
Abstract
Angiomyolipomas are rare benign tumors of the kidneys, with a risk of spontaneous hemorrhage including severe retroperitoneal bleedings. In this study, we report clinical outcomes of 5 patients who underwent 8 embolization sessions using 96% ethanol, as there is scarce data using this embolic agent for this indication. The primary angiographic success could be achieved in all but 1 lesion, which was not accessible due to vasospasm of the supplying vessel. Therapeutic success could be demonstrated in all treated cases for which follow-up imaging was available (n = 3). In 1 complex patient, a mildly reduced renal function, as well as a new onset of arterial hypertension was detected after treatment. Nontarget embolization of vital kidney tissue was demonstrated in another patient; it remained asymptomatic. Embolization therapy using 96% ethanol is an optional method to treat renal angiomyolipomas.
Background
Angiomyolipomas are relatively rare benign tumors of the kidneys, with a risk of spontaneous hemorrhage that may lead to severe retroperitoneal bleedings. In serial ultrasound screenings, angiomyolipomas could be found in 0.1% of the male and in 0.22% of the female population, respectively.1,2 Angiomyolipomas consist of abnormal blood vessels, smooth muscle cells, and fat cells in varying amounts. The structurally altered blood vessels are prone to the formation of aneurysms and to ruptures, as they bear no internal elastic lamina and their smooth muscle is replaced by fibrous tissue, which makes the vessels more rigid and tortuous.3-5
A review of the literature showed that almost 60% of patients present with clinical symptoms, 2 most typically with flank pain, a palpable tender mass, and macroscopic or microscopic hematuria. Of importance is the possible complication of a potentially life-threatening hemorrhage. Nevertheless, a significant number of angiomyolipomas are detected incidentally on radiographic findings, where the presence of fatty tissue in the renal tumor is essential to diagnose an angiomyolipoma using magnetic resonance imaging (MRI) or computed tomography (CT) studies. 2
In 80% of the patients, angiomyolipomas occur sporadically, whereas 20% are associated with tuberous sclerosis complex (TSC), an autosomal dominant systemic disorder predisposing to benign tumor formation in multiple organs. Both sporadic and in TSC-associated angiomyolipomas affect women in almost 90% of cases.2,6
Established indications for therapy are clinically symptomatic lesions of any size or a tumor size exceeding 4 cm of diameter. Treatment options include nephrectomy, partial nephrectomy, and selective arterial embolization. Recent therapy strategies are focusing on the nephron-sparing procedure of embolization. Embolization therapy of angiomyolipomas has been performed with variety of agents used for embolization, such as gelatin, polyvinyl alcohol, coils, foam, ethanol, and combinations of these agents.6-9 Ethanol is used alone or in combination with other agents such as oil or microparticles.10-12 Pure ethanol is a widely used embolization agent, but there is only scarce data using it for this indication. 13 In the literature, predominately oil or microparticles are added to ethanol when treating angiomyolipomas.10-12 In this study, we want to report on the findings of using pure 96% ethanol.
Patients and Methods
We analyzed all patients who underwent selective arterial embolization of renal angiomyolipomas at our institution between March 2015 and May 2017. In this period, no patients referred to our institution were excluded from this treatment option. Data on differently treated patients by other medical specialties were not available. In total, 5 patients were treated in 8 embolization sessions. In all of them, 96% ethanol was used. Written informed consent was obtained from all patients.
Treatment
The embolization procedures were planned electively in general anesthesia for precise cardiopulmonary monitoring and because of the painful nature of this procedure when performed without general anesthesia. To modulate the inflammatory reaction, 14 a single dose of prednisone 125 mg was administered intravenously before the procedure (Solu-Medrol; Pfizer PFE Switzerland, Zurich, Switzerland). After the intervention, oral dexamethasone (Dexamethason Galepharm, Zurich, Switzerland) was routinely prescribed for 4 or 7 days at an initial dose of 8 mg/d and was weaned off. For pain management, nonsteroidal anti-inflammatory drugs (NSAIDs) were prescribed.
Femoral arteries were accessed using a 5 F sheath (Radiofocus introducer II, Terumo, Tokyo, Japan). Subsequently, abdominal aortographies were performed followed by catheterization of the target renal arteries (C1; Cordis, Miami Lakes, FL, USA). Super-selective angiographies were performed to identify the supplying vessels of the angiomyolipomas. Then, embolizations were performed by slowly instilling ethanol under free flow conditions. Due to lack of visibility of ethanol under fluoroscopy, it was either mixed with contrast in a ratio 5:1 or it was applied in very small quantities followed by super-selective repeated angiograms. Injection was performed using 1 mL insulin syringes for better low flow control. Repeated injections were delayed by at least 1 to 2 minutes always followed by fluoroscopic contrast injection to estimate effect of ethanol embolization and to fill the microcatheter with contrast for better tracking the course of embolization.
Successful occlusions of the tumors supplying vessels were verified in a subsequent control angiography. The patients were discharged the next day. Routine postintervention ultrasound was performed either on the first day after the procedure or within 4 weeks. Postintervention cross-sectional imaging was performed with MRI or CT scans at the discretion of the referring specialists. Therapeutic success was defined as an eliminated arterial perfusion signal in duplex sonography and MRI or CT-scan.
Results
Patients
Five female patients aged 38 to 63 years (median age: 52.2 years) were treated in 8 elective embolization sessions. Details on these patients (labeled A through E) are summarized in Table 1.
Results and patient characteristics (patients labeled A through E).
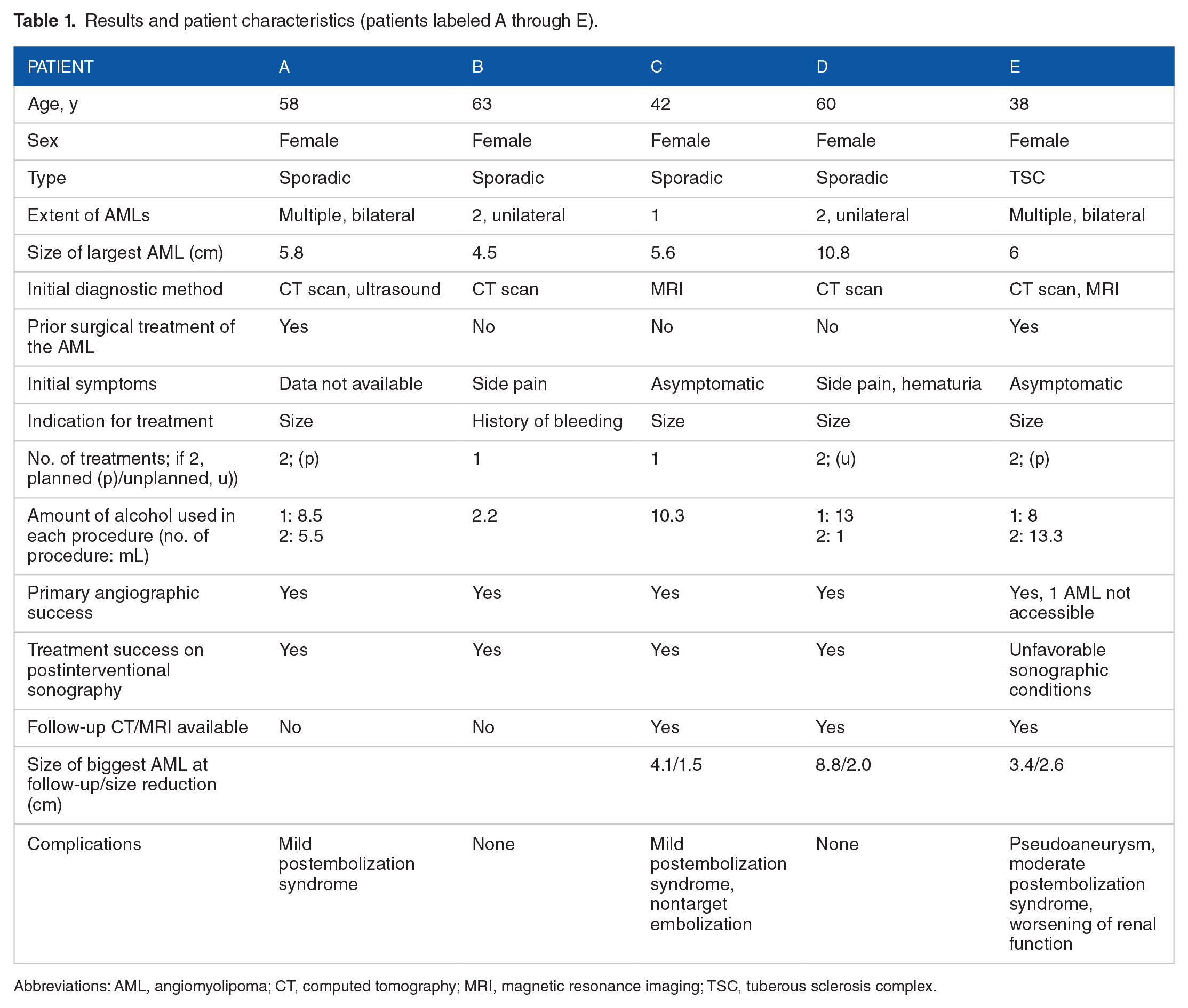
Abbreviations: AML, angiomyolipoma; CT, computed tomography; MRI, magnetic resonance imaging; TSC, tuberous sclerosis complex.
One patient (patient C) had a single angiomyolipoma, 2 patients (patients B and D) had 2 unilateral angiomyolipomas, and 2 other patients (patients A and E) had multiple bilateral angiomyolipomas, one of which was associated with TSC (patient E). Two patients (patients A and E) had a history of prior partial nephrectomy and in the same 2 patients, a planned second embolization was performed due to the multilobular tumor characteristics. In 1 patient (patient D), a reintervention was performed due to recurrent symptoms.
The treated angiomyolipomas had diameters ranging between 4.5 and 10.8 cm. Indications for the initial treatment were a large tumor size in 4 cases (patients A, C, D, E) and a history of bleeding in 1 case (patient B; Figure 1), respectively. In the latter patient, an elective embolization was performed 6 months after a self-limiting retroperitoneal hemorrhage occurred. A median amount of 7.7 mL of alcohol was used per embolization session (range: 1.0-13.3 mL).

CT scan (arterial phase) of a 63-year-old female patient (patient B) who presented with a history of flank pain for 5 days, showing an angiomyolipoma-associated retroperitoneal hematoma. No active bleeding was detected; an elective embolization procedure of the angiomyolipoma was scheduled. CT indicates computed tomography.
Efficacy
In all of our 5 patients, postinterventional control angiography showed complete angiographic elimination of the targeted angiomyolipoma, which was defined as treatment success. Figure 2 (patient A) and Figure 3 (patient D) show preembolization and postembolization angiograms. During follow-up examinations, therapeutic success could be confirmed in all cases using ultrasound, MRI, or CT scans. In 4 of the 5 patients (in patients A, B, C, D), no arterial perfusion was detectable in the postintervention ultrasound scan. In 1 patient (patient E), sonographic assessment was limited due to impaired ultrasound conditions. In 3 patients, follow-up cross-sectional imaging was initiated by the referring physicians 3 to 12 months after the intervention (patients C, D, and E). Complete target lesion elimination of the perfusion signal was confirmed in 1 patient (patient C), and a significant reduction of the target lesion perfusion was demonstrated in 2 patients (patients D and E). In all 3 patients, significant tumor size reductions were shown, ranging between 1.5 and 4.6 cm. Patient E had multiple angiomyolipoma s in both kidneys. Due to vasospasm, 1 of the 5 biggest lesions was not accessible during the initial procedure in this patient.

Preembolization (A) and postembolization angiogram (B) of a large angiomyolipoma (maximum diameter 5.8 cm) of the right kidney in a 58-year-old female patient (patient A) with multiple bilateral angiomyolipomas.
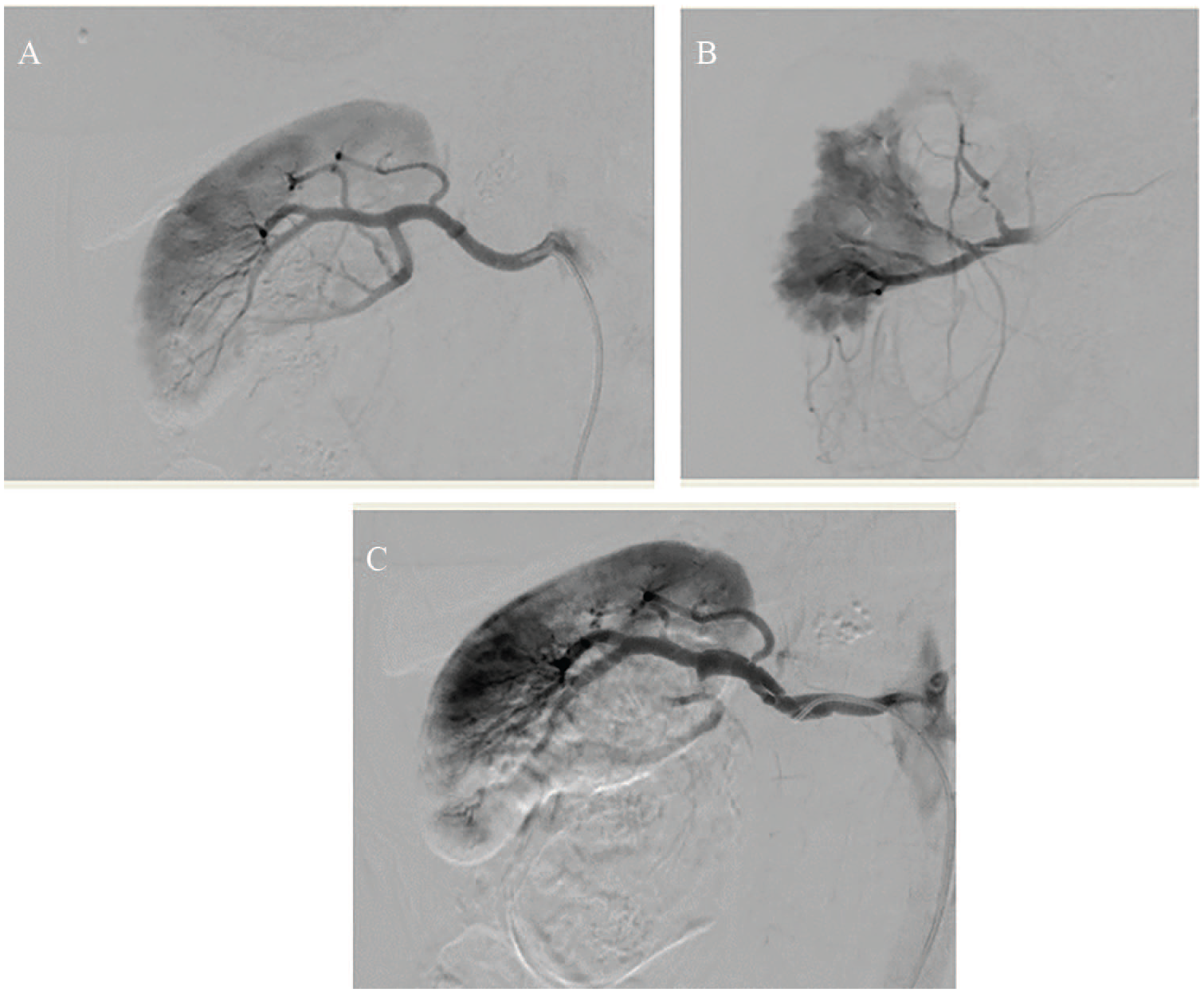
Embolization of a large angiomyolipoma located in the right kidney of a 60-year-old female patient (patient D). Showing the (A) initial selective angiogram, (B) a super-selective angiogram, and (C) the final angiogram after the first super-selective arterial embolization.
In 1 patient (patient D), an additional embolization had to be performed due to recurrent symptoms of abdominal pain and unexplained hematuria, although procedural success had been demonstrated in cross-sectional studies after the first embolization with an only weak residual arterial perfusion and a 20% size reduction in MRI. This was confirmed by re-angiography so that a small dose of 1 mL of 96% ethanol was applied (Figure 4). The final CT scan demonstrated a size reduction from 108 to 59 mm after both procedures (Figure 5).

Patient D underwent an unplanned re-intervention due to recurrent symptoms. (A) Residual perfusion of the angiomyolipoma could be demonstrated and (B) the final angiogram shows an elimination of the perfusion signal after embolization with an overlaying signal from lumbar arteries.

(A) Preinterventional and (B) postinterventional CT scan (arterial phase) of the same patient (patient D). A size reduction of the angiomyolipoma from 108 to 59 mm could be demonstrated after 2 embolization sessions. CT indicates computed tomography.
Safety
Mild and self-limiting postembolic flank pain occurred in 2 patients (patients A and C). In 1 patient (patient E), moderate to severe abdominal pain required rehospitalization for analgetic therapy. In the same patient, a femoral pseudoaneurysm was detected at the puncture site which was treated successfully by ultrasound-guided compression. In this patient, mildly increased creatinine (from 86 to 99 µmol/L) and new onset of arterial hypertension was detected after the intervention. This complex patient had a history of a prior partial nephrectomy, due to the vast extent of multiple bilateral angiomyolipomas associated with TSC. Two elective consecutive embolizations were performed in her targeting multiple tumors.
Discussion
Angiomyolipomas are benign tumors of the kidney that require interdisciplinary management. Therapeutic options include partial or total nephrectomy. 6 However, nephron-sparing endovascular embolization has evolved as the standard therapy.
There is a variety of agents used for embolization.6,8-14 In our practice, we preferably use pure 96% ethanol for tumor and vascular malformation embolizations. 15
Ethanol denaturates proteins resulting in intravascular thrombosis and subsequent tissue infarction and fibrotic and necrotic tissue remodeling. 14 Application techniques of undiluted 96% ethanol may vary. Besides directly injecting alcohol under free flow, different other application options are described in the literature. Some authors describe using flow control devices such as balloons to attenuate the arterial perfusion or the venous drainage of the tumor to enhance the denaturating effect of the alcohol on the endothelial cells by increasing the contact time. Authors also describe that the alcohol can be aspirated after being left in situ for a minute, when the perfusion has been blocked with an occlusion balloon.11-13 In our series, we injected 96% ethanol under free flow conditions, in the absence of flow control devices to avoid locoregional toxic effects seen with prolonged exposure to undiluted ethanol.
Possible adverse events of alcohol embolization include cardiopulmonary complications, which may lead to acute pulmonary hypertension and acute right heart failure as a consequence of pulmonary artery spasms or extensive microthromboembolization. Therefore, the intervention should be performed under close cardiopulmonary monitoring. However, according to Shin et al, 16 the risk of cardiopulmonary complications is low when <0.14 mL ethanol/kg body weight are applied every 10 minutes, with a maximum dose of <1 mL/kg body weight per session.15-19 After having used pure ethanol for many years for treating of vascular malformations at our institution, we prefer to perform these procedures in general anesthesia, due to the painful nature of alcohol embolization as well as for precise cardiopulmonary monitoring.
In our series of patients, we had a primary angiographic success rate of 100% of the treated tumors. Regarding adverse events, in 1 of our 5 patients, a mild worsening of an already preexisting reduced renal function (pre- and postprocedure chronic kidney disease [CKD] stage II) was noted after the intervention together with new arterial hypertension. As the final angiogram showed intact healthy renal parenchyma, a nephrotoxic effect of the contrast was suspected in this long and complex procedure targeting multiple bilateral angiomyolipomas in 1 session. An additional third planned treatment session, which was considered necessary because of arterial spasm in one of the supplying arteries of 1 remaining angiomyolipoma, has not been performed to date. The consensus with the referring specialist was to postpone the intervention to not jeopardize kidney function further in this polymorbid patient. Of note, follow-up MRI showed only a residual perfusion signal in the treated angiomyolipomas and a size regression in most of the treated lesions in this patient.
In another patient, a limited nontarget embolization could be demonstrated in the final angiogram, affecting 10% to 15% of the vital kidney tissue. However, this finding remained asymptomatic, with no effects on renal function. As pure ethanol is not visible under fluoroscopy, possible nontarget embolization due to backflow is a concern. To limit this risk, ethanol either was mixed with contrast or was applied undiluted in only very small quantities using a 1-mL insulin syringes followed by super-selective repeated angiograms.
Nontarget embolizations are possible adverse events of any embolization therapy; however, these are rare events. In a literature review by Murray et al 6 the total postinterventional morbidity in patients undergoing embolization procedures for the treatment of angiomyolipomas was described in 6.9% of patients, which included nontarget embolization in 2.3% of patients, respiratory complications in 2.0%, abscess formation in 1.6%, active retroperitoneal hemorrhage in 1.0%, allergic reactions in 0.6%, urinary retention in 0.6%, urinary tract infections in 0.3%, femoral artery damage requiring repair in 0.3%, and renal artery spasm in 0.3% of patients.
An additional embolization was performed in 1 patient due to recurrent symptoms and otherwise not explained hematuria, despite radiological success of the treatment. Murray et al 6 in their systemic review describe that re-embolizations or surgeries are required in 20.9% of angiomyolipomas treated with embolization (at a medium follow-up time of 39 months). The most common indications for re-embolization procedures are described as revascularization on follow-up imaging (30.0%), unchanged or increasing tumor size (22.6%), refractory or recurring symptoms (16.7%), and acute retroperitoneal hemorrhage in 14.3% of the cases. However, re-angiography in our patient demonstrated subtotal angiomyolipoma occlusion so that only 1 mL of alcohol was applied. Because symptoms persisted after successful reintervention, an alternative explanation for the symptoms seems likely.
An inherent limitation of a case series of patients undergoing embolization procedures is that the included subjects have been previously chosen for this treatment modality and not for another one. Our findings therefore are not necessarily applicable to all patients with angiomyolipomas.
In conclusion, our case report and literature review provides evidence that embolization using 96% ethanol is an option to treat renal angiomyolipomas. Please find teaching points and a quiz in the appendix.
Footnotes
Appendix
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Iris Baumgartner encouraged Alexander Rosenov to write the manuscript and provided the idea and concept. Alexander Rosenov wrote the manuscript under supervision and Marc Schindewolf who contributed relevant parts to the manuscript. Iris Baumgartner contributed relevant parts to the manuscript. Christoph Saely supervised the findings of this manuscript and added relevant contributions. All authors discussed the findings and contributed to the final manuscript.