
Abstract
Background:
Osteochondromas are a relatively common primary bone tumor, which may share common clinical features with Osgood-Schlatter disease (OSD). A limited number of cases have described tumors misdiagnosed as OSD.
Case Presentation:
We report the case of an 11-year-old male with a sessile osteochondroma of the tibial tubercle and concomitant involvement of the distal extension and attachment of the patellar tendon into the tibial periosteum. A prior diagnosis OSD had been made. The lesion was resected and repair of the extensor mechanism was required at the time of surgery. The patient was followed for 20 months postoperatively and had restoration of knee function with minimal pain, as demonstrated by a PEDI-IKDC score of 94.6 at 19-month.
Conclusion:
This is a rarely reported case of benign tumor masquerading as OSD requiring excisional biopsy with extensor mechanism repair.
Introduction
Osteochondromas are a relatively common primary bone tumor, often arising from the metaphyseal portions of long bones with the majority of these being solitary lesions. 1 Osteochondromas are usually asymptomatic, and are most frequently detected in adolescent males. 2 Most common reasons for surgical excision of the mass include pain, cosmetic appearance, pressure on adjacent structures, limitations in range of motion, pathologic fracture of the mass, and occasionally malignant transformation. 3
Osteochondromas may share common clinical features with Osgood-Schlatter disease (OSD). OSD is a common cause of anterior knee pain in adolescents, more frequently affecting males and athletes. 4 It is a traction apophysitis of the tibial tubercule caused by a repetitive strain on the tibial tuberosity.4,5 Conservative management of OSD includes rest, icing, and activity modification. Operative treatment is rarely warranted given that OSD is self-limiting. However, more severe cases may require excision of bony ossicles. 5
A limited number of cases have described tumors misdiagnosed as OSD.6 -8 Herein, we report a case of an adolescent proximal tibia osteochondroma with concomitant involvement of the distal extension and attachment of the patellar tendon into the tibial periosteum, and a clinical presentation mimicking OSD.
Case Report
An 11-year-old male presented to clinic with a large anterior bony prominence just distal to the tibial tubercle of his right knee. The patient was athletic and recently began experiencing pain over his proximal tibia with physical activity. Approximately 4 years prior, the patient presented to another orthopedic surgeon with concern about the bony prominence. He was diagnosed with severe OSD and an MRI demonstrated chronic osteochondrosis distal to the tibial tubercle with an overlying bursa. The patient was treated conservatively at that time without resolution of the prominence.
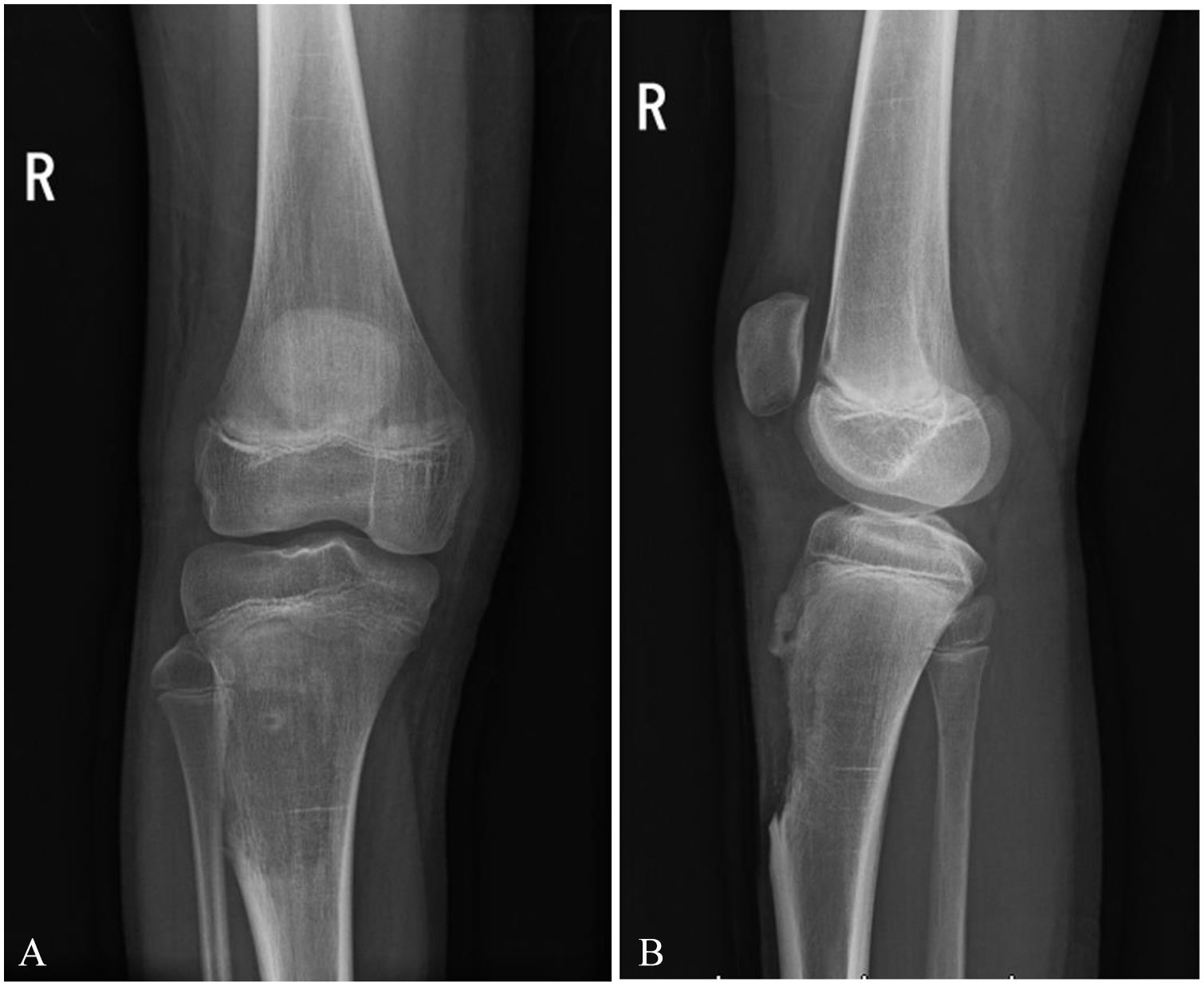
On physical examination, the prominence was not tender to palpation. Full and painless range of motion was observed for the hip, knee, ankle, and toes, and sensorimotor function was intact distally throughout the lower extremity. X-ray demonstrated a possible osteochondroma of the proximal right tibia (Figure 1A and B). MRI confirmed the diagnosis and revealed that the patellar tendon partially inserted on the osteochondroma as well as the tibial tubercle (Figure 2A and B). Given that the mass appeared to be growing in size and the patient was progressively symptomatic, it was decided that surgical excision would be the most appropriate treatment (Figure 3).

Preoperative findings on X-ray. Plain radiographs showing the anteroposterior (A) and mediolateral (B) views of the right knee.

Preoperative findings on MRI. MRI showing the sagittal (A) and axial (B) views of the right knee.

Pre-operative image of large anterior bony prominence just distal to the tibial tubercle of the patient’s right knee.
A total resection of the mass was performed using an anteromedial approach. An incision spanning 3 inches was made. Local soft tissue from the proximal tibia was dissected. A dissection was also performed on the portion of the patellar tendon that was attached to the anterior tibial mass. The mass was demarcated using a combination of anatomic parameters and C-arm fluoroscopy while taking care not to violate the physis. The mass was resected with a combination of osteotomes and a rongeur. Bleeding was mitigated with bone wax and cautery. The distal insertion of the patellar tendon was then reattached to the bone of the tibia with a suture and anchor technique. The repair was evaluated with motion of the patella, which was found to be excellent and stable. Patellar height was found to be equivalent compared to the contralateral side. Wound irrigation and closure were followed by a sterile dressing and a brace that was locked in extension. Dimensions of the resected mass were 5.0 cm × 4.0 cm × 2.0 cm (Figure 4A). Pathology confirmed that the mass was a benign osteochondromatous proliferation, with irregular architecture and immature cartilage giving rise to disorganized woven bone (Figure 4B and C). Additional areas of reparative changes were suggestive of fracture callus. These histopathology findings were distinct from those expected in OSD, although OSD also presents with changes in fibrocartilaginous tissue.

Dimensions of the resected mass were 5.0 cm × 4.0 cm × 2.0 cm (A). Hematoxylin and eosin staining of disorganized, woven bone with immature cartilage, and irregular architecture on 4× (B) and 10× magnification (C).
Postoperatively, the patient was instructed to abstain from athletics for 8 to 10 weeks. At his 2-week postoperative visit, the patient was observed to be compliant with non-weightbearing and mobilizing with a wheelchair. Range of motion in the knee brace was increased, and the patient was permitted to toe-touch. Given that the patient had difficulty adjusting to crutches, physical therapy was prescribed to increase weight-bearing capacity. At the 5-week follow-up, the patient had intact straight leg raise and was able to bear weight as tolerated in the brace. Range of motion in the knee brace was subsequently increased from 0° to 90°. At the 8-week follow-up, knee range of motion was 0° to 120° without discomfort. Bracing was discontinued given that the patient was observed to bear weight as tolerated and the radiographs showed no concern for fracture (Figure 5A and B). The patient was instructed that he may resume some sports activities (eg, shooting baskets) but should avoid competitive or gym activities until fully cleared. At the 16-week follow-up, range of motion further increased to 130° without discomfort, and the patient was instructed to resume activities. At the 19-month follow up, patient had full resumption of athletic activities and experienced minimal pain. Radiographs demonstrated progressively healing tissue in surgical site evident by remodeling in the area of the lesion inferior to the tibial tubercle (Figure 6A-C). Clinical examination showed fully healing of the incision without any recurrence of the anterior mass (Figure 7). The patient’s PEDI-IKDC 9 score at approximately 19-month post-operatively was 94.6.
Findings on X-ray 2 months postoperatively. X-ray showing the anteroposterior (A) and anteromedial (B) views of the right knee.

Findings on X-ray 19 months postoperatively. X-ray showing the standing hips-to-ankles view (A), left lateral (B), and right lateral (C) views with increased cortical density in the area of anterior resection without recurrence.

At 19-month post-operatively, clinical examination showed fully healing of the incision without any recurrence of the anterior mass.
Discussion
Osteochondroma and OSD may present with overlapping clinical features. Both conditions typically occur in adolescents with knee pain, although osteochondroma is more frequently asymptomatic. OSD is more likely to occur in athletes who engage in sports that require repetitive contraction of quadriceps muscles, causing undue stress on the tibial tubercule. 10 OSD is therefore frequently symptomatic with physical activity. OSD may present bilaterally in up to 30% of patients. 11 Unlike OSD, osteochondroma affects the tibia and humerus in only 10% to 20% of cases, with the femur being the most common site. 12 Though OSD is typically a self-limiting overuse injury, osteochondroma may progress in size and lead to complications including pathological fracture, neurovascular impingement, bursa formation, and malignant transformation in 1% of patients. 12
There is a limited number of cases describing osteochondroma mimicking OSD. Balaji et al 6 described a case of an adolescent male presenting with swelling over his right proximal tibia with associated pain. Unlike our case, the patient also experienced pain on physical exam with knee flexion and extension. Surgical excision was performed, and the patient was asymptomatic at final follow up. Similarly, Vancauwenberghe et al 7 reported a case of a periosteal chondroma in an adolescent female with no associated pain and successful treatment with surgical excision. The clinical presentation suggested that the absence of pain was an indicator against OSD. Jamshidi et al 8 described 11 cases of benign tumors mimicking OSD, of which 3 were eventually diagnosed as osteochondroma. The 3 cases with osteochondroma did not present with associated pain. Jamshidi et al described a treatment algorithm for differentiating benign tumors from OSD, including the following characteristics in favor of a benign tumor: lack of pain, progressive pain and bump, activity-independent pain, a bump size greater than 5 cm2 at presentation, and age fewer than 10 years. 8 Our case did not meet all of the criteria for benign tumor, notably the requirement for absence of pain and age less than 10 years, suggesting complexity in differentiating osteochondroma from OSD.
A 3 to 8 years follow up of surgical outcomes with resection of symptomatic osteochondroma suggested resolution of preoperative symptoms in 93.4% of patients. 13 Major complications occurred in 4.7% of patients, including intra-operative fracture and nerve palsies that resolved with decompression. 13 Our case presented a challenging resection given the concomitant involvement with the extensor mechanism. Tumor resections that require more complicated reconstructions are associated with decreased postoperative function and stability of the knee joint. 14 Despite the complexity of reconstruction, our case experienced a successful outcome, as indicated by the optimal PEDI-IKDC 9 score and resolution of symptoms at 19-month post-operatively.
In summary, we report a case of an adolescent male with osteochondroma in the proximal tibia, originally misdiagnosed as OSD given similarity in clinical presentation. To the author’s knowledge, this is the first such case involving repair of the extensor mechanism with assessment of functional outcome using the PEDI-IKDC 9 score on longitudinal follow-up. These findings suggest the clinical complexity in differentiating osteochondroma from OSD, and that radiographic findings may be difficult to interpret early in presentation. Surgical excision of osteochondroma should be considered for symptomatic patients.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors participated in conception, analysis, interpretation, drafting, and critical revision of the manuscript.
Ethics Approval and Consent to Participate
Waived.
Consent for Publication
The patient and his parents consented to submission of data concerning the case for publication.