
Abstract
Purpose
Our study aimed to evaluate the effect of daily oral dose of everolimus in the treatment of patients with tuberous sclerosis complex (TSC) associated with renal angiomyolipoma (RAML), and the feasibility and safety of surgical treatment approach.
Methods
We retrospectively investigated a total of 13 patients diagnosed of TSC-associated renal angiomyolipoma (TSC-RAML) who were scheduled for everolimus therapy. At 3-9 months after starting everolimus therapy, 4 of the study patients were symptomatic and underwent partial renal resection surgery. Two of these surgeries were performed open nephron sparing surgery (NSS) after TAE (Trans-arterial embolization), while the remaining 2 underwent robot-assisted partial nephrectomy (RAPN). A multi-slice helical CT scan performed among all the patients every 3 months, which was used to measure the volume and the density of the lesion.
Results
Follow-up CT images revealed a significant reduction (P < .05) in the RAML volume, at a rate ranging from 11.6 to 42.5%, in response to everolimus therapy (10 mg/day) in TSC-RAML patients. Further, a significant decrease in the mean tumor density (P < .05), as compared to its baseline value, was also observed. Super-selective renal arterial embolization done prior to NSS was effective in reducing the intraoperative bleeding and stabilizing the patient during the NSS procedure: mean warm ischemia time was 29.5 minutes (range 18-40 minutes) and mean intraoperative bleeding volume was 275 mL (range 200-350 mL). Post-surgical (both NSS and RAPN) follow-up showed a favorable perioperative morbidity profile with good renal functional preservation. At the end of 2 years, all patients were well, with no signs of progression or recurrence of the condition, and demonstrated normal renal function.
Conclusions
The results suggested oral everolimus as an effective non-invasive therapy to treat TSC-RAML patients. Post mTOR inhibitor therapy, NSS and RAPN are preferred mode of surgical intervention in symptomatic patients. TAE prior to NSS is beneficial.
Keywords
Introduction
Renal angiomyolipoma (RAML) is a benign type renal neoplasm that is comprised of fat, smooth muscle, and disorganized vascular elements. When associated with tuberous sclerosis complex (TSC), RAML is characterized as multiple and commonly bilateral lesion, 1 and is the leading cause of death in TSC patients as it typically enlarge with time, resulting in arterial hypertension and potentially life-threatening hemorrhage. 2
To date, the main line of treatment of RAML associated with TSC (TSC-RAML) patients is embolization or elective surgery, and when associated with uncontrollable haemorrhage emergency nephrectomy is preferred. 3 Performing renal transarterial embolization (TAE), an effective method to control acute haemorrhage, may help to prevent TSC-RAML associated hemorrhage before surgical intervention. Moreover, in asymptomatic RAML, such selective embolization or kidney-sparing resection has been accepted as a second-line of therapy. 4 Post-embolisation, partial nephrectomy is proven feasible and efficacious in TSC-RAML patients with large bilateral or unilateral lesions. 5 However, a delay in partial or total nephrectomy after angioembolisation may lead to extensive tissue adhesion, and thus should be done within a few days of the procedure.6,7
Recently, mammalian target of rapamycin (mTOR) inhibitors has been recommended as the first-line of treatment in TSC-RAML patients with large (>3 cm in diameter) but asymptomatic lesions.4,8 In this regards, health authorities have approved everolimus, a mTOR inhibitor, to treat TSC-RAML patients who do not require immediate surgery.
Here we report the effect of everolimus on TSC patients with massive RAMLs. Besides, partial nephrectomy was preferred in symptomatic patients with large or multicentric RAMLs, after oral everolimus (10 mg/day) therapy.
Material and Methods
Patients and Study Design
From July 2016 to August 2019, a total of 13 TSC patients diagnosed based on the 2021 international TSC surveillance and management Guidelines, 9 with RAML lesions measuring ≥4 cm and who were scheduled for everolimus treatment, were retrospectively recruited; and all patient details were de-identified in the study. This study was approved by the local ethics committee (NO. 2019-KY-264), and a waiver of informed consent was obtained. The dose of everolimus was set at 10 mg once a day by oral and maintained throughout the treatment. Blood testing, urinalysis, abdominal CT or MRI scan were carried out every 3 months after treatment initiation. By comparing the volume of the RAML in subsequent scans to volume prior to the everolimus treatment, we calculated the AML reduction rate and transition of the mean Hounsfeld unit (HU) value or T1-weighted/T2-weighted imaging for each patient. Then adverse events were evaluated, when a grade 3 or more severe adverse event was observed, the treatment was suspended. It was restarted after the adverse event was resolved. Indications for surgical treatment of AML include intractable pain, large-size tumors (≥4 cm), or spontaneous ruptures after everolimus administration for ≥3 months. Estimated glomerular filtration rate (eGFR) values were calculated using the modification of diet in renal disease (MDRD) formula. 10 The eGFR value was measured preoperatively, every 3 months postoperatively, and at the latest follow-up. All the patients were followed up for 2 years. Patients were included if they met the following inclusion criteria: (1) Men or women (not pregnant) ≥18 years; (2) Clinical and/or genetic diagnosis of TSC-RAML; (3) CT or MRI shows 1 or more TSC RAMLs with the longest diameter ≥4 cm; (4) Without RAML bleeding or embolism in the past 6 months. Patients were excluded from the study if they met the following exclusion criteria: (1) Age <18 years; (2) Women who plan to be pregnant or have been pregnant or lactating; (3) CT or MRI shows the longest diameter of RAML <3 cm; (4) History of RAML bleeding or embolism in the past 6 months; (5) Uncontrollable epileptic seizures despite being treated with anti-epileptic agents; (6) Patients who could not periodically visit the hospital.
Imaging Conditions
A 40-slice scanner (Health Care Discovery, GE, USA), with an X-ray tube voltage of 120 kVp, was used to perform the CT imaging. The effect of patient’s size or body weight on the radiographic optical density and patient dose was compensated by adjusting the tube current accordingly. The obtained data from the initial CT scan was reconstructed into axial and coronal images with slice thickness of 3.0-4.0 mm. The mean HU value of the area representing RAML on axial CT images was determined as the density of the RAML. MRI examinations were performed with 3.0-Tesla scanner (MAGNETOM skyra, Siemens, Germany) using an 18-channel matrix torso coil. Imaging sequences and parameters: conventional sequences included T1WI, T2WI, DWI (b = 50, 800). Specific parameters: slice thickness 4 mm, spacing .8 mm, TR 3500 ms, TE 85 ms, FOV 300 mm × 300 mm. Typically, T1-weighted images were used for volume assessment. Contrast-enhanced MR imaging was used if indicated. Dynamic contrast-enhancement-magnetic resonance imaging (DCE-MRI): T1WI-TWIST, flip angle 2°/15°, slice thickness 3.5 mm, spacing .7 mm, TR 4.91 ms, TE 1.90 ms, FOV 260 mm × 260 mm. Radiologists experienced in diagnostic radiology evaluated all the images.
Surgical Intervention
After scheduled everolimus treatment, symptomatic TSC-RAML patients with tumors ≥4 cm and tendency of bleeding, surgical interventions remain the preferred form of management. In our cases, TAE was used primarily to control bleeding, as also helping stabilize the patient for attempted partial nephrectomy. Embolization, selective arteriography of renal artery, was performed in 5 cases, in whom a superselective catheterization of the segmental renal artery was performed to locate the exophytic lesion. The indications of partial nephrectomy in present study are established in patients who were still flank discomfort at the time of presentation had a tumor ≥4 cm, particularly with recurrent bleeding, or lack of regression of the lesion after everolimus treatment. In our study, 2 patients underwent open nephron-sparing surgery (NSS), via retroperitoneal surgical procedure, which was conducted by placing the patients in a full lateral decubitus position with a raised waist bridge. Robot-assisted partial nephrectomy (RAPN) was performed in 2 cases by using the da Vinci standard surgical system with 4-arm setting, in whom the transperitoneal route, with routine clamping of both renal artery and renal vein, was adopted. Considering the prolonged resection time and warm ischemia time with conventional RAPN, the use of open NSS is even more critical in TSC patients accompanied with impaired renal function as the giant and multifocal disease pattern with a higher rate of recurrence, or lesion in a solitary kidney which makes renal parenchymal preservation a key concern. Additionally, RAPN is likely generalizable to at least small AMLs or treatment strategy based on the patient’s preference to some extent. The reporting of this study conforms to STROBE guidelines. 11
Statistical Analysis
Statistical analysis was performed with the SPSS 20.0 software (Inc., Chicago, IL). Wilcoxon’s signed-rank test was used to analyze the changes in the tumor volume and density. A value of P < .05 was considered statistically significant.
Results
Patient Characteristics
Patients’ characteristics.

Treatment Efficacy
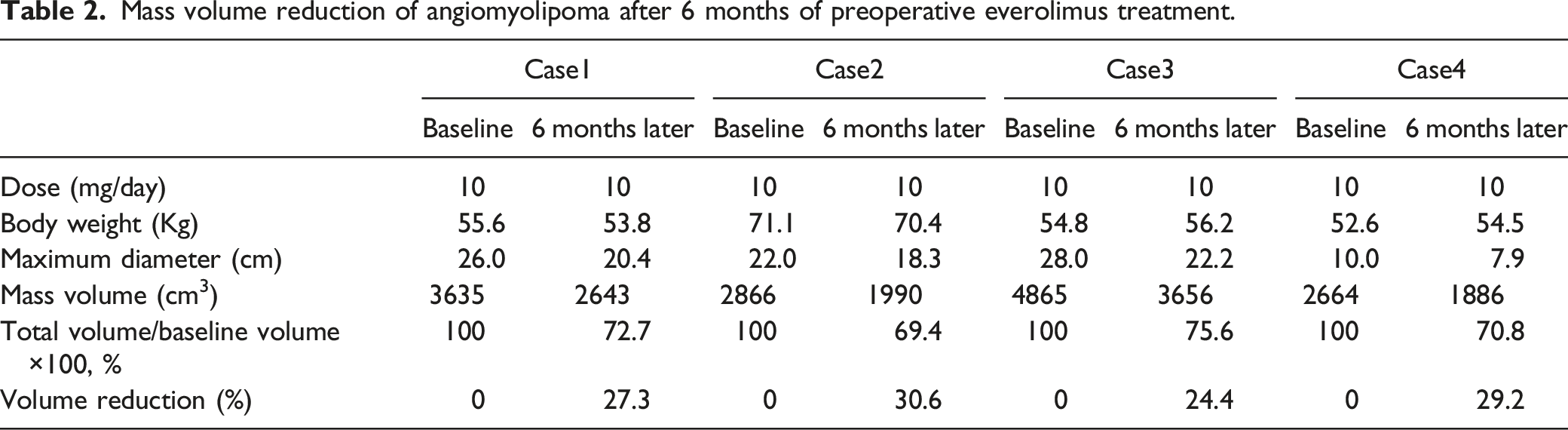
The TSC-RAML patients in this study received 10 mg of everolimus for a median period of 15.8 months (range 5.5-26.5 months). After initiating the treatment, serial CT or MRI scan was performed to measure the RAML volume that was used to calculate the volume reduction rate, defined as the percentage change in the tumor volume. The largest volume reduction rate from the baseline in each study participant is shown in Figure 1. In most patients, a marked decrease in the RAML volume was evident after 3 months of treatment (Figure 2(b), (f)). Primary-tumor shrinkage was most rapid during the initial 6 months of treatment, with evidence of a sustained response at subsequent time points during the core treatment phase. Nine months thereafter, the AML hardly shrank, and remained approximately the same size. After 12 months of therapy, more than 80% of patients experienced reduction in renal angiomyolipoma volume of >50%, and this degree of response continued over the study period. The mean volume decreased to 41.14 ± 26.54% of the baseline volume (P < .05) (Table 2 and Figure 1). No new angiomyolipoma lesions were observed, and no instance of grade 2 bleeding occurred. Figure 2(d) and (f) shows the mean tumor density values at baseline and after 6 months of treatment, which revealed a significant decrease in the mean tumor density in all patients. We chose to perform a superselective embolization of the afferent arteries via the transfemoral arterial approach, which allowed us to identify irregular arterial branches supplying the lesion and the final cessation of blood flow in the treated vessel (Figure 2(g), (h)). eGFR follow-up data were available for all 14 patients. No local recurrences were observed and the median (IQR) change in eGFR was 5.2 (0-12) mL/min/1.73 m2 during 12 months. Significant difference of renal function was virtually observed in 1 patient, eGFR at baseline and the latest follow-up was 85.5 mL/min/1.73 m2 and 73.4 mL/min/1.73 m2, respectively. The effect of everolimus daily on renal angiomyolipoma volume reduction over time. The difference of angiomyolipoma volume reduction in the study patients was statistically significant between at baseline and after 12 months of treatment (P < .05). Target TSC-RAML patients. (A, B) Median volume decrease from 3314 cm3 at baseline to 2795 cm3 after 3 months of everolimus 10.0 mg; (C, D) Showing a decrease in tumor size and an increase in low-density area within the tumor (white arrow); (E, F) Treatment with everolimus was initiated at a dose of 10 mg/day. After 1 year, total renal size decreased to 1560 cm3 (67.6% of baseline); (G, H) CT scan of the kidney and pre-embolization angiogram showing arteries supplying the lesion after super-selective catheterization of the segmental renal artery. Panel A, C, E: RAMLs before initiation of everolimus therapy; panel B,D,F: RAMLs after initiation of everolimus therapy. Mass volume reduction of angiomyolipoma after 6 months of preoperative everolimus treatment.

Adverse Events
Most frequent side effects in our group were stomatitis/oral ulcer (69.2%, 9/13), headache (53.8%, 7/13), abdominal pain (46.1%, 6/13), hypercholesterolemia /hypertriglyceridemia (38.4%, 5/13), urinary tract infection (30.7%, 4/13), and irregular menstruation/amenorrhea (22.2%, 2/9), and in most cases grade 1 or 2. The most common grade 3 adverse events were irregular menstruation (11.1%, 1/9) and mucositis oral (7.6%, 1/13). All patients improved with symptomatic treatment and resumed everolimus.
The Role of Preoperative Everolimus Therapy
Mean tumor density after 6 months of preoperative everolimus treatment.

*HU value was statistically significantly lower after 6 months therapy.
HU: Hounsfeld units.
Intraoperative and postoperative findings.
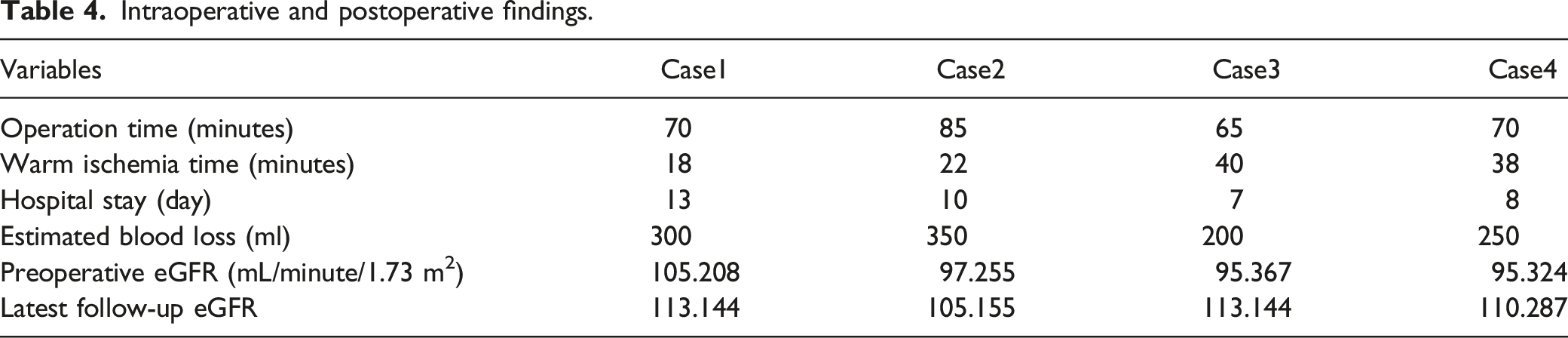
In these cases, solid lesions decreased in size with no trace of RAML-associated hemorrhage. Radiological assessment at 3-24 months after surgery showed no evidence of lesion recurrence or other postoperative complications.
Preoperative eGFR was 103 (IQR = 85.5-112) ml/min/1.73 m2, 6-month postoperative eGFR was 103 (IQR = 85.5-112) ml/min/1.73 m2 and 12-month postoperative eGFR was 107 (IQR = 85.5-112) ml/min/1.73 m2 (Table 4). The eGFR was obtained immediately prior to surgery, and the last available value was used to calculate the change in renal function. The eGFR was slightly decreased after NSS in 4 cases. However, there were no significant differences between the preoperative values and 12-month follow-up in these patients (Fig. 3(b)). Analysis of eGFR during follow-up from baseline in patients treated with everolimus (a) and NSS management (b) Arrows represent the time point of intervention. The difference of eGFR was statistically insignificant within postoperative 12 month from baseline in cases with everolimus treatment. The differences between preoperative and postoperative eGFR values were found to be statistically insignificant in 4 cases.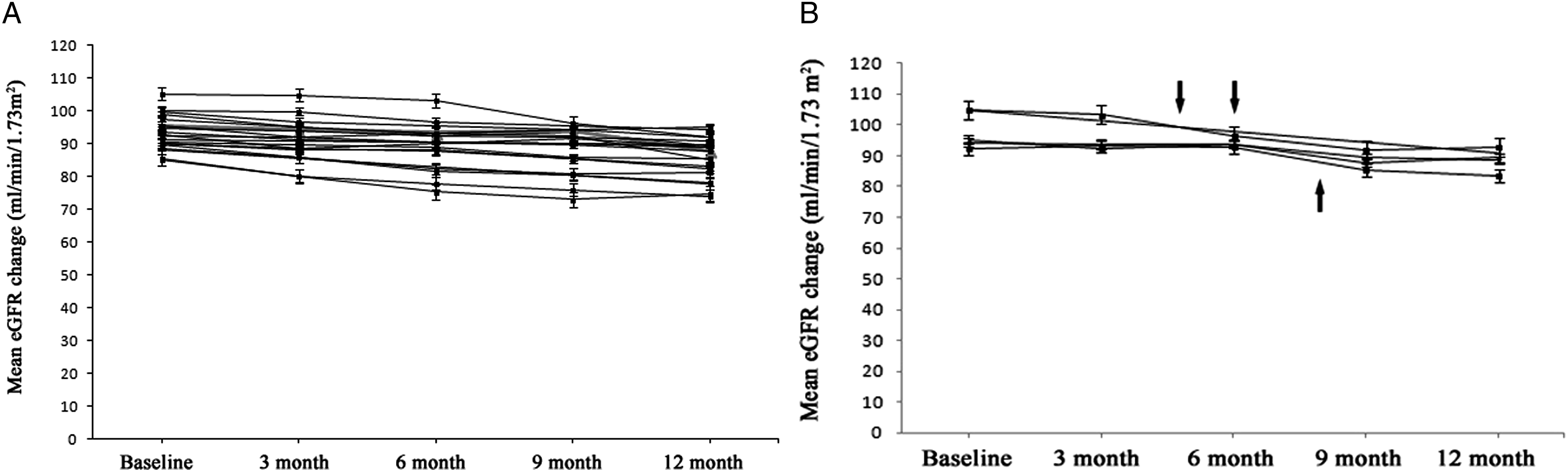
Discussion
TSC is a disease presenting with complex clinical picture, with increased morbidity and mortality when vital organs like central nervous system, heart, lung, and kidneys are involved. Although of benign nature, TSC-RAML is likely to grow, rendering the patients susceptible to comorbidities including life-threatening conditions like spontaneous haemorrhage. Retrospective analysis of patients with TSC demonstrated an increased risk of haemorrhage with increase in RAML size. Further, a direct correlation was also established between RAML size, aneurysm formation and the risk of haemorrhagic rupture.12,13
The goal of treating TSC-RAML patients is not only to prevent the progression of the tumor but also to regress the existing lesions, towards which, using targeted therapies that inhibit mTOR pathway is considered the most novel strategy. 14 Everolimus, an mTOR inhibitor derived from sirolimus, is an effective anti-proliferative agent that has been shown to be effective in reducing the volume of TSC-RAML. 15 In our study, a daily dose of 10 mg of everolimus could significantly reduce the mass volume of TSC-RAML, highlighting its efficacy as a targeted therapy in TSC-RAML patients. The average reduction rate of AML was 67%. Most of the AML reduction was of the solid component (angioma and leiomyoma), and there was only a slight reduction of the lipid component. The effect of everolimus on TSC-AML was mainly a reduction of the solid components consisting of angioma and leiomyoma. Accordingly, everolimus treatment significantly reduced the mean tumor density due to higher tumor shrinkage in the solid components with high tumor densities. In most cases, the AML volume decreased markedly within 9 months of treatment. The current trial shows that everolimus are effective in reducing angiomyolipoma size in tuberous sclerosis in present cohort.
The management of TSC-RAML is a complex procedure, especially in symptomatic patients with large or multiple lesions who demand surgical intervention. Further, parenchymal preservation is another important factor that determines the treatment approach, which is adroited by nephron-sparing surgery or preferably by selective embolisation, particularly in patients with compromised renal function, these techniques offer preservation of renal function with acceptable complication and recurrence rates. 16
Though TAE is an appealing option for management due to its less invasive nature and an effective treatment modality for acute hemorrhage, re-treatment rates are about 20%-40% of cases due to neoangiogenesis or re-canalization of treated vessels, or persistent symptoms after embolization. 17 Preoperative embolization of the large tumors is recommended to avoid excess blood loss during surgery. 18 Therefore, regardless of potential tumor shrinkage time in this study, the most important preoperative indication of TAE in renal AML treatment is previous history of retroperitoneal hemorrhage or the presence of large tumors. In these situations, embolisation may prevent total nephrectomy. In our present study, embolisation was performed in 2 of our study participants to control bleeding and stabilize the patient during the open NSS procedure, and the procedure was considered effective as these patients demonstrated low post-operative complications and no recurrence of RAML over the study period.
Any treatment method for renal AML should have a durable control of symptoms, low recurrence rate, and maximal preservation of renal function. Although active surveillance for clinically insignificant AMLs is broadly accepted, partial nephrectomy is still recommended for uncontrolled pain, a size greater than 4 cm, and failure or recurrence of embolisation with the risk of life-threatening hemorrhage.19-21 Besides, the decision of NSS is influenced by the patient’s age, anatomical location of the tumor in the kidney and the adjacent organs.
As seen in 4 cases, due to lack of tumor size reduction and uncontrolled pain on follow-up imaging in patients, partial nephrectomy should be strongly considered and it is always better to have some functioning tissue than making the patient anephric. mTOR inhibitors may diminish the potential bleeding risk by reducing vascularization itself to play a role in making this possible. 22 Such an effect can be achieved with preoperative everolimus therapy for 3-9 months, and such therapy could prevent the loss of renal function due to surgical procedures.23,24 Two of our study participants, underwent robot-assisted partial nephrectomy for their lesions without pre-operative embolisation, whose post-surgical follow-up showed a favorable perioperative morbidity profile with good functional preservation. In the RAPN series, none of the patients had a recurrence and eGFR preservation was 90% by published report. 25 Consistent with that, in the current study we did not observe AML or symptoms recurrence during follow-up (median 8 months), and there was no new onset CKD and the renal preservation rate was 95%. Among the 2 patients who needed transfusion in the NSS group, 1 had preoperatively anemia due to recurrent bleeding, and the other had plenty of intraoperative blood loss in tumor bed due to perirenal adhesion.
Almost all study participants reported adverse reactions of everolimus treatment that were tolerable, with stomatitis/oral ulcer and irregular menstruation/amenorrhea being the most common everolimus-related adverse reaction of them all. In addition, mTOR inhibitors block growth signals required for proliferation of endothelial cells and fibroblasts, thereby restricting fibrosis, which is a key factor in successful wound healing.26,27 If patients require subsequent surgeries and mTOR inhibitor therapy can be safely interrupted, the risk of wound-related adverse events may be reduced by stopping mTOR inhibitor therapy at least 1 week before surgery and resuming it 10-15 days afterward. 28 Furthermore, wounds should be somewhat healed and wound strength should be developing after the first 30 days postoperatively, the risks of wound complications associated with newly initiated mTOR inhibitor therapy at this stage should be minimal.29,30 Therefore, preoperative drug withdrawal was started 1 week before surgery, and continued for 4-6 weeks after surgery in our study, respectively. And no wound complications were observed in all patients.
Our study was subject to several limitations. First, the study was limited by the inherent drawbacks of retrospective design. Second, this study was a single, tertiary-care institution study. Finally, the number of patients is low to make a definite conclusion.
Conclusions
Collectively, the management of TSC-RAML is a complex procedure, and each option may have benefits depending on the specific clinical situation. The results of the present study suggest that the medical therapy in form of everolimus in TSC-RAML patients is beneficial and the patients may require maintenance therapy to continue to reap the benefits, particularly for patients not suitable for surgery. Secondly, super-selective embolization of segmental arteries that supply the lesion is considered as the most effective minimally invasive approach in preventing haemorrhagic events and symptomatic manifestations, and as a way to reduce the potential bleeding during the follow-up planned NSS. Thirdly, partial nephrectomy is the preferred treatment when the patient’s anatomy is available and the surgeon is experienced, more importantly, it should be considered as a treatment option in patients with recurrent bleeding, AML-related symptomatic, and suggesting limited size reduction for lesions after everolimus treatment. Lastly, robot-assisted laparoscopic partial nephrectomy may be an effective, feasible and safe method to treat TSC patients with RAMLs. It offers a good preservation of renal function in the long-term follow-up with a low clinically significant complication rate and rapid recovery of daily life.
Abbreviations
Hounsfeld unit
nephron sparing surgery
mammalian target of rapamycin
Renal angiomyolipoma
robot-assisted partial nephrectomy
trans-arterial embolization
tuberous sclerosis complex
tuberous sclerosis complex associated with renal angiomyolipoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by In-hospital Youth Fund, aim for the Top University Plan, of The First Affiliated Hospital, Zhengzhou University.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the First Affiliated Hospital of Zhengzhou University, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This retrospective study was approved by the Institutional Ethics Review Board (NO. 2019-KY-264), and a waiver of informed consent was obtained.