
Abstract
Background:
Cyst infection is a complication sometimes seen in patients with autosomal dominant polycystic kidney disease (ADPKD) and often shows through a positive blood culture. However, there have been no reports of ADPKD patients whose cyst infection propagate to peritoneal fluid leading to positive peritoneal fluid culture.
Case presentation:
A 74-year-old Japanese man with ADPKD under peritoneal dialysis (PD) was presented with left flank pain, fever, and chills at our hospital. He did not show any symptoms or signs suggestive of peritonitis. There were no elevated cell counts or polymorphonuclear leucocytes in his PD fluid. There were some complicated cysts found in computed tomography and magnetic resonance imaging examinations. We clinically diagnosed him as having a renal cyst infection rather than PD-related peritonitis. We initiated treatment by administering ceftriaxone with an immediate favorable response. As the possibility of accompanying prostatitis still remained, we switched to intravenous levofloxacin on the second day. On the 10th day, Helicobacter cinaedi was detected in 2 sets of blood culture as well as in PD fluid. We switched back to ceftriaxone and this treatment was entirely successful.
Conclusions:
This is the first report of H cinaedi cyst infection which propagates to peritoneal fluid in a patient with ADPKD.
Introduction
Cyst infection is a complication sometimes seen in patients with autosomal dominant polycystic kidney disease (ADPKD). 1 Although several studies have been conducted to explore testing and imaging modalities for diagnosing cyst infections, they are still difficult to clinically identify.2–4 The gold standard for diagnosing cyst infections is a cyst aspirate with the presence of pathogens or neutrophils. 2 One pathogen that was hard to be diagnosed is Helicobacter cinaedi, a gram-negative spiral bacterium colonizing in the intestinal tracts of animals and humans.5–8 It is a slow-growing organism and a long period of time is required before a blood culture shows positive. 9 H cinaedi infections were first reported in homosexual men and immunocompromised patients. 10 However, recently non-HIV and nonimmunocompromised patients with H cinaedi infections have also been reported. 6 There is also evidence that end-stage renal disease may be a risk factor for H cinaedi infection 11 and that H cinaedi infection commonly presents in a patient with cellulitis, colitis, and bacteremia.9,12 Here we report a case of cyst infection in a patient receiving peritoneal dialysis (PD), whose blood culture and peritoneal fluid culture got positive for H cinaedi.
Case Presentation
A 74-year-old man with medical history of ADPKD, benign prostate hypertrophy, hypertension, and a 2-year history of PD visited our outpatient clinic, complaining of left flank pain, fever, and chills for the past 3 days. He was in his usual state of health until 1 month before when he went golfing and got insect bite and cellulitis of his left ankle. He consulted a dermatologist the next day and was treated with cefdinir for a week and cellulitis healed. Three weeks before the admission, he had a low-grade fever, which sometimes spiked to 38°C to 39°C. Two weeks before his admission, he began to feel the left flank pain. He denies having any sexual intercourse for more than 5 years or a medical history of sexually transmitted diseases. He has no obvious family history of polycystic kidney disease; however, his mother as well as her sister and brother died of intracranial hemorrhage at the age of their 40s or 50s, which suggested ruptured cerebral aneurysm, a complication of ADPKD. On physical examination, his vital signs were normal. He had tenderness on left upper quadrant; however, any peritoneal irritation symptoms, such as rebound tenderness or muscular guarding, were absent. On digital examination, he had a slight sense of discomfort but no obvious tenderness, indicating the possibility of prostatitis. There was no skin rash. Laboratory data revealed an elevated white blood cell count with left shift. Urinalysis revealed a low level of white blood cells (Table 1). HIV test was negative. A computed tomography (CT) scan revealed complicated cysts (Figure 1). An abdominal magnetic resonance imaging (MRI) was performed to identify an infected cyst. The MRI scan revealed several complicated cysts, and it was difficult to determine the infected cyst (Figure 2). Therefore, we did not drain the infected cyst.
Laboratory data.
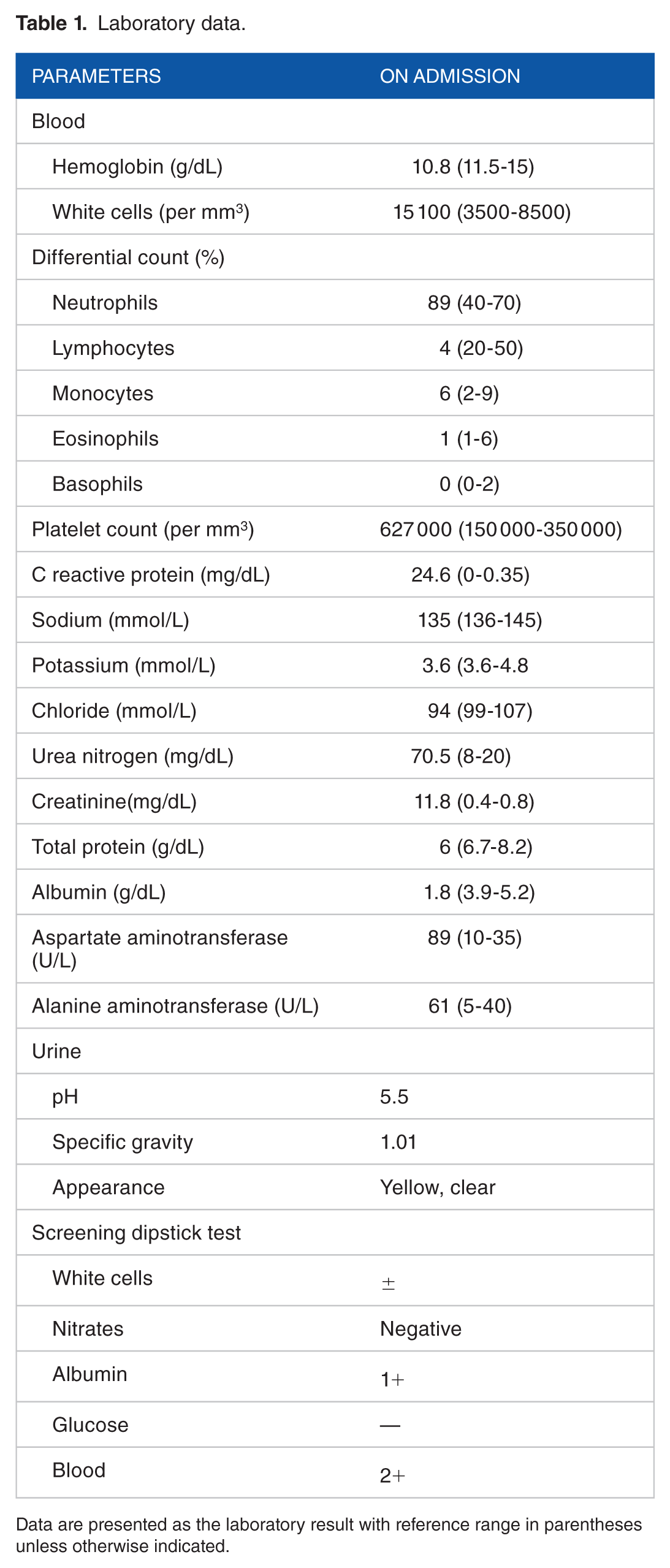
Data are presented as the laboratory result with reference range in parentheses unless otherwise indicated.
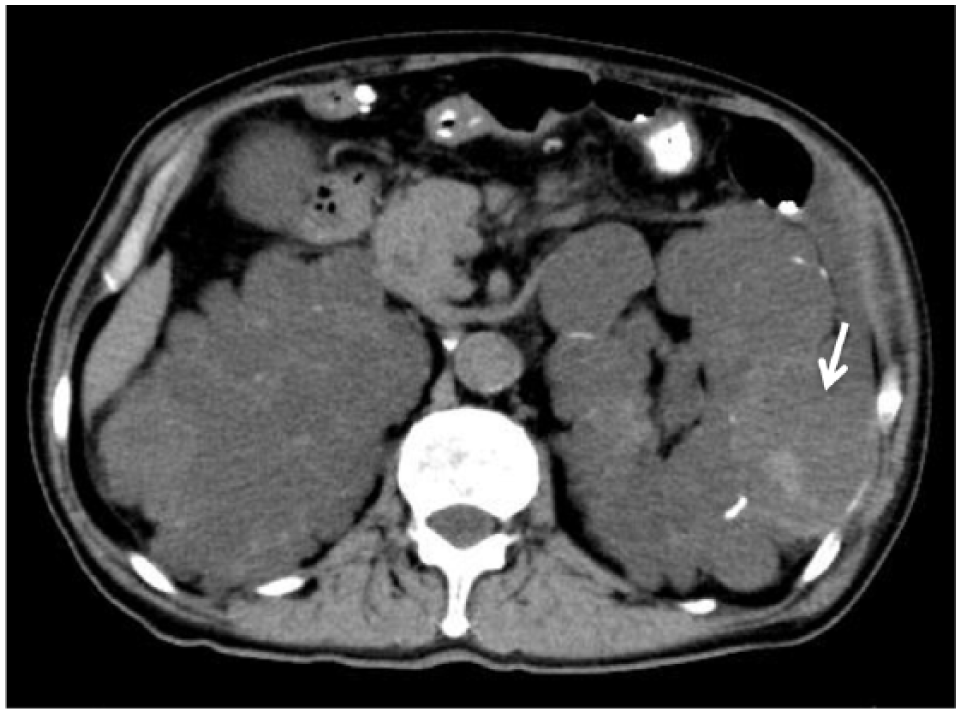
Computed tomography (CT) of affected cyst. Noncontrast CT shows a heterogeneous peripheral cyst with its thick and irregular wall (arrow).

Diffusion-weighted magnetic resonance imaging shows a heterogeneous cyst with hyperintensive signal on diffusion on the lateral surface of the left kidney (arrow).
Judging from his localized symptoms, with no signs of peritoneal irritation, and the CT scan findings, the most likely diagnosis was a cyst infection. We administered intravenous (IV) ceftriaxone (2 g/d) on admission. As the possibility of accompanying prostatitis still remained, we switched to IV levofloxacin (500 mg q48 h) to cover both the cyst infection and prostatitis. On the third day, his symptoms improved and his body temperature was reduced to almost normal range, which was about 36°C. We checked cell counts of peritoneal fluid once every 2 to 4 days for 9 days and found that the cell counts remained consistently low (Table 2). On the fifth day, gram-negative spiral bacteria were detected in the 2 sets of blood cultures, which were found to be H cinaedi on the 10th day. Peritoneal fluid culture also revealed the presence of the same bacteria, although urine culture was negative for it. The subsequent cultures of peritoneal fluid were negative. On the basis of a past report of H cinaedi bacteremia, we switched back to ceftriaxone and continued it for 2 weeks. 12 Subsequently, we switched to oral doxycycline (200 mg/d), and he was discharged. Doxycycline was then continued for 2 weeks, and he fully recovered.
White cell count in dialysis effluent.

Discussion
We report a case of a cyst infection in a patient receiving PD wherein both blood and peritoneal fluid cultures were positive for H cinaedi. This case is unique in that cyst infection spread to the abdominal cavity and to peritoneal fluid in PD patient.
In our patient, PD fluid culture detected H cinaedi, the same bacteria that was present in blood stream. These pathological mechanisms of cyst infection-induced peritonitis or colonization have not been reported thus far. This may be partly because cyst infections do not usually present enough ascites to perform paracentesis, thereby having low chances for collecting peritoneal fluid to diagnose peritonitis. In the present case, we detected the bacteria in the abdominal cavity by collecting PD fluid, which suggested that cyst infections might spread to the abdominal cavity. Another reason for cyst infection-induced colonization of H cinaedi in the present case may be explained by the characteristics of this bacteria, whose infections have higher blood culture positivity than other types of Helicobacter species. 5 In addition, this pathogen is reportedly involved in abdominal aorta aneurysms, atherosclerosis, and atrial arrhythmia,13–15 suggesting that H cinaedi could have more capability to invade blood vessels and even spread to the abdominal cavity than had previously been recognized. 5 In this respect, it is necessary to consider that cyst infection can propagate to peritonitis in ADPKD patients.
In the previous observational report comprised of 73 continuous ambulatory peritoneal dialysis patients, microorganisms recovered from dialysates of patients without peritonitis were identical to organisms recovered from other body sites or indwelling catheters in 9 occasions. The other sites of recovery included blood in 2 cases. 16 Seeding of the peritoneum by organisms originating from other sites may have occurred as observed in our patient. Since kidneys are located in retroperitoneal space, we do not expect a cyst infection to be causing peritonitis through direct bacterial transmission from cyst to peritoneal space. H cinaedi can colonize human skin, and there is a possibility that bacteria were transmitted to abdominal cavity at the time of changing PD fluid. However, we suppose that the possibility of this touch contamination pathogenesis was low because of the very low frequency of bacteremia accompanying PD-related peritonitis. 17 We simply speculate that cyst infection by H cinaedi first occurred and then the bacteria got into blood and transported to abdominal cavity. Intravenous administration of levofloxacin is effective to cyst as well as blood infection. And levofloxacin can also reach abdominal cavity and can be therapeutic option for the treatment of peritonitis as the International Society for Peritoneal Dialysis peritonitis recommendation mentioned. 18 The present case showed appropriate clinical response to fluoroquinolone treatment, which also implied that these three infections were interrelated through the mediation of blood stream infection.
It can be affirmed that the patient did not have PD-related peritonitis because of the lack of the increase in number of peritoneal leukocyte and the lack of the typical abdominal symptom. However, there still remains the possibility that the patients suffer from peritonitis although it was mild. This assumption is based on the evidence that 6% of PD-related peritonitis shows an impaired initial cell reaction.19,20 The reason why peritonitis did not occur despite the existence of H cinaedi is speculated to be from following 2 reasons. First, H cinaedi is a slow-growing bacteria and the abdominal cavity had always been irrigated by receiving PD. Therefore, there was too little time for H cinaedi to grow enough to cause peritonitis. Second, he received oral antibiotics for the insect bite, which may have partially decreased H cinaedi. In this respect, if any cyst infection is incompletely resolved, it will cause peritonitis in the future and such patients are to be followed up carefully.
Conclusion
PD fluid elucidated H cinaedi spread to the abdominal cavity of the ADPKD patient with cyst infection. This is the first report identifying culture-positive peritoneal fluid caused by a cyst infection.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
IY wrote the manuscript and was the treating physician for the patient. NW and KS were treating physicians at the outpatient clinic and helped in drafting the manuscript. HT, KH, MY, MR, HU, SW, and HI helped in drafting the manuscript and revised it critically. All authors have read and approved the final manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report.