
Abstract
Epididymo-orchitis is a common intra-scrotal inflammation among males that causes swelling of the epididymis and testis. In the era of modern antibiotics, complications associated with this condition are now rare. Herein, we report a 28-year-old man with acute epididymo-orchitis complicated by the formation of several abscesses involving the left testis and seminal vesicles. The literature review showed this patient as the first case with such extensive complications following epididymo-orchitis. Initial antimicrobial therapy was unable to resolve the condition. The management necessitated surgical intervention, which included MRI-guided aspiration of the seminal vesicle abscesses and testicular sparing drainage of the testicular abscess.
Introduction
Epididymo-orchitis (EO) is the most common etiology of intra-scrotal inflammation in men older than 18 years of age. 1 Recent studies showed that about 2.45 cases per 1000 men seek outpatient consultation with EO, 2 and over 600 000 American men present to emergency departments with this condition each year. 1
EO is mostly happening secondary to the retrograde spread of infection through the vas. 2 In males aged below 35 years, the offending organism is commonly sexually transmitted Neisseria gonorrhoeae or Chlamydia trachomatis, while in men older than 35 years, enterobacteria are frequently incriminated. 3
The diagnosis is usually settled because of the clinical picture and physical assessment. Patients are mostly complaining of scrotal pain, which may be accompanied by fever, nausea, vomiting, and exhaustion.1,2 Yet, in addition, further evaluation could be useful in affirming the diagnosis of EO and recognizing complications. In the era of recent antibiotic therapy, EO could be successfully treated without sequels. Therefore, EO seldom advances to abscess formation.3,4
In this article, we report a case of bilateral acute EO that was poorly managed initially, progressed to abscess formation in several genital organs, and eventually necessitated surgical interference.
Case Presentation
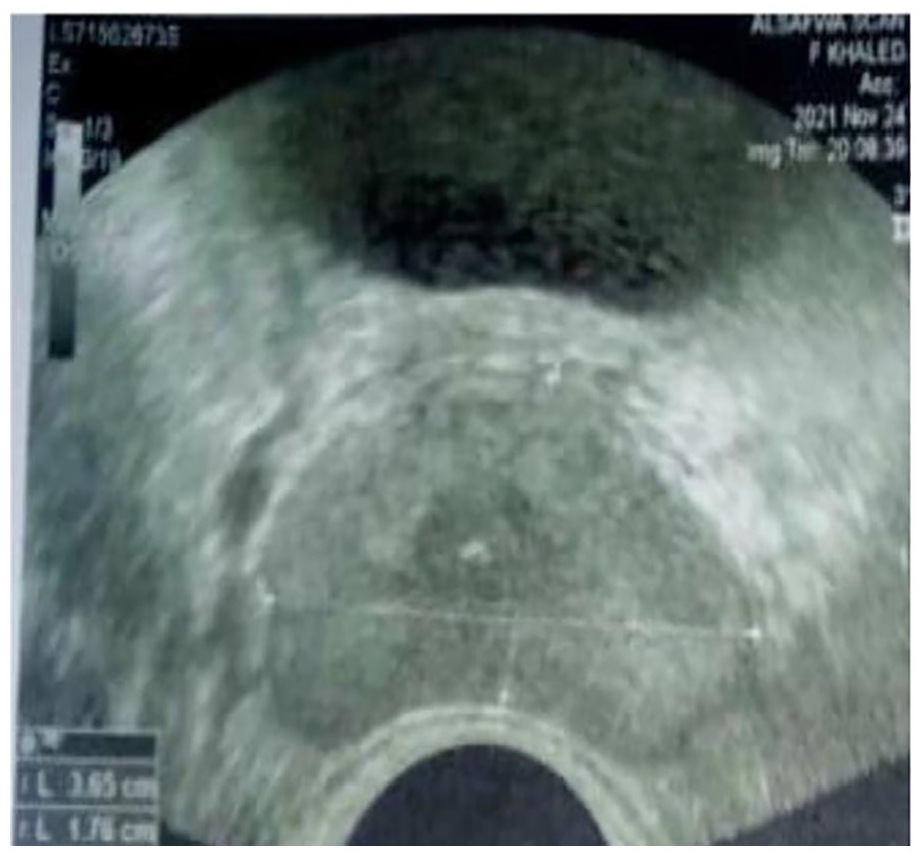
A 28-year-old married male sought medical advice at a urology clinic in his rural hometown after complaining of painful scrotal swelling for 1 week. On a spot diagnosis, the urologist identified the patient as having bilateral EO. The only requested investigation, at that time, was a urine analysis, which indicated 12-15 pus cells/HPF. The patient received a prescription containing ciprofloxacin 500 mg tablet/12 hours, and some analgesics. Five days later, the patient noticed stepping pain in his scrotum, along with worsening scrotal swelling. Also, he started to have a fever (40°C), chills, a sense of unease, anorexia, and nausea. The patient, therefore, consulted another urologist in his hometown for these emerging symptoms. This second urologist clinically confirmed the previous diagnosis of bilateral EO. Sulbacef (sulbactam & cefoperazone) 1.5 g vial/day and Voltaren injection every 12 hours were prescribed by the urologist. This treatment was planned to last for 7 days. Until the fourth day, the patient did not show any improvement, although he strictly followed the recently scheduled treatment regimen. Instead, the patient got extremely sick. The fever rose (41.5°C), and he started vomiting. He could not sleep for 24 hours a day, and he was exceptionally exhausted. A laboratory biochemical check-up, at that time, showed an elevated leucocytic count (24. 3 × 103/mL; the normal is 4-11 × 103/mL), neutrophilic predominance (88%; the normal is 35%−80%), and high C-reactive protein (96 mg/dL; the normal is <6 mg/dL). Blood urea and serum creatinine were normal. A digital rectal examination revealed tender cystic structures over the prostate, indicating enlarged seminal vesicles. Because transrectal ultrasound (TRUS) was not available, transabdominal ultrasound was done first in the urologist’s office. The scanning showed markedly dilated seminal vesicles. The urologist requested TRUS to further clarify the pathological nature of the dilated vesicles. The TRUS confirmed the existence of markedly distended seminal vesicles (up to 4 cm in diameter) with hyperechogenic contents suggesting abscesses formation (Figure 1), and a midline prostatic cyst (5 mm in diameter) (Figure 2). A cystourethroscopy was done, and an enlarged cystic prostatic utricle was seen, which was immediately resected. During the resection, a gush of frank pus appeared coming from the right side of the utricle. A urethral catheter was fixed for 24 hours and the patient was kept again on Sulbacef in the emergency department. The patient showed considerable improvement starting the next day. The fever disappeared, and the body temperature was around 37°C. He could sleep after several days of continuous insomnia. His appetite improved, and oral feeding was resumed. However, 4 days later, the previously annoying symptoms recurred.

Transrectal ultrasonography showed markedly dilated seminal vesicles with hyperechoic density, suggesting the existence of abscesses.
Transrectal ultrasonography showing the prostate with a 5 mm central utricle cyst harboring calcific foci.
Herein, the patient’s family sought counsel at the Urology Outpatient Clinic, Alexandria Main University Hospital. The patient denied a history of any genital trauma, diabetes, tuberculosis, urethral discharge, sexually transmitted diseases, extramarital relations, or previous similar conditions. He had a history of primary infertility for 7 years. The repeated semen analyses showed azoospermia with a low semen volume (0.7-0.9 mL), and the FSH assay was high-normal (11.5; the normal level is 1.5-12.4 mIU/mL). Physical examination disclosed tachycardia (112 beats/minute), low blood pressure (100/65), and fever (40.5°C). The upper abdomen was lax, but the supra-pubic area and both inguinal regions were tender and rigid. The scrotum was erythematous and swollen, with excoriated skin on its left side. On palpation, the scrotum was tender and indurated, and the epididymes were not palpable from the testes. The spermatic cords were also tender and indurated. A digital rectal examination revealed remarkably enlarged and tender seminal vesicles. The patient received a magnetic resonance imaging (MRI)-pelvis examination. The image showed notably dilated seminal vesicles (Figure 3) with diverse signal intensities from normal. The left testis also suspiciously showed a fluid collection in its lower pole, suggesting an impending abscess formation (Figure 3). An immediate transrectal aspiration of seminal vesicles was done under MRI guidance. The aspiration yielded frank yellowish pus, around 75 mL in volume. The aspirate was referred for bacteriologic examination, and the culture later grew Escherichia coli (E. coli) with susceptibility to Merional (Meropenem). The patient was scheduled to receive Merional (1 gm/12 hours) for 5 days on an outpatient basis immediately after the aspiration and before getting the bacteriologic report. Three days later, the patient came for a follow-up. He showed distinct clinical improvement. His laboratory results returned close to the normal ranges (total leucocytic count fell to 12 × 103/mL, neutrophils subpopulation fell to 77%, and C-reactive protein fell to 48 mg/dL). The right testis started recovering but on the contrary, the left testis was still tender and enlarged. The next day, while at home, pus started to come from the lower pole of the left testis. The patient was immediately re-admitted to the hospital and received surgical exploration of the scrotum. An abscess (2 cm × 3 cm) in the lower pole of the markedly left swollen testis was detected (Figure 4) with areas of necrosis. A fibrous capsule surrounded the abscess except at the site of the discharge. The drainage of the abscess produced a frank yellow discharge. Testicular sparing surgery with debridement of the necrosed parts was expedited. The testicular tissue around the abscess seemed viable. The patient left the hospital after a few hours and continued on Merional for 2 days. The patient then began a 2-week course of oral Augmentin 1 g/12 hours until his first follow-up visit. Two weeks later, the patient attended the outpatient clinic. His general condition was fine. The scrotal incision healed, and the previous tenderness and swelling of the left testis almost disappeared. A repeat transabdominal ultrasound showed normal-sized seminal vesicles. The total leucocytic count was 9 × 103/mL and CRP was 5 mg/dL. The patient continued to be symptomless for 5 months after ending the Augmentin course. A scrotal duplex, at that time, showed unremarkable findings. Two repeated semen analyses revealed normal semen volumes (4.5 cc and 3.8 cc) but with azoospermia.
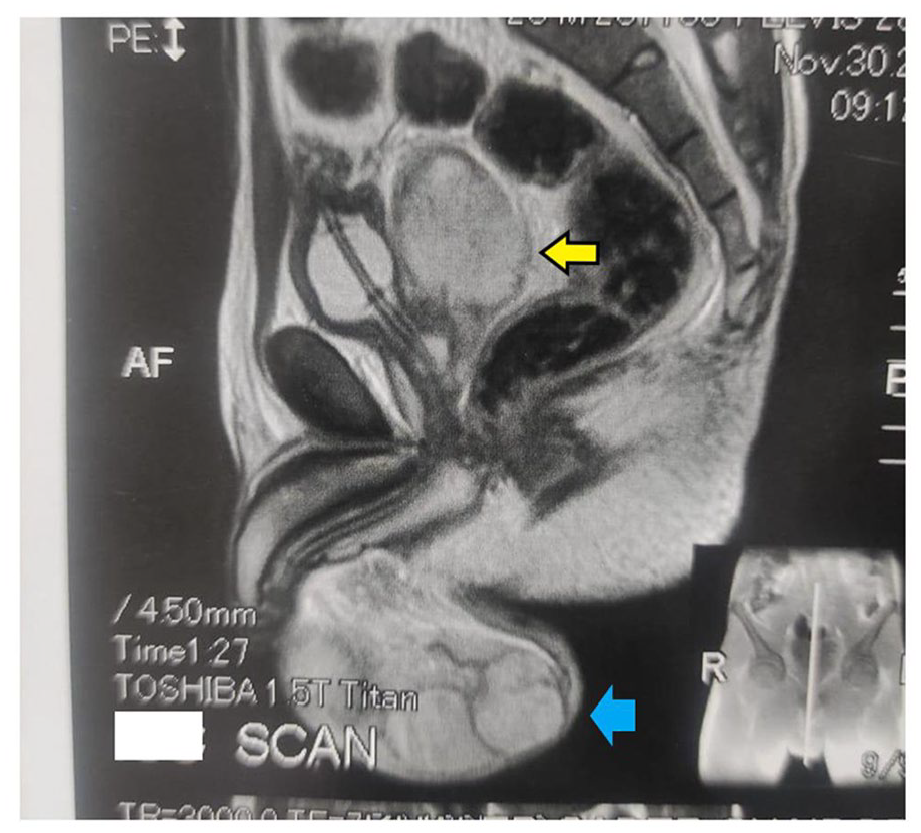
MRI-pelvis showing markedly dilated left seminal vesicle (the yellow arrow), reaching 5 cm in the anteroposterior diameter. There was a fluid collection in the lower pole of the left testis (the blue arrow), suggesting a potential abscess formation.

Surgical exploration of the left testicular abscess (TA) with drainage and debridement. The tip of the finger demonstrates the cavity of the drained abscess.
Discussion
EO is the inflammation of the epididymis and the adjacent testis. Orchitis mostly occurs after the spread of inflammation from the epididymis. EO usually resolves conservatively and is rarely complicated.3,4 Acute EO, on the other hand, usually necessitates prompt and careful management to avoid complications and protect against loss of testicular tissue quality. The diagnosis is mostly done based o the clinical picture and physical examination.1,2,5 In this report, the initial management of the patient implemented by the first urologist had, unfortunately, some shortcomings. First, there was no full genitourinary assessment to feel the seminal vesicles during the digital rectal examination, although it is well known that EO mostly occurs after seeding of urinary microorganisms into the epididymis by retrograde progression through the ejaculatory duct and vas deferens. 3 Second, no urogenital imaging like TRUS to search for any structural anomalies of the prostate which may contribute to prostatitis, 6 particularly in the presence of a low semen volume and azoospermia. Prostatitis is now regarded as a risk factor for EO. 5 Third, no urine culture was requested although the urine analysis showed about 15 pus cells/HPF. In this situation, no data was available about the offending microbe. This may be particularly important in this patient whose genital system was also not screened. Previous researchers reported that when enterobacteria is the causative organism in EO, this is frequently associated with anatomical urogenital anomalies. 5 At the same time, the identification of the most suitable antibiotic against the offending organism, which could replace the empirical antibiotic was missed. Fourth, and probably the most critical shortcoming, was that no re-evaluation was booked, despite the patient’s complaints being maintained and even worsening (eg, a fever reaching 41.5°C). Re-assessment of patients with EO is recommended after 3 days of starting empiric antimicrobial therapy. 2 It is of utmost importance that the physician should tell the patient what to do if things deteriorated rather than improved.
In the present report, the patient did not initially respond to the empiric antibiotic therapy. TRUS, done later, showed the presence of a prostatic utricle cyst, which blocked the ejaculatory ducts leading to a low semen volume. This structural anomaly, together with other associated factors like diabetes, long-standing urethral catheters, and urethral manipulation, can be precipitating factors for the development of a seminal vesicle abscess (SVA). 6 The reported patient’s prostatic utricle cyst may play an additional role in the predisposing to the initiation of EO itself, 7 with a special preference for men under 35, 8 like the patient in this report. So, prostatic pathology could play a dual role in the patient’s presentation.
SVA is an uncommon pathological condition whose precise etiology remains obscure. So far, 41 cases have been reported in the English literature. 9 SVA can cause a variety of symptoms, including testicular and inguinal pains, fever, and malaise, 10 as described by the patient in this report. It has always been challenging to diagnose SVA until the advent of the TRUS and the ensuing MRI. The initial diagnosis of SVA in our patient was made by TRUS, which usually gives a good diagnostic idea about the existence of SVA. 11 However, we shifted later to MRI to manage the SVA. MRI was more comfortable for the patient during imaging and aspiration, and it could scan the SVA in several plan sectors, giving more comprehensive information 10 without the risk of inciting bacteremia as TRUS did. 12 So, the MRI in the present report was both diagnostic and remedial for the SVA. For these reasons, MRI is now strongly recommended for assessing seminal vesicular pathological conditions. 13 Additionally, MRI, in our patient, could provide a preliminary idea about the scrotum in the same films as SV. It highlighted the fluid collection in the lower pole of the left testis, which suggested a potential TA.
SVA may resolve, on rare occasions, with proper parenteral antibiotic therapy. 14 If conservative therapy fails, surgical drainage via transurethral, 15 transperineal,10,11 or transrectal routes11,12 may be performed. In the present report, the patient underwent drainage of SVA on 2 occasions. The first, via the transurethral route, was not effective enough to completely drain the seminal vesicles. The second was expedited through the transrectal approach under MRI guidance and has been determined to be effective. The drained pus grew E. coli. This is consistent with the findings of several workers who showed that E. coli is the most common offending organism in SVA.10,16
In the present report, the inability of EO to resolve under parenteral antimicrobial therapy ended with suppurative necrosis at the lower pole of the left testis and TA development. Therefore, we think that a non-resolving EO should attract attention to the possibility of TA formation. Several cases of TA preceded by EO, unfortunately, ended with orchiectomy. 17 Rapid management of TA is, therefore, important to avoid loss of testicular tissue and compromise of future fertility.
In the era of modern antimicrobial therapy, EO rarely pursues TA development. 3 Some studies demonstrated an incidence of 3.5% for TA in males with EO. 18 This rarity of TA makes its precious pathogenesis unclear. However, tissue edema and exudate associated with EO may cause tissue compression and venous congestion, which both result in hypoxia. Such an event sequence may precipitate abscess development. 19 The TA in our patient discharged copious pus and had a maximum dimension of 3 cm. It required, therefore, surgical intervention. 20 We did abscess drainage and tissue debridement in a testicular sparing intervention. TA can, at some occasions, be managed conservatively with a broad-spectrum antimicrobial therapy and serial ultrasound scanning to follow the progress of the abscess. 20 TA can also be treated surgically. Percutaneous aspiration, 21 open incision and drainage 22 as in the current patient, and orchiectomy 20 all are options. Surgical intervention is usually the treatment of choice when the abscess’s greatest dimension exceeds 0.5 cm, 20 The patient, in the present report, had a good outcome based on a scrotal duplex at 5 months after recovery.
EO related to different pathogens has an impact on human sperm parameters. This may appear in the form of a decline in count, motility, morphology, and fertilizing potential during the disease, and improvement of these deteriorated parameters after resolution of the condition. 23 The same deleterious effect on sperm characteristics appears also in rodent models, 24 which luckily lack the uneven distribution of patient features, that may adversely and coincidentally affect sperm attributes, for example smoking. Therefore, EO in rodent models has a genuine detrimental impact on sperm parameters. This negative influence of EO on the seminogram could not be declared for the reported patient, who had azoospermia long before the commencement of the disease. It was only the semen volume that showed remarkable increase after resection of the prostatic utricle cyst.
In this report, we described a case of bilateral acute EO with prostatic pathology that advanced to the emergence of several abscesses in the left testis and seminal vesicles. To the best of our knowledge, this is the first case showing the capability of EO to be extensively complicated and have sequels in different sites of the male genital system. Given the scarcity of information on best practices for the management plans of EO, this report may indicate the need to update the current treatment guidelines for EO.
Conclusion
A digital rectal examination should never be missed in men with EO to evaluate the status of the prostate and seminal vesicles. Improper management of EO, particularly in the presence of prostate pathology, may be complicated by the formation of multiple abscesses in the male genital system. Once the treatment of EO is refractory to antibiotic therapy, the existence of abscesses in the male genital system may be anticipated. Under such conditions, surgical intervention of abscesses should be seriously considered in order to avoid its impact on male fruitfulness.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
N.S. contributed to the conception and design of the study, analysis, and interpretation of data, and drafting the article with final approval of its completed form. A.H. contributed to collection, analysis, and interpretation of data, and drafting of the article with final approval of its completed form. O.S.H. contributed to the drafting the article with final approval of its completed form.
Informed Consent
The patient has consented to his case information for publication purposes.