severe aortic stenosis who was awaiting TAVI. He presented to the ED with decompensated heart failure, and was unexpectedly found to have mitral valve endocarditis.
The risk of IE while waiting for TAVI, or valve surgery in general, is not well-studied. Instead, the literature focusses on the risk and management of IE following intervention. Patients waiting for TAVI have risk factors for IE. Firstly, structurally abnormal valves can serve as a substrate for IE.4,5 This includes aortic stenosis, which is present in 10%-18% of IE cases.4,6 Secondly, TAVI candidates tend to be older, medically complex patients who are not suitable for surgical replacement. Age and certain comorbidities, such as severe kidney disease (OR 16.9, 95% CI 1.5-193, p = 0.02) and diabetes (OR 2.7, 95% CI 1.4-5.2, p = 0.004), are known risk factors for IE.7,8
Our patient had multiple risk factors for mitral valve endocarditis, including his pre-existing mitral stenosis and regurgitation, age, and diabetes. This patient also had frequent lab draws and IV insertions for iron and blood transfusions due to recurrent gastrointestinal bleeding, raising the possibility of introducing skin flora into the bloodstream. 8
Finally, this case highlights the use of echocardiogram in the pre-TAVI period. The American College of Cardiology and American Heart Association provide recommendations on the use of echocardiogram in the setting of severe aortic stenosis. 3 Echocardiogram is used at the time of diagnosis to assess severity and suitability of anatomy for TAVI. Typically, a repeat echocardiogram is then done at the time of TAVI. There are no recommendations regarding the use of echocardiogram in between these 2 time points as patients wait for TAVI. Similarly, there are no recommendations on the use of echocardiography in the period prior to TAVI in the joint guideline by the European Association of Echocardiography and the American Society of Echocardiography. 9
Our center routinely performs focused echocardiography immediately before TAVI procedures, elucidating any changes that may have occurred since initial diagnosis. Our protocol involves limited parasternal, apical and subcostal views, with attention to new or worsening left ventricular dysfunction, significant mitral and aortic regurgitation, pericardial effusion, increased pulmonary artery pressures, or as in this case, the presence of a new mass. Operator awareness of these new findings may result in modifications to the procedure, anesthesia plan or change in management. Additionally, this echocardiogram serves as a baseline prior to the procedure and facilitates the identification of any procedural complications.
Given that TAVI patients have risk factors for IE, clinicians must maintain a high index of suspicion. We suggest screening patients waiting for TAVI for IE on history and physical examination. In the setting of progressive (eg, worsening heart failure) or new symptoms (eg, fever), an echocardiogram should be done. Further research is required to elucidate the role of routine echocardiography in the pre-TAVI period in patients who do not have a change in clinical status.
Conclusion
We present the case of an 85-year-old male awaiting TAVI with decompensated heart failure due to mitral valve endocarditis. Clinicians should understand that patients awaiting TAVI have multiple risk factors for IE, including valvular disease, advanced age, and certain comorbidities. IE should be considered as a cause of decompensated heart failure in this population. Further research is required to better understand this risk, to determine if preventive measures are warranted, and to inform the use of screening echocardiography in the pre-TAVI period.
Footnotes
Acknowledgements
This work is done in memory of the patient who ultimately received palliative care and passed away.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed to the design of the work, interpreted the data, drafted the article, and approved the final version of the manuscript.
Consent
Consent was obtained from the patient’s next-of-kin.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.