
Abstract
Breast cancer might be complicated by distant metastases accompanied by hypercalcemia, but hyperparathyroidism is not commonly considered in the differential diagnosis. We present a case of 38 years old female patient who was diagnosed with ductal breast carcinoma. Eight months after the initial diagnosis the patient was diagnosed with distant bone metastases. However, this diagnosis was reconsidered at follow up, because we identified elevation of PTH 137.2 pg/ml, Ca2+ 1.19 mmol/l, albumin corrected calcium 2.42 mmol/l, 25(OH)D 39.4 nmol/l, indicating hyperparathyroidism. Scintigraphy with 99mTC-sestamibi confirmed parathyroid adenoma. Postoperative histopathology confirmed 1.2 g chief-cell PTA. Two months after the operation both PTH and Ca2+ levels were within the normal ranges. This study emphasizes the importance of considering possible hyperparathyroidism in patients with breast cancer and hypercalcemia. Routine evaluation of PTH is considered as a reasonable test in patients with breast cancer accompanied by bone lesions.
Keywords
Background
Breast cancer is the most common malignant neoplasm in women. 1 In some cases, breast cancer might be accompanied by hypercalcemia as a consequence of bone osteolysis due to overproduction of parathyroid hormone-related protein (PTHrP), resulting in increased calcium loss due to urine excretion and bone resorption.2,3 In addition, the metastatic spread of breast cancer to the skeleton is usually associated with hypercalcemia and decreased parathormone (PTH). Hypercalcemia and bone lesions are also symptoms of primary hyperparathyroidism (PHPT).4,5 Hypercalcemia in PHPT appears as a response to the overproduction of PTH by parathyroid adenoma (PTA) or carcinoma.5,6 PHPT might be asymptomatic, normocalcemic, or with an unusual presentation, causing no specific symptoms; and therefore, it might escape from the early diagnosis and subsequently cause severe complications.4,5,7,8 Bone loss should always be considered in patients with breast cancer due to hormone-ablative therapy.9,10 On the other hand, the bone is a frequent site of breast cancer distant metastases, accompanied by hypercalcemia, but not with the elevated PTH. In such circumstances, PHPT as a cause of bone loss is not commonly considered in the differential diagnosis, resulting in less effective management of osteolytic lesions in cases of unrecognized diagnoses.
The aim of this study was to emphasize the importance of differentiating the primary hyperparathyroidism from hypercalcemia or metastases to the bones in patients with breast cancer.
Case presentation
A female patient (born in 1983) with a body mass index of 28.34 kg/m2 was diagnosed with ductal breast carcinoma in October 2019.
At the baseline, preoperative whole-body computed tomography (CT) scan was performed and right breast mass was confirmed, whereas lesions to the bones were not identified. Preoperatively, serum calcium was not evaluated because it is not on the list of routine preoperative investigations. The patient underwent a right lumpectomy and axillary dissection. Postoperative histopathology revealed poorly differentiated (G3) ductal right breast carcinoma 1.5 cm in the largest diameter and local metastases (pT1 pN2a (7 lymph nodes with metastases out of 33 dissected) cM0). The patient was administrated 6 courses of adjuvant chemotherapy by cyclophosphamide 1000 mg and doxorubicin 110 mg in November 2019.
Molecular and genetic findings
Immunohistochemistry (IHC) revealed estrogen receptors 80% positive cells, positive progesterone receptors, negative HER2/neu, and c-erb-2. MIB-1 proliferative index was 40%. BRCA1 and BRCA2 showed no mutations. Fluorescence in situ hybridization showed no amplification for HER2/neu.
Diagnosis of hyperparathyroidism
At follow-up in June 2020, magnetic resonance imaging (MRI) showed a pathologic signal in the spine Th3-Th12 (arches and bodies). Whole-body bone scintigraphy was performed with technetium 99m-methyl diphosphonate (99mTc-MDP), and secondary bone lesions were confirmed. Whole body scintigraphy showed hyperfixation of radiotracer in the thoracic and lumbar spine bones, ribs, as well as in the right ileum bone (Figure 1). Diagnosis of distant metastasis to the bones was established and the patient was administrated paclitaxel 300 mg (6 courses) and 4 mg of zoledronic acid followed by radiotherapy. Radiation therapy of 40 Gy was administrated for residual parasternal lymph nodes, regional axillary and clavicular lymph nodes, whereas right breast was given 50 Gy. Three months later (September 2020), CT scan confirmed previously detected multiple bone lesions without signs of progression and the patient was administrated goserelin and tamoxifen (10 months from the baseline). In November 2020 (13 months from initial diagnosis and 3 months from the detection of bone lesions) the patient was evaluated with a whole-body CT scan, resulting in the identification of the well-circumscribed mixed density nodule near the left thyroid lobe (Figure 2) as well as multiple lesions to the bones. Evaluation of PTH revealed 137.2 pg/ml (normal range 18.8-88.0 pg/ml), Ca2+ 1.19 mmol/l (normal range 1.0-1.3 mmol/l), total calcium 2.52 mmol/l (normal range 2.18-2.6 mmol/l), albumin 45 g/l (albumin-adjusted total calcium 2.42 mmol/l), 25(OH)D 39.4 nmol/l (normal range >75 nmol/l). Given such results (normal calcium and low vitamin D), the elevation of PTH was considered as secondary to the vitamin D deficiency, and the patient was administrated 5600 U of cholecalciferol. This nodule near the thyroid gland was suspicious for PTA, but in light of subsequent laboratory investigations we had some doubts in diagnosis of PHPT, which was in line with practice guideline and our experience.5,11,12

Comparison of the whole body bone scintigraphy with technetium 99m-methyl diphosphonate before and after removal of parathyroid adenoma (View 1—anterior view of the skeleton, View 2—posterior view of the skeleton). (A) Scintigraphy was performed at baseline showing hyperfixation of radiotracer in the thoracic and lumbar spine bones, ribs, as well as in the right ileum bone. (B) At follow up (3 months after removal of parathyroid adenoma) scintigraphy showed decreasing number of bone lesions as well as decreasing of radiotracer uptake as compared to baseline.

Photograph of whole-body CT scan showing a well-circumscribed mixed density nodule posterior to the left thyroid lobe (the locations of the nodule are marked by arrows ). This lesion is separated by a thin tissue plane from the adjacent anatomical structures, including the left thyroid lobe ((A)—sagittal plane; (B)—coronal plane; (C)—axial plane).
The patient returned to our hospital in March 2021 with signs of cancer recurrence. The biopsy of right breast showed markedly atypical cells in comedo-type ductal carcinoma in situ. CT scan confirmed the presence of the mass near the thyroid gland and no changes in the bone lesions within 5 months from the previous check-up. Ultrasonography investigation showed left parathyroid gland 4.5 × 4.5 mm and right 5.5 × 4.7 mm (Figure 3). The blood tests revealed the following findings: PTH 95 pg/ml (normal range 18.8-88.0 pg/ml), Ca2+ 1.2 mmol/l (normal range 1.0-1.3 mmol/l), 25(OH)D 113 nmol/l (normal range >75 nmol/l), indicating normocalcemic PHPT. To further confirm PTA, scintigraphy with 99mTC-sestamibi was performed, resulting in the identification of a clear focus of strong signal in the area of the lower pole of the left thyroid lobe (Figure 4).

Ultrasonography illustration of the left parathyroid gland 4.5 × 4.5 mm in the largest diameter (marked with the rectangle).

Photograph of scintigraphy with 99mTC-sestamibi showing a clear focus of strong signal from the radiotracer in the area of the lower pole of the left thyroid lobe (indicated by the dotted ellipse).
Simultaneously, patient underwent parathyroid removal followed by bilateral mastectomy with immediate breast reconstruction with implants. Intraoperatively, an enlarged mass was identified near a low pole of the left thyroid lobe and laterally to the left recurrent laryngeal nerve, indicating left upper single parathyroid adenoma (PTA). Parathyroids autofluorescence signal was evaluated in near-infrared light by using Fluobeam-800 (Fluoptics, France) according to the previously described approach (Figure 5). 12 On the next day after the operation Ca2+ was 1.17 mmol/l and PTH 35.7 pg/ml. One month from the operation day, Ca2+ was 1.15 mmol/l and PTH 36.1 pg/ml. Postoperative histopathology confirmed 1.2 g chief-cell PTA. 2 months after the operation both PTH and Ca2+ were within normal ranges.
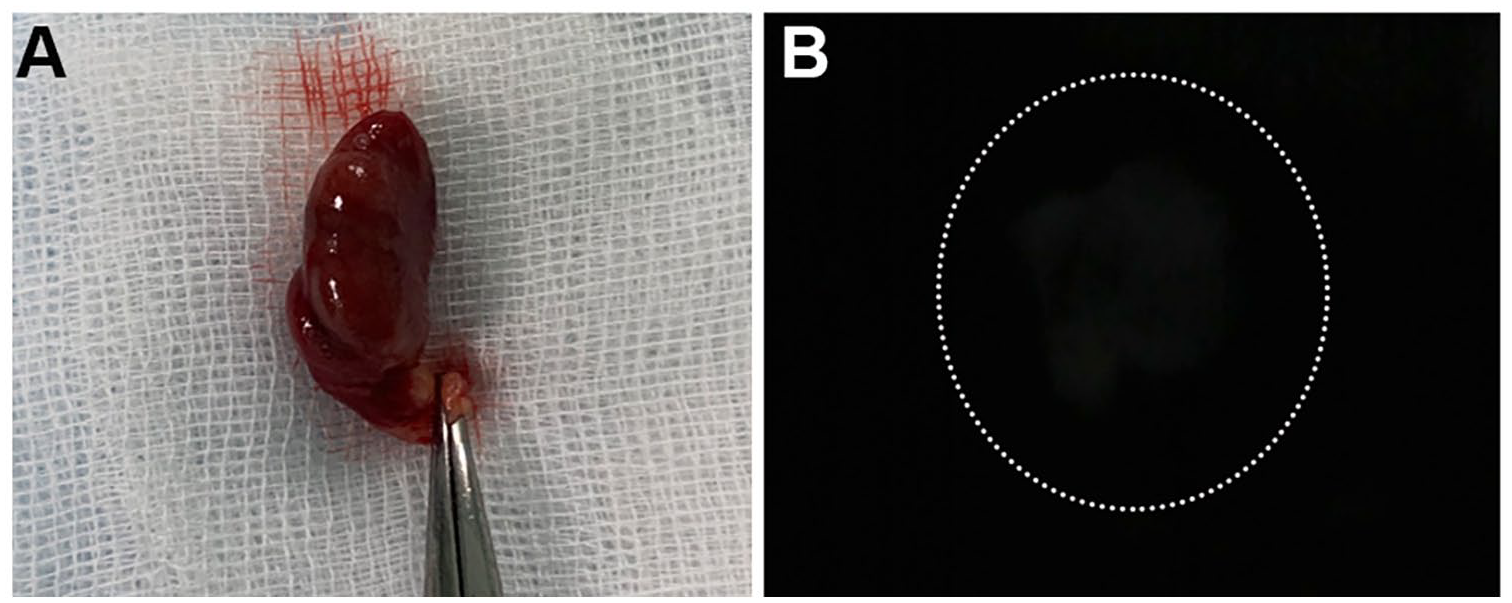
(A) Macrophotograph of the removed parathyroid adenoma of the left upper parathyroid gland under the room light. Photograph of the right parathyroid adenomas showing autofluorescence in near-infrared light. (B) Photograph of the parathyroid adenoma exhibiting autofluorescence signal in near-infrared light (marked with the dotted ellipse).
Follow up
During the follow up period, patients was received chemotherapy of goserelin and tamoxifen; bone lesions were treated by zoledronic acid, calcium carbonate and cholecalciferol. In October 2021 (4 months after parathyroidectomy), a whole body scintigraphy scan showed decreasing of multiple bone lesions as well as decreasing of radiotracer uptake in some spots, which is indicated improvement as compared to baseline (Figure 1). CT scan showed no difference in the bones lesions as compared to baseline measurements. Laboratory tests showed PTH 35.0 pg/ml, Ca2+ 1.24 mmol/l, 25(OH)D 91.4 nmol/l. In November 2021 (5 months after parathyroidectomy), dual-energy X-ray absorptiometry showed no signs of systemic bone density loss, however moderate osteopenia was detected in area of the left femoral neck (T-score −1.4) and forearm bones of both upper extremities (both T-scores −1.3).
In April 2022, patient was diagnosed with moderately differentiated (G2) ductal invasive right breast carcinoma of no special type (NST), indicating recurrence.
Discussion
This study demonstrates that an importance to consider other causes of bone lesions in patients with cancer, but not only metastatic spread. Therefore it is important to consider also PHPT, which is common endocrine disease with the average frequency 27 to 30 per 27 and 30 per 100 000 person-years 13 . Our study underlined the relationship between bone metastases from breast cancer and PHPT as well as the importance to investigate serum calcium and PTH in patients with suspicion of metastasis to the bones. The main massage from this case report is to consider diagnosis of PHPT in patients with elevated or normal serum calcium associated with bone lesions, but not to keep focusing on malignancy only. In our opinion, hypercalcemia is not considered frequently as a possible sign of hyperparathyroidism by oncologists, which is supported by published evidence. Furthermore, it is a clinical challenge to discriminate hypercalcemia and elevated PTH in breast cancer patient, because such metabolic changes in calcium metabolism might be a secondary to malignant progression. In this report, a diagnosis of PHPT was postponed due to several overlapping conditions such normal calcium (both ionized and albumin-corrected calcium as vitamin D insufficiency, possible bone metastases as well as medication by goserelin and tamoxifen. PHPT is demonstrated heterogeneity in clinical course, showing overlap of symptoms with other diseases including breast cancer. PHPT diagnosis was established by applying multidisciplinary approach of oncologist, radiologists and endocrine surgeon.
Although PHPT is frequently asymptomatic, it may suddenly progress and severe hypercalcemia could cause life-threatening complications such as severe arrhythmia. As showed by Khubaib et al 14 patient was opted for palliative care due to worsening metastatic breast cancer and PHPT with severe hypercalcemia.
The pathogenesis of PHPT co-occurrence remains controversial in patients with breast cancer. According to published literature, the possible cause of PHTP in patients with breast cancer could be prior neck or breast irradiation.15,16 Our findings are in line with Punda et al demonstrated various sides of PTA whereas, Woll et al showed strong correlation between the side of breast radiation therapy with the side of PTA occurrence.15,16
Bones are the most frequent site of breast cancer distant metastases and bone loss is frequently seen in patients under tamoxifen therapy.10,17 Therefore, detection of the bone loss in such patients is usually considered as disease-related, whereas secondary causes of osteolytic lesions receive low attention.17,18 Hilton et al and Filippiadis et al considered to perform a bone biopsy in case of metastases of breast cancer, however we avoided such a procedure because of technical limitation to detect tissue biomarkers which is in line with ESMO Clinical Practice Guideline.19 -21
Although the scan of the bone is a useful tool to detect osseous metastases from breast cancer, 22 in our case it was not consistent with metastatic spread, but with PHPT. Our findings are in line with others, suggesting performing PTH measurement in breast cancer patients with hypercalcemia.17,18,22
The well-known is that PTA could develop within hereditary diseases such as multiple endocrine neoplasia or hyperparathyroidism jaw syndromes. However, the coexistence of hyperparathyroidism with other non-endocrine malignancies might be escaped from clinicians as showed in this study. According to large epidemiological studies the most common association was detected between PHPT and breast cancer, indicating a negative role of increased calcium for the malignant transformations.2,23,24 Considering the relationship between the PHPT and breast cancer, the question remains unclear whether the first event is PHPT or it is a subsequent event after the breast cancer progression. Hypercalcemia is frequently diagnosed in patients with various cancers, possibly, due to deregulations of the cytokines, prostaglandins and, PTHrP. 2 Also, one should consider that administration of tamoxifen and goserelin may cause hypercalcemia in the patients with breast cancer, which were also applied as adjuvant therapy in our case. Although the mechanisms for tamoxifen flare hypercalcemia remain unclear, studies suggest it as a frequent complication of anti-estrogen therapy.7,25 On the other hand, osteolytic hypercalcemia is usually associated with decreasing PTH due to overproduction of PTHrP, resulting in calcium renal retention.2,3
Vitamin D deficiency might be considered as a risk for breast cancer and PHPT since this steroid hormone is associated with induction of apoptosis and negative impact on cancer cell proliferation.26,27 It is worth to mention, that vitamin D is usually decreased in overweight and obese people mainly due to metabolic alterations.27 -29 A low vitamin D was detected in our overweight patient followed by administration of 5600 U of vitamin D. Unfortunately, vitamin D and calcium were not examined at baseline in this study, therefore it is difficult to estimate the time of hypercalcemia appearance, which is a limitation. It is also worth mentioning that calcium has the properties of metalloestrogen and activates ERα, which is associated with a higher risk for the development of breast cancer. 30 Diagnosis of PHPT is also challenged in patients with bone disorders. For example, a giant cell tumor or brown tumor might mimic bone resorption due to PHPT.8,31
Conclusions
To sum up, our study emphasizes the importance to consider possible hyperparathyroidism in patients with breast cancer and hypercalcemia. In view of possible of misunderstanding of skeleton changes, routine evaluation of PTH is considered as a reasonable test in patients with breast cancer accompanied by bone lesions.
Footnotes
Acknowledgements
None.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MG—project conception and design, data collection, analysis, and writeup; AD—data collection, analysis, literature search, preparation of supplementary video, drafting of manuscript; DP—acquisition of data, analysis and interpretation of data, preparing of figures, literature search, writeup; KA—acquisition of data, analysis and interpretation of data, preparing of figures, literature search, writeup; YP—project conception and design, analysis, and writeup; VH—project conception, writeup; critical revision of manuscript, final approval.
Ethical Approval
Ethical approval has been exempted by our institution.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.