
Abstract
A patient was diagnosed with ulcerative colitis (UC) in 2010. In March 2015, she had abdominal pain, diarrhea, bloody stool, and UC has relapsed. In June 2015, pain and sensory disturbance of both lower limbs appeared. Blood flow at the distal femoral artery was not confirmed with magnetic resonance angiography, and it was diagnosed as bilateral acute inferior limb ischemia. Arterial thrombolectomy with Fogarty’s balloon catheter was performed and blood flow was improved. The severity of UC was moderate with Mayo score 8. Thrombosis is considered to be a complication with a high incidence in inflammatory bowel disease. Reports of arterial thrombosis are very rare. It is important to evaluate the risk of bleeding and thrombosis in active or severe cases in UC and need to do thrombotic prophylactic treatment simultaneously with UC treatment.
Keywords
Introduction
Ulcerative colitis (UC) is a chronic inflammatory bowel disease of an unknown etiology that is localized to the colonic mucosa. Chronic inflammation causes various extraintestinal complications. Venous thrombosis is a relatively common extraintestinal complication, but arterial thrombosis is a rare complication of UC. We report a case of bilateral acute inferior limb ischemia in a patient with UC.
Case Report
A 49-year-old woman was diagnosed as having UC (total colitis and relapsing-remitting types) in 2010. Beginning in March 2015, she had abdominal pain, diarrhea, bloody stool, and UC relapse. She was admitted to another hospital from mid-May 2015 and started induction therapy with prednisolone (PSL) 40 mg/d, salazosulfapyridine 8000 mg/d, and azathioprine 50 mg/d. The symptoms improved, but remission was not attained. In June 2015, pain and sensory disturbance of both lower limbs suddenly appeared. As magnetic resonance angiography (MRA) did not detect the blood flow in the distal femoral artery, she was diagnosed as having bilateral acute inferior limb ischemia. For detailed examination and treatment, she was immediately transferred to our hospital. After hospitalization, anticoagulation therapy was performed with heparin and prostaglandin E1; however, the pain in the lower limb worsened. Thus, arterial thrombolectomy with Fogarty’s balloon catheter was performed on the following day. The severe pain was relieved, and the femoral arterial blood flow was improved on magnetic resonance imaging (MRI; Figures 1 and 2). On colonoscopy for detailed evaluation, the severity of UC was moderate, with a Mayo score of 8 (Figure 3). Therefore, PSL 40 mg/d with salazosulfapyridine 8000 mg/d and azathioprine 50 mg/d were administered. She was discharged on the 28th day from admission, with improvement of arterial thrombosis and UC activity.

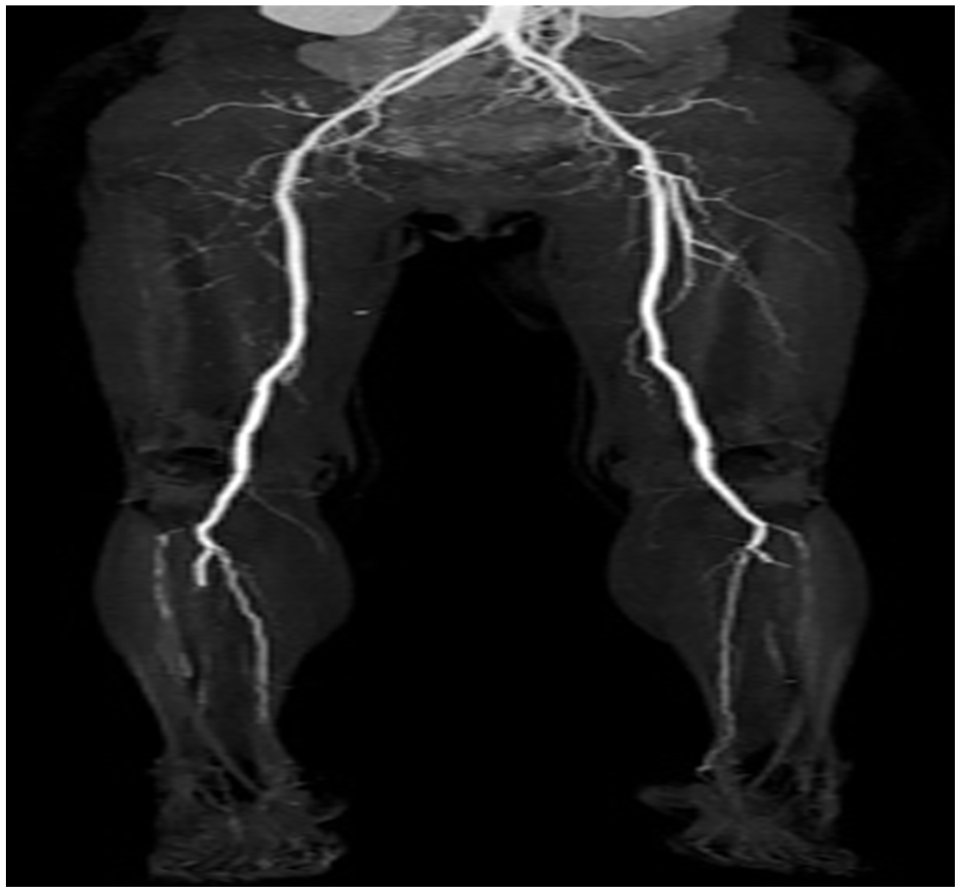
Magnetic resonance angiogram showing no blood flow in the distal femoral artery.
Improvement of distal blood flow from the bilateral femoral artery.

The sigmoid colon with multiple shallow ulcers with a Mayo endoscopic subscore of 3.
Thrombosis is considered a complication with a high incidence of inflammatory bowel disease.
1
Although venous thrombosis is common, arterial thrombosis is a rare condition. The causative factors of thrombosis are thought to be as follows: increased number of thrombocytes and abnormality in the coagulation system according to disease activity. Previous studies showed that an increased number of thrombocytes was more frequently found in active or severe cases of UC.
2
Of UC cases, 79% that developed thrombosis were in the active phase.
3
In the present case, the number of platelets was increased (64.6 × 104/μL on admission) with prolonged inflammation. On the other hand, the coagulation test results were within the normal ranges (prothrombin time/international normalized ratio, 1.10 and
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MK and TS wrote the manuscript and provided the images. FT, KTa, KTs, KTo, YM, MI, KG, and AI reviewed the manuscript. TS is the article guarantor.
Informed Consent
We had received informed consent from the patient.