
Abstract
Crohn’s disease (CD) has an unknown etiology, but it has a genetic component. Many cases of familial CD have been reported. We describe a Kosovar Albanian family with 6 children, of whom 3 have CD: monozygotic twins and their sister. As far as we know, this is the first such report of CD within a Kosovar family.
Introduction
Around 2 million people worldwide are affected by CD (CD) which consists of chronic inflammations that affects any part of the gastrointestinal tract and mostly the terminal ileum and colon. The etiology of CD is not clear but it is thought to be of immunological, genetic and environmental components. 1 Several investigations supported the idea of the genetic factors have a role in the inflammatory bowel disease (IBD), taking into account the patients with IBD that have a family history with the disease, and the prevalence being higher in monozygotic twins than that in dizygotic ones. Also, The IBD occurrence and prevalence varies locally and ethnically.2 -4The risk between the first-degree relatives of individuals with IBD is 8 to 10 times bigger than of the general people. 5 Approximately 1 in 5 subjects with CD has reported having at least one affected family member. It has been observed that many families have more than one patient with CD, even though it is most likely to have either ulcerative colitis (UC) or CD particularly, mixed cases also can happen. Research of monozygotic and dizygotic twins indicates that genetic structure is a more dominant factor for CD than for UC. 6 Although, the concordance for IBD in twins being below 50% points out the importance of environmental factors in developing IBD.7 -9
Here we are presenting a Kosovar family of Albanian ethnicity with twins and a sister that has CD. As far as we know this is the first reported case of monozygotic twins and a sister from Kosovo.
Family Report
The family has 6 children, consisting of 4 girls and 2 monozygotic twin boys. They were born in a southern city of Kosovo and lived in the same household with their family. The twins both got married at the age of 25 and continued sharing the same household until a few years ago. There was no particular stressful event in the life of the family which could lead CD to appear. They have no positive family history of IBD. All of the 6 children share the same blood type, A negative. The twins are monozygotic as established by clinical observation. Genetic analysis for monozygotes has not been performed. None of the children underwent appendectomy or tonsillectomy. The parents are of Albanian ethnicity and do not have blood ties with each other (Table 1).
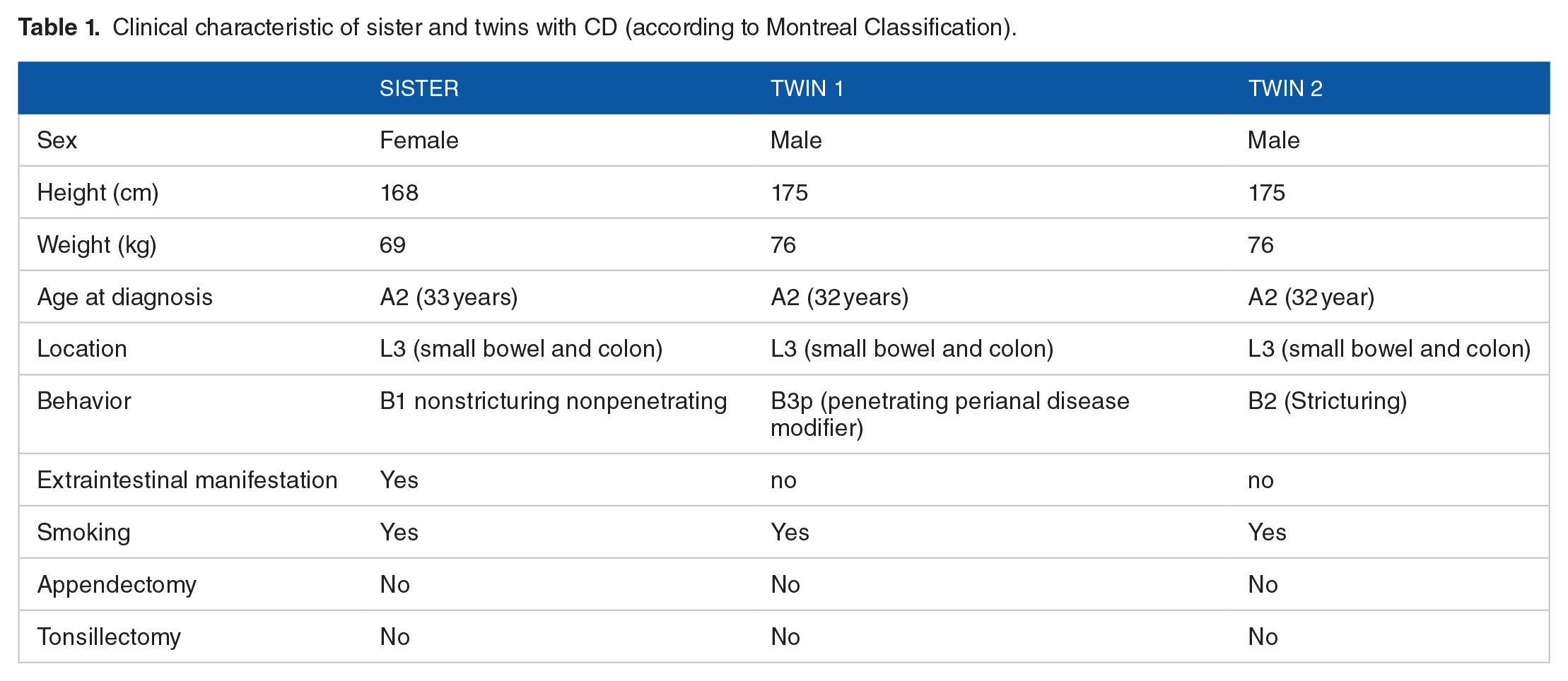
Clinical characteristic of sister and twins with CD (according to Montreal Classification).
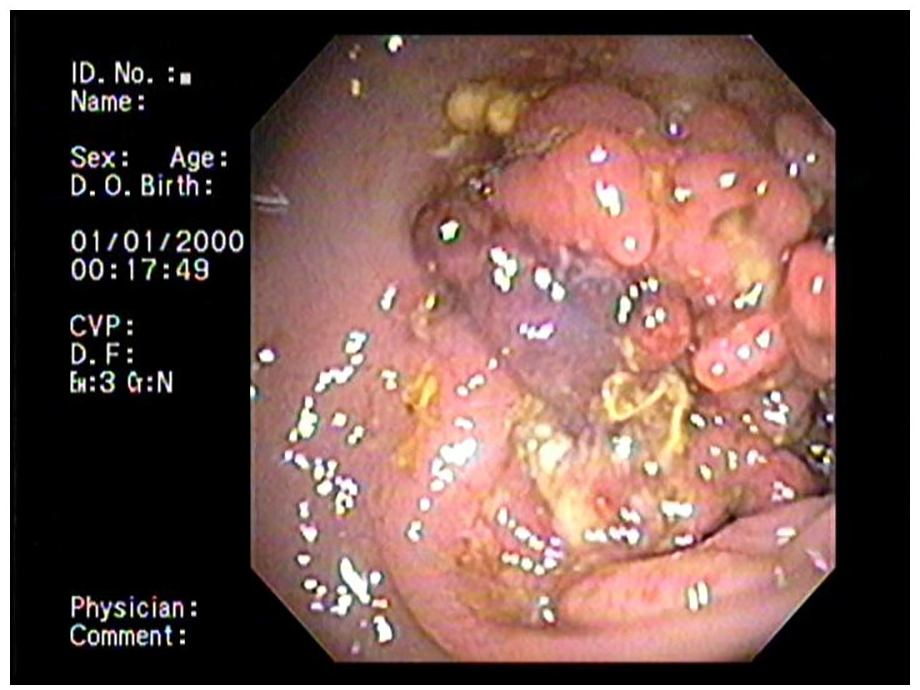
Colonoscopy of second twin. Mass at the level of splenic flexure.

Colonoscopy of second twin. Stricture at the level of splenic flexure.
Discussion
With a publication by Crohn et al. in 1932, CD was recognized as a separate entity from UC. 10 It has been uncovered in many reports prior to 1932 that describe CD (often by the name of “regional ileitis” or “regional enteritis”).11,12Kosovo lacks national registers and as a result much less is known about the incidence and prevalence of IBD in our country.
There have been numerous studies documenting the familial aggregation of IBD. The rate of patients with CD that report a family history of CD ranges between 2%and 14%, and of any type of IBD from 5% to 16%. While patients with UC, reporting a family history of UC ranges between 7%and 11% and any type of IBD from 8% to 14%. 8
Because of the familial clustering of IBD and predisposition of IBD incidence in Jewish people, particularly the Ashkenazim, it is suggested that IBD is inherited with genetic risk factors.13 -15The first report of familial clustering of IBD was done in 1930s. 16 Researches in which twins participated suggests that genetic structure is a more dominant factor for CD than for UC. The rate of concordance in monozygotic twins is as high as 67% for CD but only 13% to 20% for UC. 16 Most researches have pointed out the concordance of location and behavior of the disease, supporting the idea that there is a genetic factor to these attributes of the diseases.8,17
As for someother large European studies performed in Sweden,7,9 Denmark, 18 and UK, 17 the rate of concordance rate for CD in monozygotic twins was observed to be between 20% and 50%, whereas in dizygotic it is less than 10%.
Also the role of smoking habits was seen to influence the risk and phenotype in IBD according to twin studies.7,18 Orholm et al. observed that smoking had a mildly positive impact although non-significant in relation with CD, and significantly negative in UC. 18
Smoking is thought of as a strong environmental component influencing the acquisition of the disease type. 19
According to 6 twin studies performed in Europe, the proband concordance of CD turned out to be 30.3% between 112 pairs of monozygotic twins and 3.6% in 196 pairs of dizygotic twins suggesting that genetic components have a role in acquisition of IBD.20,21
In the Western Europe, approximately 5% to 22% of subjects with CD and 6% to 15% of subjects with UC had reported family history of IBD. 22 In first degree relatives of individuals with CD, the lifetime risk of IBD was 7.8% in Jewish people and 4.8% to 5.2% in non-Jewish people. In a epidemiological research done in Denmark between the years 1977 and 2011, the CD risk of first-degree relatives of patients with CD and UC resulted to be 7.77 and 4.08. 23
Another research done by Thompson et al. in British twins, also suggested similar results between monozygotic twins. 17 Furthermore, the concordance between UC and CD among twins is different. A study done on a Swedish twin pair resulted in higher concordance rate of 50% for CD than for UC, which was 18.8%) suggesting that inheritance and genetic factors is higher in CD than in UC.10,11,13
We should mention that the subjects in our study has no record of family history of inflammatory diseases of their parents. None of the parents have ever smoked. As for the age of onset, 3 of the subjects are diagnosed around the same age (32-33 years old). It should be taken into account that the sister was diagnosed with CD 2 years after moving out of Kosovo, which does not exclude the influence of any environmental factor, while the twins were both diagnosed in Kosovo. It is noteworthy to point out that the age of onset of CD in the 3 of the subjects was 32 to 33 years old (A2 According to Montreal classification). All of the subjects share the same location (ileocolonic L3), as for the behavior of the disease, the sister is B1 with non-stricturing and non-penetrating. The first twin had ileosigmoid and perianal fistulas, for which he was operated 6 times (B3p). And lastly, the second twin with strictures at the level of lienal flexures (Figure 2), is categorized as B2. It is important to mention that 3 of the subjects have been and continue smoking cigarettes, contrary to the doctor’s advice to quit. As for the extraintestinal signs, only the first subject (sister) had seronegative arthritis. Currently, none of the subjects’ children have any complaints related to IBD.
Throughout this research, we encountered a family report of an Albanian family who migrated to Greece, that has 3 children with CD, consisting of one son and a pair of twin sisters. 14
The genetic studies over the last 2 decades have pointed out many potential genetic loci that may have a role in the pathogenesis of IBD. 24
Genetic variations in the ATG16L, NOD2/CARD15, and IL23R genes have strongly been linked to the onset of CD. 25 Due to technical difficulties, we were not able to conduct genetic testing.
As the occurrence and prevalence of CD increases, deeper studies on the etiology and pathogenesis of CD and related genes are necessary.
We plan to contact one of the leading centers in IBD genetics to enable establishing of a molecular diagnosis through whole-genome sequencing
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
ST, AV, MS, MT, HF, FA made a substantial contribution to the concept or design of the work.MT, HF made analysis and interpretation of data.ST, FA, AV drafted the article and revised it critically for important intellectual contentST, AV, MS, MT, HF and FA approved the version to be published and did the agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.