
Abstract
Background:
Ovarian ectopic pregnancy is a rare form of non-tubal ectopic pregnancy. It can rupture before the end of the first trimester, causing hemoperitoneum, and present with signs and symptoms similar to other commoner abdominal emergencies or the pregnancy can continue intraperitoneally. Therefore, they are not often diagnosed preoperatively. Ultrasound can assist in diagnosis of ovarian ectopic pregnancy but the findings could be ambiguous or inconclusive. We present a case of ruptured ovarian ectopic pregnancy at the second trimester causing massive hemoperitoneum that was suspected as an intrabdominal malignancy co-existing with intrabdominal pregnancy.
Case presentation:
She was a 34 year-old Nigerian unbooked G4P3+0, (3 alive), who presented to the labor ward on 21st January, 2021 with a complaint of a 6-week history of abdominal pain and swelling. Pain was insidious in onset, generalized, non-colicky, non-radiating, constant, no known aggravating or relieving factor, but it was of moderate intensity. She had amenorrhea with a positive serum pregnancy test without prior early ultrasound. At presentation, initial abdominopelvic ultrasound revealed intra-uterine viable pregnancy but repeat ultrasound done showed a left adnexal ectopic gestation and an echo-rich intraperitoneal fluid collection. Laparotomy was done and ovarian pregnancy was accurately diagnosed intra-operatively. Tissue samples from the ovary confirmed normal products of conception, namely chorionic villi, trophoblastic cells and ovarian stroma at histology.
Conclusion:
Despite advances in imaging techniques, the diagnosis of ovarian ectopic gestation is still very difficult. When premenopausal women present with amenorrhea, generalized non-colicky abdominal pain and swelling in combination with ambiguous findings of pregnancy on ultrasound in the absence of trauma, differential diagnoses should include ruptured ovarian pregnancy. Obstetricians should maintain a high index of suspicion to forestall delayed diagnosis and the potential maternal morbidity and mortality. However, the need for high-index of suspicion should be for any ectopic, not just ovarian pregnancy.
Introduction
Ovarian pregnancy is a rare form of ectopic pregnancy. Its incidence is 0.5% to 1% of all ectopic gestations, or 1 in 7000 to 40,000 live births. 1 The diagnosis is intricate and based on surgical and histopathological observations and its recognition is imperative as it can be potentially life-threatening when intra-abdominal bleeding and potentially shock occurs.1,2
According to current literature, ruptured ovarian ectopic pregnancy is rarely diagnosed preoperatively, as it shares similarities with other more prevalent abdominal structures at emergencies.2,3 Although transvaginal ultrasound is a valuable diagnostic method to detect early ovarian pregnancy, specific ultrasound features that aid a preoperative diagnosis may not always be visible. Therefore, pelvic ultrasound should be performed more carefully in such patients. Higher suspicion for a ruptured ovarian ectopic pregnancy will facilitate the decision to pursue a laparotomy or laparoscopy. Here we discuss a case of a ruptured ovarian ectopic pregnancy that presented with clinical and imaging findings that initially raised suspicion for intrabdominal malignancy, intrauterine pregnancy initially and ectopic pregnancy at repeated imaging study. We aim to clarify some of the key preoperatively and intraoperatively findings that are helpful for differentiating between intrauterine pregnancy and ectopic pregnancy in low-and middle-income settings.
Case Presentation
A 34-year-old Nigerian unbooked G4P3+0A3 presented to our labor ward on January 21, 2021 with a complaint of a 6-week history of abdominal pain and swelling. Pain was insidious in onset, generalized, non-colicky, non-radiating, and constant with no known aggravating or relieving factor and of moderate intensity. Her last menstrual period was in September 19, 2020 and pregnancy was confirmed by a positive serum pregnancy test. Her gestational age at presentation was 17 weeks plus 5 days, however no early ultrasound scan was done. On examination, she was chronically ill-looking, pale, afebrile, dehydrated. Her temperature was 36.5°C, pulse rate was 135 beats per minute, respiratory rate was 20 cycles per minute and blood pressure was 120/70 mmHg. Her abdomen was non-uniformly distended but moved with respiration, there was mild generalized tenderness (Figure 1). There was right iliac fossa tenderness. There was a right iliac fossa mass, non-tender with a fairly smooth outline and not attached to the overlying skin, non-mobile with no differential warmth, and we could get above but not below it.

Pre-incision abdominal exposure showing non-uniform abdominal shape.
On examination, we found a gaping introitus with anterior vaginal wall bulge. The cervix could not be visualized on speculum examination. On digital exam, the cervix was found to be displaced anterior-laterally toward the 10 o’clock position and the os was closed.
An assessment of suspected intra-abdominal malignancy in pregnancy with severe anemia was made. An urgent packed cell volume was done and it was found to be 0.14 L/L. We also requested full blood count, serum electrolytes, urea and creatinine which showed normal values. Four units of blood were grouped and cross-matched. She was commenced on intravenous antibiotics. Initial abdominopelvic ultrasound scan revealed a gravid uterus that harbored a viable fetus with the placenta on the right lateral wall of the uterus which was not low-lying and with no adnexal mass lesion seen. A maternal echo-rich intraperitoneal fluid collection noted in all the 4 quadrants and abdominal tap revealed 10 ml of non-clotting blood. Repeat abdominal ultrasound scan revealed a left adnexal ectopic gestation and an echo-rich intraperitoneal fluid collection. Patient had exploratory laparotomy and ovarian marsupialization and peritoneal lavage via an extended midline longitudinal incision with the following intra-operative findings: hemoperitoneum of 2.5 L, a left adnexal gestational sac on the left ovary (placental insertion originated from the left ovary), the gestational sac was attached to but separated from the posterior uterine wall, the uterus was bulky, and intact the right ovary was not visualized, the right fallopian tube was swollen and tortuous, the left fallopian tube was intact and adherent to the surface of the gestational sac. The estimated blood loss was 500 ml and there was a viable male fetus (Figures 2 and 3).
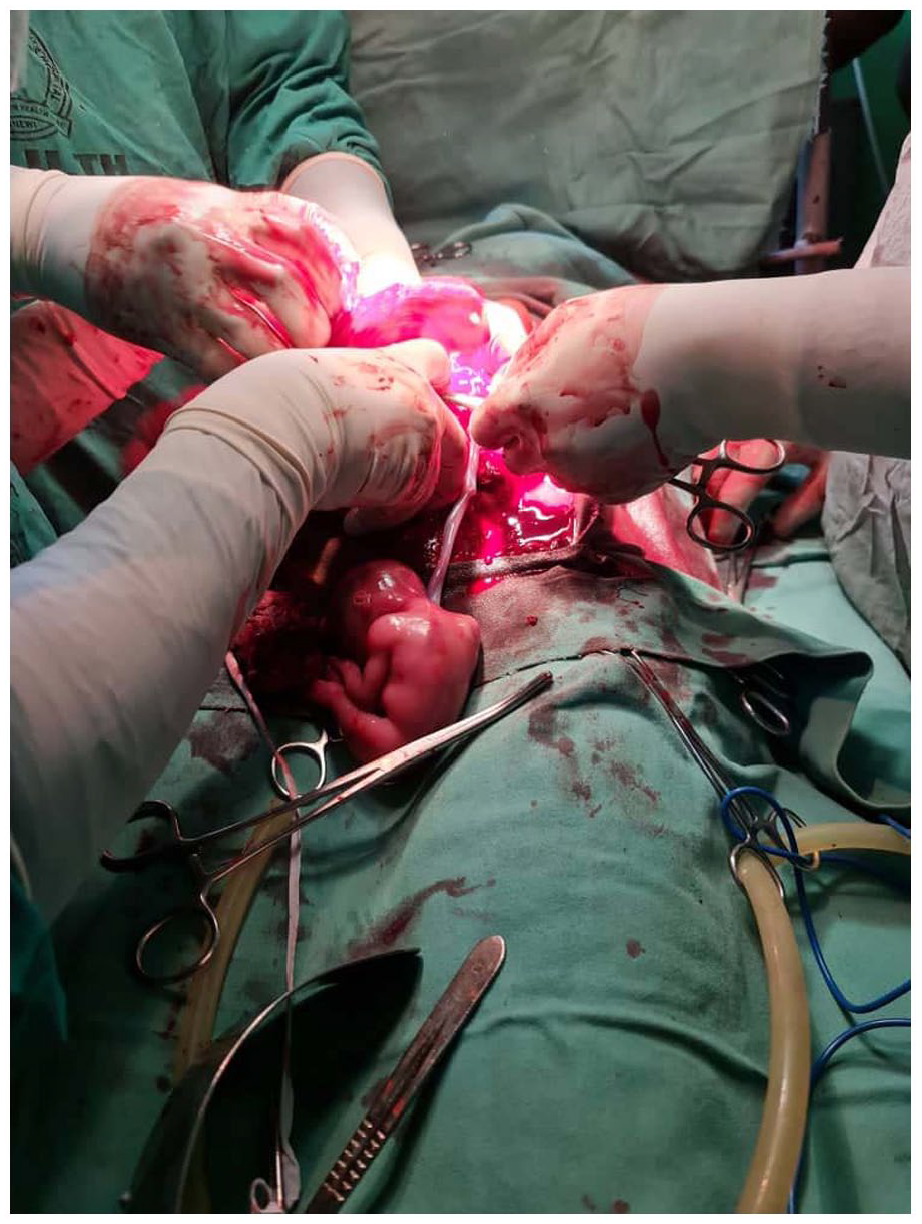
Intra-operative findings.

Extruded fetus and the placenta and other products of conception.
The patient received 4 units of blood intra-operatively and she was placed on intravenous antibiotics. On the second post-operative day, she had paralytic ileus which was managed conservatively. The subsequent post-operative days were uneventful and she was discharged on the 8th day post-operation.
The histology of submitted specimen report showed normal chorionic villi, decidualized ovarian stroma, hemorrhagic areas and areas of necrosis. Harvested fetal organs show normal histology. The overall features are those of normal products of conception.
Discussion
Ovarian ectopic pregnancy is a rare clinical finding especially in Nigeria. As in our case, it is a documented rarity which makes many clinicians misdiagnose a patient presenting with amenorrhea and abdominal pain. Close differentials include a ruptured tubal pregnancy and a corpus luteum cyst. There were no risk factors identified in our patient, except the intraoperative findings of edematous fallopian tubes, suggestive of pelvic inflammatory disease. 3 This was also similarly reported in some other case reported by different authors.1,2,4,5
Although ovarian pregnancy is considered a rare pregnancy complication, however, an increase in the number of cases is being noted. This increase in the incidence of ovarian ectopic pregnancy has been linked to extensive use of intrauterine contraceptive device, history of ectopic pregnancies, fallopian tube surgery, ovulation induction drugs, and assisted reproductive techniques like in vitro fertilization, embryo transfer, and empty follicle syndrome.3,4 Regarding ovulation induction, Fernandez et al. 5 reported that ovulation induction carries an increased risk of ovarian pregnancy. During ovulation induction, the increased level of estrogen and progesterone is thought to inhibit the frequency of tubal peristalsis. This could affect its normal movement.
The etiology of ovarian ectopic pregnancy is not clear, however 2 hypotheses have been put forward. One hypothesis is the reflux of conceptus from the tube leading to implantation in the ovary. 6 The second hypothesis suggests that it occurs due to failure of ovum release probably due to thickening of the tunica albuginea.2,6
Imaging can be used to diagnose ovarian pregnancy. In the first trimester, on ultrasound, the gestational sac adjacent to the ovary is described as a double echogenic ring within a hypoechoic adnexal mass and the presence of ovarian cortex which includes corpus luteum follicle around the mass because of the peripheral vascularity and the sac.7,8 This finding was not noted in our patient as she presented at an advanced gestational age. Tubal ring sign becomes a less specific finding for ectopic pregnancies in the second trimester,7 -9 but one feature that will still maintain an accurate distinction between ectopic and intrauterine pregnancies is mantle distance, defined as the thickness of the myometrium surrounding the gestational sac. Measuring mantle distance screens for asymmetric implantation suggestive of ectopic pregnancy. 10 A recent review of ectopic pregnancy and ultrasound literature, Lewiss et al concluded that a mantle distance <8 mm was a sensitive cut-off for gynecologists working in emergency areas to suspect ectopic pregnancy. 10 Also, recently, a case report by Keller et al, on a series of visits by a pregnant woman in her second-trimester of pregnancy which was deemed intrauterine on transabdominal ultrasound due to gestational age and location-who later developed massive hemoperitoneum and was diagnosed with a ruptured 15-week tubo-ovarian pregnancy on laparotomy was reported. 8 The case emphasized the possible sonographic discoveries that could have aided in making the appropriate judgment. This is particularly mantle distance-the thickness of the myometrium adjoining the gestational sac-which would have correctly recognized the pregnancy as ectopic. Mantle distance was not calculated in our patient as such technique is not fully implemented in low-and middle income countries like Nigeria.
In a similar case, a 26-year-old Asian woman who presented with a case of ruptured ovarian pregnancy in the second trimester also complained of an abrupt mental change. 11 Therefore, the psychological ill health can be an outcome of this type of ectopic pregnancy.
The diagnosis of primary ovarian pregnancy is made based on the Spigelberg criteria.12,13 It includes: intact fallopian tube on the involved side, gestation sac in the cortical region of the ovary, histologically proven gestation sac in ovarian tissue, and ectopic pregnancy attached to the uterus by the utero-ovarian ligament. Following these criteria, our case fits the complete description of ovarian ectopic pregnancy. In our patient, the left fallopian tube was intact but adherent to the gestational sac, and placental insertion was found to be on the left ovary. The adherence of the intact left fallopian tube to the gestational sac could probably be due to the advanced gestation. Second-trimester ectopic pregnancy are exceedingly rare because of the vascularity and elasticity required to support such an advanced pregnancy. The histology report was also synchronous as histology revealed normal chorionic villi, decidualized ovarian stroma, hemorrhagic areas, and areas of necrosis with the harvested fetal organs showing normal histology.
Historically, ovarian ectopic pregnancy was managed by ipsilateral oophorectomy. The trend moved to uterine sparing surgeries such as cystectomy and wedge resection but currently laparoscopic surgery is the choice management. 3 Additionally, reports have shown increased rates of conservative management for ovarian ectopic pregnancy and other ectopic pregnancy types.13,14 In this patient, laparotomy was done because of the massive hemoperitoneum in addition to the fact that the diagnosis was still in doubt till it was accurately diagnosed intra-operatively.
One of the limitations of this case report is that the case presented with unstable hemodynamics in emergency hours. This makes it impossible for embarking on conservative management of ectopic pregnancy coupled with the fact that the risk factors present in the patient could not be fully studied. 14 Additionally, since the obstetrician-gynecologists are becoming increasingly more alert globally, it has become the standard practice to evaluate the adnexal area for ectopic pregnancies so that this dangerous diagnosis of rupture ovarian pregnancy is not missed.13,14 Therefore, the index report could serve more than just a reminder of the importance of having a lower threshold of suspicion, but serves as an impetus for exploring more of what can be done to prevent similar situations from occurring in lower income pregnant women population groups. In Nigeria, there is notable poor patients early turn-up to hospitals coupled with a poor system for gynecologic emergencies.15,16 A better solution to this problem is advocacy for early recognition for danger signs of ectopic pregnancy in the rural and sub-urban communities and early presentation of women that have cases of ovarian ectopic pregnancy. This is because, late presentation could be a challenge in diagnosing ovarian ectopic pregnancy as well as a challenge in life threatening emergency. Thus, early ultrasound scanning to confirm intrauterine pregnancy could be a preventative salvage factor.
Conclusion
Despite advances in the imaging techniques, the diagnosis of ovarian ectopic gestation is still very difficult. When premenopausal women present with amenorrhea, generalized non-colicky abdominal pain and swelling in combination with ambiguous findings of pregnancy at abdominopelvic ultrasound in the absence of trauma, differential diagnoses should include ruptured ovarian pregnancy. Its diagnosis is difficult and relies on criteria based on intraoperative findings. Obstetricians should maintain a high index of suspicion to forestall delayed diagnosis and the potential maternal morbidity and mortality. However, the need for high index of suspicion should be for any ectopic, not just ovarian pregnancy. Therefore, the index report serves more than just a reminder of the importance of having a lower threshold of suspicion, but serves as an impetus for exploring more of what can be done to prevent similar situations from occurring in lower income pregnant women population groups. The aspects of management in this case that were compromised on or made more difficult due to the patient’s socioeconomic status included late presentation since the gestational age at presentation was 17 weeks plus 5 days. This could be due to cost or fear of earlier presentation. Also, due to similar reasons, no early ultrasound scan was done.
Footnotes
Acknowledgements
The authors thank the Histopathology department of Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
GUE, GOU, TKN, CCO1 and CCO2 conceived, supervised the study and performed the surgery; ECI, CON, OPA, MEC and CGO analyzed data; OCE, OAO, PCO, JIM, COD, NPO, JCA, NCO, JEO, DEM, CIN, EUN and OOE wrote the manuscript; EPI, HCN, OOD and GUE made manuscript revisions. All authors reviewed the results and approved of the final version of the manuscript.
Ethics
A written informed consent was obtained from the patient to allow the reporting of this case as well as the use of her intraoperative picture.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal