
Abstract
Spontaneous uterine rupture is a catastrophic obstetric complication for both the mother and fetus. We highlight a case of a 32-year-old G2P1A0L1 Hispanic female at 36 weeks gestation who presented to the labor and delivery unit with minimal prenatal care, complaining of abdominal pains and vaginal bleeding. An abdominopelvic ultrasound confirmed an empty uterus and fetal demise in the abdominal cavity, leading to an exploratory laparotomy to evacuate the fetus. At surgery, a preterm sized fetus “en caul” with intact amnions was floating in the abdominal cavity and a hemostatic, complete rupture of the anterior uterine wall was discovered. Uterus was repaired and the patient recovered postoperatively without complications. Despite the best evidence suggesting that a history of low-transverse Cesarean section poses a low risk for spontaneous uterine rupture, this complication should always be considered and patients should be counseled regardless of the low risk should they desire a cesarean section.
Introduction
Spontaneous uterine rupture is a rare and potentially catastrophic obstetric complication that has been associated with maternal mortality, fetal demise, postpartum hemorrhage, and the need for Cesarean hysterectomy. 1 A complete uterine rupture is defined as a full thickness tear of the uterine wall, which includes both the myometrium and uterine serosa that occurs during pregnancy or delivery. 2 In a systematic review designed by the World Health Organization (WHO) in 2005, the authors estimated the worldwide prevalence of uterine rupture with a history of previous Cesarean section (CS) to be around 1%. 3 The prevalence varies from country to country with the less and least developed countries having a higher prevalence and worse outcomes when compared to higher income countries. 3
As a rare complication, the diagnosis of uterine ruptures are typically done intraoperatively or during labor. This complication is rather insidious and careful evaluation of the patient and the fetus, as well as access to basic obstetric care is crucial in determining maternal and perinatal outcomes. 2 In the following case report, we describe a preterm pregnancy complicated by an asymptomatic but complete uterine rupture with “en caul” expulsion of the fetus in the patient’s abdominal cavity.
Case Presentation
A 32-year-old G2P1A0L1 Hispanic female at 36 weeks gestation presented to the Labor and Delivery unit after 48 hours of minimal abdominal pain, vaginal bleeding, and no perceived fetal movement. Prior to admission, she was at home with a doula attempting an unsupervised delivery but after being unsuccessful, came to the Labor and Delivery unit. Her past obstetric history included a previous low-transverse CS for breech presentation, birthing a healthy neonate at 39 weeks. For the current pregnancy, prenatal obstetric care was minimal and only an ultrasound at 20 weeks was performed which revealed normal fetal anatomy and confirmed gestational age. Additional pertinent medical history included smoking 5 to 6 cigarettes a day. At the time of presentation during triage, an abdominopelvic ultrasound examination revealed an empty uterus and fetal demise in the abdominal cavity, which prompted to a subsequent emergent exploratory laparotomy to evacuate the fetus. During surgery, an at-term size fetus “en caul,” involving intact amnions with the fetus in the sac and the entire placenta attached, was floating in the abdominal cavity. A non-actively bleeding, complete rupture of the anterior uterine wall on the previous scar from cesarean delivery was discovered. After completing the delivery of the fetus, the uterus was repaired in a usual fashion with double imbricating delayed absorbable sutures. Total blood loss from the procedure was 1200 ml. The patient recovered well postoperatively with no complications (Figure 1).
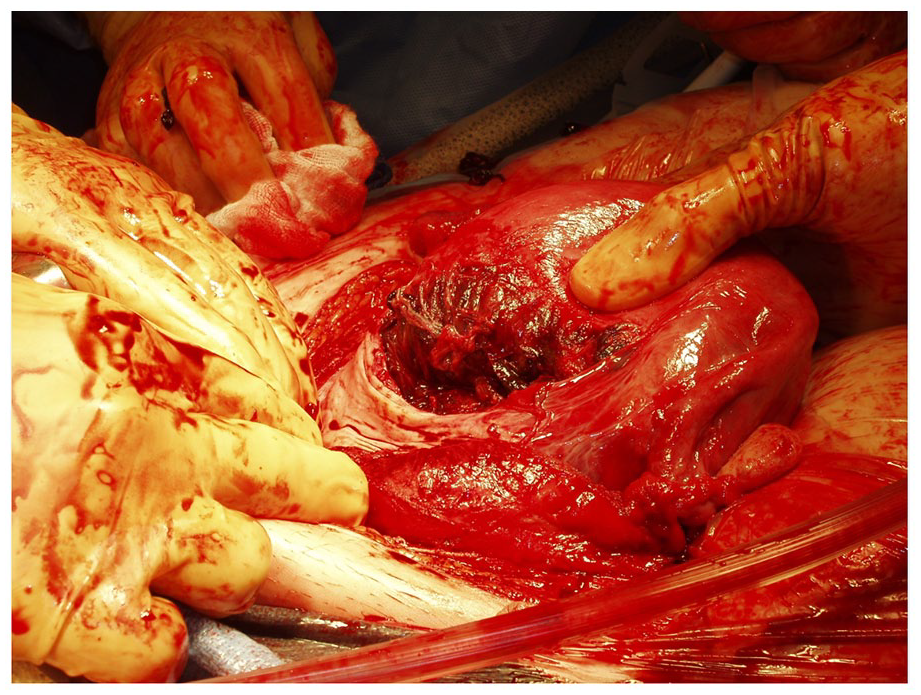
The evacuated fetus during the exploratory laparotomy procedure. The fetus is encased in its amniotic sac.
Discussion
Although presenting signs of uterine rupture can include extreme abdominal pain, vaginal bleeding, loss of fetal station, and fetal distress, patients can present with incomplete ruptures, scar dehiscence, be asymptomatic or with vague and common complaints seen every day in obstetric triage. 1 Other more common obstetric complaints such as decreased fetal movement or vaginal spotting should always be taken seriously and appropriately worked up due to the possibility of an emergent or life-threatening condition arising.
There are 2 main classifications of uterine rupture including complete rupture and incomplete rupture. Complete rupture involves the full thickness of the uterine wall and includes all 3 layers of the uterus. 2 Complete uterine rupture typically presents with the more classic, severe symptoms of uterine rupture and leads to worse outcomes. Incomplete uterine rupture occurs when the visceral peritoneum of the uterus remains intact and typically presents as a less severe and typically asymptomatic dehiscence of an existing uterine scar. 1 The occurrence of scar dehiscence can be benign in nature and can even occur following a vaginal delivery, often times going undiagnosed. 1
It is worth noting that primary CS rates are increasing worldwide. In a paper recently published by Beorma et al they estimated that the average annual rate of CS usage globally increased by 3.7% during the years 2000 to 2015, which was observed in all regions in the world. 4 These increasing rates of CS section likely contribute to the uptick in incidence of uterine ruptures worldwide.2,4 However, it is crucial to highlight that uterine ruptures in less developed countries continue to be a major cause of maternal death as there is a striking difference in perinatal and maternal outcomes when comparing developed and less or least developed countries. 2 This disparity in outcomes exists due to limited access to healthcare in developing countries where hospitals or personnel are not readily available to diagnose early, treat and have the means to manage patients with uterine ruptures effectively. 2
The overall risk for uterine rupture and serious adverse perinatal outcome (stillbirth, hypoxic ischemic encephalopathy, neonatal death) at term after cesarean birth is 0.32% and 0.27%, respectively. 5 The most important risk factor for uterine rupture is a scarred uterus, generally from a previous CS. More specifically, a previous classical CS involving a vertical uterine incision is more likely to cause uterine rupture (2%-9%) and result in more serious complications when compared to a CS involving a low-transverse hysterotomy (0.2%-0.9% for one previous and 0.9%-1.8% for multiple previous). 6
Trial of Labor after Cesarean (TOLAC) is still recommended and routinely offered to patients who have had one previous low-transverse CS, but continuous monitoring of the mother and fetus is required. 7 Some interventions that are routinely done in a normal induction of labor can increase the risk of uterine rupture, including the use of misoprostol, a commonly used prostaglandin E1 containing medication that is contraindicated during TOLAC due to the higher risk of uterine rupture. 8 One large prospective observational study involving nearly 34 000 women showed that this increased risk of uterine rupture during TOLAC was 1.4% for induction with prostaglandin containing drugs with or without oxytocin, 1.1% for oxytocin alone, 0.9% for augmented labor, and 0.4% for spontaneous labor. 9
Rupture of an unscarred uterus is extremely rare but with multiple risk factors can be more likely to occur. Risk factors for uterine rupture can include factors that are common in obstetrics including short interval pregnancies (pregnancy that occur less than 18 months after previous delivery) and labor interventions including the use of oxytocin or prostaglandin containing medications. Other less common risks include multiple gestations, abnormal placentation, or uterine anomalies. Traumatic origins that can lead to uterine rupture can include external trauma from falls or motor vehicle accidents, obstetric maneuvers such as internal or external cephalic versions, 10 or congenital disorders affecting tissue strength such as Ehlers-Danlos type IV. 10
Conclusion
Uterine ruptures can present in many ways and should always be considered as a possibility in obstetrics, especially in those who have previously had a CS. With the rates of CS increasing globally, the incidence of uterine rupture increases and continues to be a devastating complication in lesser developed countries due to their lack of access to proper management and obstetric care. Although there is an increased risk of uterine rupture for those who attempt a TOLAC, the best evidence suggests that the absolute risks are low in those with one previous low-transverse CS, as long as the trial of labor is taking place in a unit with continuous coverage with an obstetrician and anesthesiologist on site. Those who still desire to attempt a TOLAC should be given the opportunity but must be counseled extensively on the risk of uterine rupture and subsequent outcomes.
Footnotes
Acknowledgements
We are grateful to the Texas Tech University Health Sciences Center, Permian Basin, TX, and Kushal Gandhi and Nathan Joshua Manales at the TTUHSC-PB Research Lab for their excellent support on this case report in revising and editing.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contribution
Gary Ventolini was in charge of the patient’s care and obtained patient consent. Gary Ventolini, Suna Burghul, and Stanley Eboh designed the case report. Suna Burghul, Stanley Eboh, MICHAEL Galloway, Asley Sanchez, and Gary Ventolini contributed in the writing and editing of this manuscript. All authors have approved the submitted version. Suna Burghul and Stanley Eboh contributed equally.
Consent
An informed written consent was obtained from the patient for the publication of this case report and image.
Statement of Ethics
The authors have no ethical conflicts to disclose. The authors certify that they have all obtained all appropriate patient consent forms.
Disclosure Statement
The authors have no conflicts of interest to declare. The work described in this case report has not been published previously, is not under consideration for publication elsewhere, and has been approved by all authors responsible for the work carried out.