
Abstract
Keywords
Key Points
Flexibility athletes are a unique patient group where sport-specific movement demands an increased hip ROM compared to non-flexibility athletes.
Flexibility athletes successfully regained range of motion 1-year after periacetabular osteotomy for the treatment of symptomatic hip dysplasia.
Flexibility athletes fully regained external rotation, a key component to turnout stance, by the 1-year postoperative time point.
Introduction
Periacetabular osteotomy (PAO), a well-established surgical intervention for the treatment of hip dysplasia, corrects acetabular under-coverage by reorienting the acetabulum in multiple planes.1 -3 Hip dysplasia is characterized by under-coverage of the femoral head by the acetabulum. Although infants are screened at birth, some patients are not diagnosed until adolescence or early adulthood.1 -3 Treatment of patients diagnosed in adolescence or adulthood may initially be a course of physical therapy,4,5 but one study found that nearly 60% of patients progressed to PAO after conservative management. 4 After PAO, patients demonstrate significant improvements in hip pain and functionality. Active patients who undergo PAO typically return to sports and activities at or above their preoperative level.6 -8 A recent study of young female dancers found that approximately two-thirds of the participants returned to dance at an average of 8.8 months after PAO with overall improvement in hip pain and function. 9 However, few studies have investigated range of motion (ROM) outcomes in flexibility athletes—such as dancers, gymnasts, and cheer athletes—who undergo PAO.
Flexibility sports require a higher degree of hip flexion, extension, abduction, and external rotation (ER) compared to non-flexibility sports.10 -12 In combination, these extremes of hip ROM can place increased tension on the labrum. 13 Furthermore, actions and positions that incorporate front and side splits can lead to hip impingement and even mild subluxation. 14
Considering these unique demands placed on the hip, knowing whether these athletes are expected to regain their preoperative hip ROM after PAO could help set expectations for recovery or in clinical decision-making. Our study had 2 primary objectives. First, we examined if young flexibility athletes who undergo PAO for hip dysplasia recovered their baseline hip ROM within 1 year of surgery. Second, we evaluated if hip ROM recovery after PAO differed between flexibility athletes and non-flexibility athletes. We hypothesized flexibility athletes would have decreased hip ROM 1 year after surgery compared to preoperative ROM. We also hypothesized that non-flexibility athletes would recover their baseline hip ROM sooner than flexibility athletes.
Methods
Participants
We conducted a retrospective case-control analysis of data collected from a registry of patients with hip pathology, ages 10 to 25, treated with PAO for a primary diagnosis of symptomatic hip dysplasia at a single institution between January 1, 2016 and December 31, 2019. Some patients had additional diagnoses including labral tear (n = 6) and abductor dysfunction (n = 8), though these diagnoses did not impact their treatment approach. Patients included in the group of interest were self-identified flexibility athletes—dancers, cheer athletes, or gymnasts. Patients included in the comparison group were self-identified volleyball players, basketball players, swimmers, or track and field athletes. Patients were excluded if they had a history of prior ipsilateral hip surgery, underlying neuromuscular or musculoskeletal condition, or did not self-identify as an athlete in one of the previously noted sports. All data collected in this study was performed as clinical standard of care. However, consent was obtained from each patient at their initial visit so that their data may be de-identified and used for future research. The local institutional review board approved of this study prior to commencement.
Study Design
Our primary ROM variables included hip flexion, internal rotation (IR), and external rotation (ER). ROM measurements were visually assessed by a board-certified orthopedic surgeon, with the patient supine and the ipsilateral knee flexed to 90°. Measurements were obtained at the preoperative visit and consecutive postoperative visits for at least 1 year. Once ROM was measured within 5° of preoperative ROM in a specific plane, patients were deemed to have recovered their baseline ROM. We allowed for 5° of variability because measurements were assessed visually, rather than with a measurement tool such as a goniometer.
Patient Classification
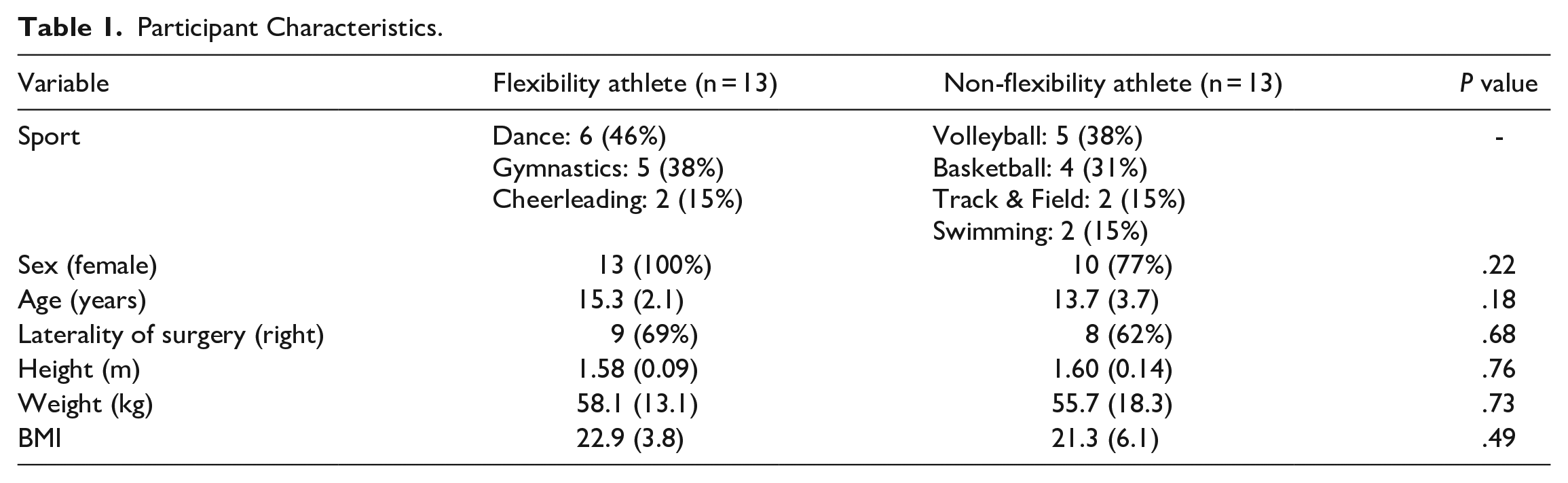
Upon initial evaluation in clinic, all patients were asked to complete a new-patient questionnaire which included listing the sports and activities they were actively involved in. Although this is part of the standard clinical care, patients are made aware that this data will be de-de-identified and may be used in future research. As such, all patients are given the opportunity to opt out of completing these questionnaires. Patients who self-identified as dancers, gymnasts, or cheerleaders were classified as flexibility athletes. Patients who self-identified as volleyball players, basketball players, track and field athletes, or swimmers were classified as non-flexibility athletes. In total, we included 13 flexibility athletes and 13 non-flexibility athletes (Table 1).
Participant Characteristics.
Statistical Analysis
Data are presented as means (standard deviation) for continuous variables or the number included (corresponding percentage) within group for categorical variables. We compared the percentage of flexibility and non-flexibility athletes who regained preoperative flexion, IR, and ER within 5° 1 year after surgery. For patients who were not seen exactly at 1-year post-operation, we chose the soonest visit after that time point. We compared the time to recovery (days) between groups in each ROM plane using Mann Whitney U tests, given the nonparametric distribution of the data. We then compared the proportion of participants in each group who demonstrated full ROM recovery in each movement plane at 1-year post-op. Finally, we used a series of 2 × 2 repeated measures analyses of variance (ANOVAs) to examine the effects of time (pre-operative vs 1-year post-operative) and group (flexibility vs non-flexibility), and the interaction between these 2 variables. Significance was determined using an alpha level of P = .05. All statistical analyses were 2-sided and performed using Stata version 15 (StataCorp, College Station, TX, USA).
Results
We evaluated the preoperative and postoperative hip ROM for 13 flexibility athletes and 13 non-flexibility athletes who underwent PAO for symptomatic hip dysplasia. In the flexibility athlete group, we included self-identified dancers (n = 6), gymnasts (n = 5), or cheerleaders (n = 2). They were 15.3 years old on average, and 100% were female. In the non-flexibility athlete group, we included self-identified volleyball players (n = 6), basketball players (n = 4), track and field athletes (n = 2) or swimmers (n = 2). They were 13.7 years old on average, and 77% were female (Table 1).
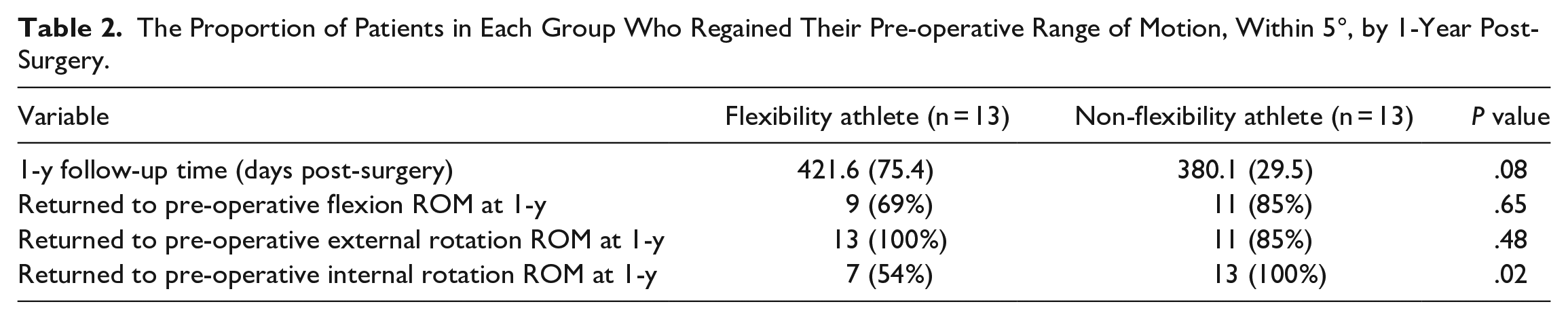
One-year follow-up data was collected at approximately 13 to 14 months postoperatively in both groups (Table 2). A higher percentage of non-flexibility athletes regained baseline flexion at approximately 1 year, but this was not statistically significant. (Table 2). However, a significantly higher percentage of non-flexibility athletes regained preoperative IR at approximately 1 year (Table 2). All (100%) flexibility athletes regained preoperative ER at 1 year compared to 85% of non-flexibility athletes (Table 2).
The Proportion of Patients in Each Group Who Regained Their Pre-operative Range of Motion, Within 5°, by 1-Year Post-Surgery.
The difference in the time to ROM recovery between groups for flexion, IR, or ER was not significant (Figure 1). For ER, we observed a main effect of time, where patients in both groups demonstrated significantly higher ER ROM at the 1-year post-operative assessment compared to the pre-operative assessment (Figure 2; P = .003). We observed a significant time × group interaction for IR ROM (Figure 2; P = .046). Although no differences between groups existed pre-operatively, by 1-year follow-up, non-flexibility athletes had significantly higher IR ROM than flexibility athletes (mean difference = 7.1 degrees; 95% CI = 0.3, 14.0; P = .036).
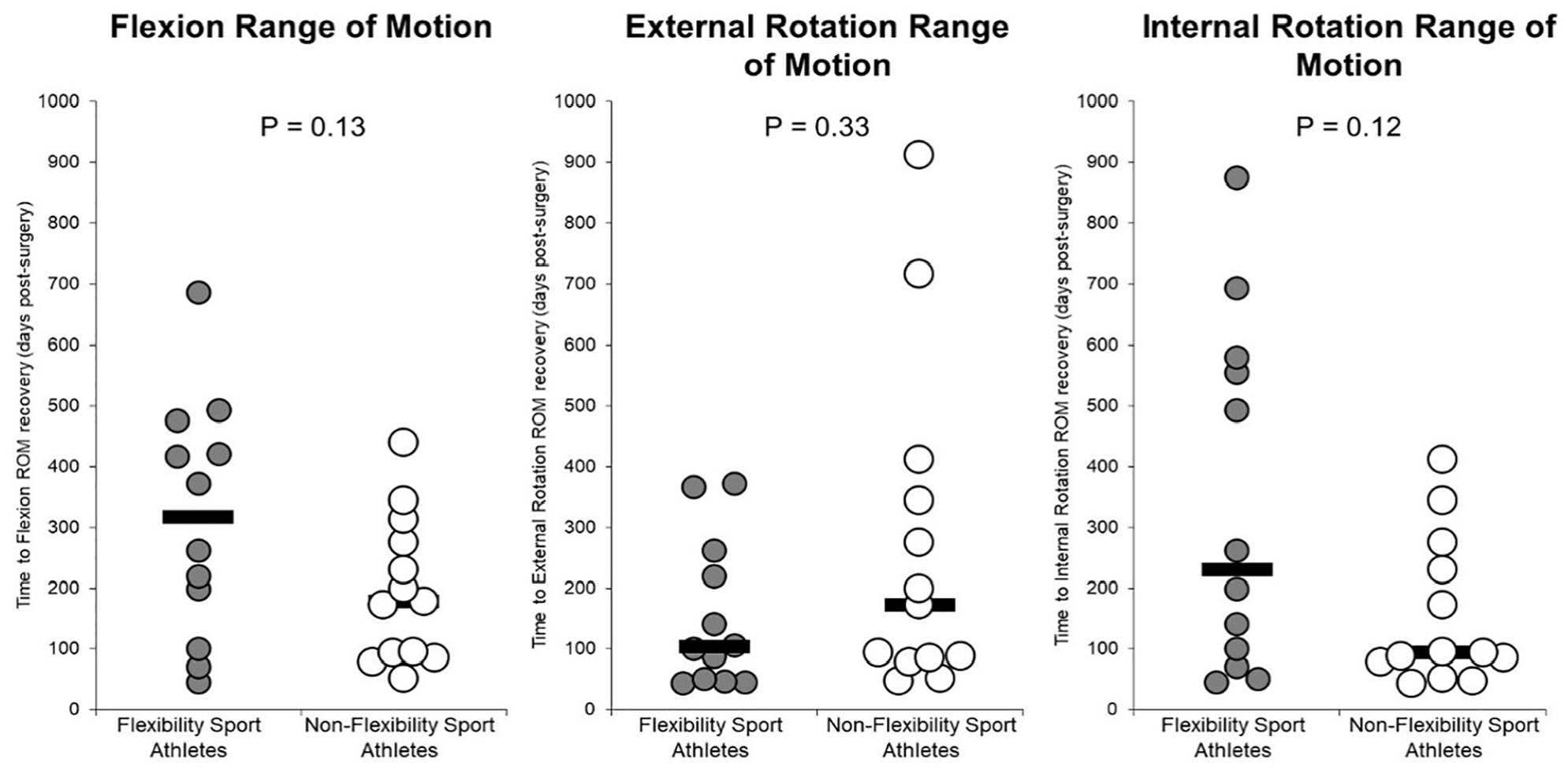
Time required from surgery until the first observation of returning to pre-operative range of motion, within 5°, among flexibility and non-flexibility athletes. Each dot represents and individual patient, black bars represent the group median value.
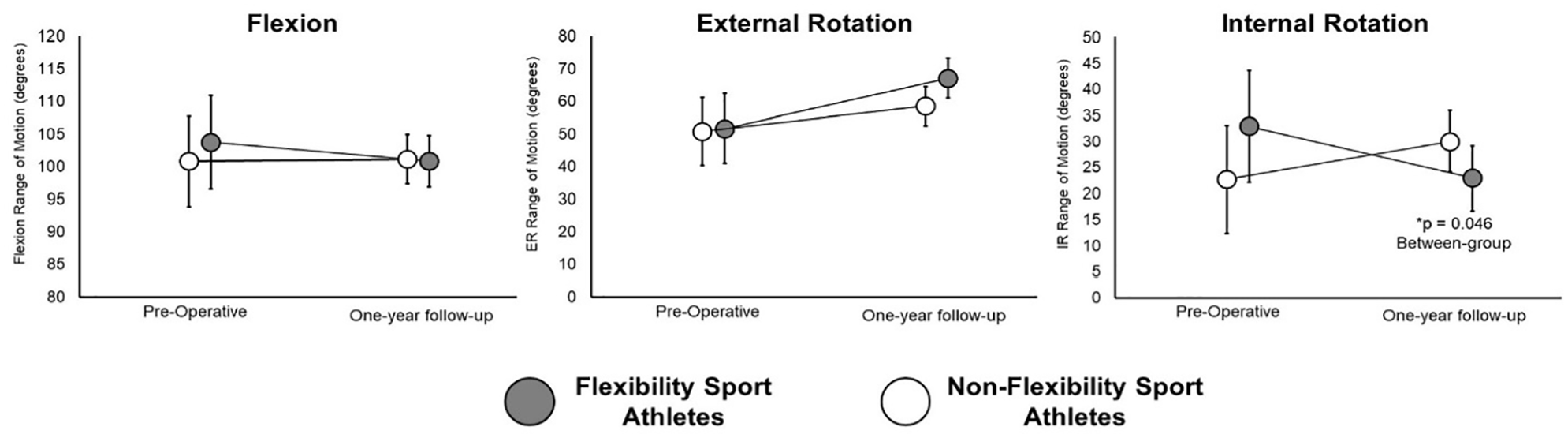
Comparison of pre-operative and 1-year range of motion values between flexibility and non-flexibility sport patients. Dots represent the mean value of the group; error bars represent the 95% confidence interval for the mean.
Discussion
Our study found that flexibility athletes regained their baseline ER by 1 year after surgery but did not always regain IR or flexion by that time. There was not a significant difference between when non-flexibility and flexibility athletes regained their baseline flexion and ER, though non-flexibility athletes regained IR at 1-year post-operation more often than flexibility athletes did.
All flexibility athletes in our study returned to baseline ER by 1-year post-operation, compared to 85% of non-flexibility athletes. ER was the earliest plane of motion to return to baseline (103vs 172 days in non-flexibility athletes). Although not statistically significant, this result may have important sport-specific implications for flexibility athletes. External rotation at the hip greatly contributes to, though is not the sole predictor of,15,16 the classic turnout position which is highly emphasized in ballet, figure skating, and other flexibility sports.10,11,17 Given that turnout functions as the foundation for many classic positions and movements, 11 this result could have clinical utility to orthopedic clinicians and rehabilitation professionals who are counseling dancers and other flexibility athletes before and after PAO.
A significantly lower proportion of flexibility athletes regained their preoperative IR compared to non-flexibility athletes (54%vs 100%, respectively; P = .02). Additionally, non-flexibility athletes regained baseline IR sooner than flexibility athletes (93vs 230 days, respectively) and demonstrated higher average IR amplitude by 1-year follow-up, although neither of these results were statistically significant. These observations may still be clinically significant and could be explained by intraoperative and postoperative considerations. First, decreased amplitude of IR after PAO may be partially attributed to the amount of acetabular correction performed. Other studies have attributed reduced IR after PAO to increased anterior acetabular coverage,18,19 which may decrease the ability of the hip to internally rotate to the same degree as it had preoperatively. However, this explanation alone would not account for the difference we observed between flexibility and non-flexibility athletes. A second consideration is that flexibility athletes and rehabilitation professionals may be less focused on recovery of IR compared to ER and other hip ranges of motion. One study comparing hip ROM between high-level dancers and non-dancers found that dancers tend to have a lower IR, leading to a more ER-focused arc of motion at the hip. 9 Therefore, it is possible that sport-specific rehabilitation for many flexibility athletes prioritizes recovery of ER and other ranges of motion, rather than IR. Thus, our finding that 100% of flexibility athletes regained ER may be more clinically relevant to flexibility athletes than the finding of decreased IR recovery.
Though not statistically significant, only 69% of flexibility athletes regained baseline hip flexion at 1-year follow-up. This is consistent with Novais et al, who also found an average reduction in the amplitude of flexion after PAO in young dancers, 9 suggesting our finding may be clinically significant. As with IR, changes in anterior acetabular anatomy after PAO may limit the ability to regain baseline flexion by reducing the maximum potential ROM in this plane. Flexion is especially critical to proper landing techniques in flexibility sports.20,21 The possibility of reduced flexion leading to altered landing mechanics during leaping, jumping, or tumbling is a clinically relevant outcome to discuss with patients and to monitor throughout recovery.
We acknowledge several limitations to our study. First, this is a retrospective analysis of registry data which includes patients who underwent PAO. This created a limitation in the type of hip ranges of motion that could be included in our study. A prospective study tracking patients’ recovery in additional planes of motion after PAO, such as hip extension, 11 would increase the clinical utility of this study. Second, all ROM measurements were visually assessed by orthopedic surgeons in clinic. Although patients were followed by the same orthopedic surgeon preoperatively and postoperatively, the use of a measurement tool such as a goniometer would enhance internal consistency and accuracy of measurements. Third, this is a single-center study. A larger sample size would allow us to investigate whether demographic factors such as age and sex had an effect on return of ROM.
Practical and Clinical Applications and Implications
Flexibility athletes are a unique patient group where sport-specific movement demands an increased hip ROM compared to non-flexibility athletes. Despite this, there is limited data available regarding postoperative outcomes in flexibility athletes who have undergone PAO. In our study, 100% of flexibility athletes regained baseline ER within 5º by 1-year post-operation; 69% regained baseline flexion; and 54% regained IR. Of these planes of motion, ER and flexion are most likely to be clinically relevant to the flexibility athlete. However, clinicians may consider monitoring each of these variables closely throughout follow-up and increasing rehabilitative techniques to increase flexion and IR. Our findings can help providers set expectations regarding the recovery of ROM in flexibility athletes who are considering undergoing PAO for symptomatic hip dysplasia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.