
Abstract
Meckel diverticulum is the most common congenital abnormality of the gastrointestinal system. Although most Meckel diverticula are asymptomatic, they can also present with bleeding, obstruction, or perforation. Helicobacter pylori is pathognomonic for the development of a peptic ulcer. We present a case report of a patient with a Meckel diverticulum with Helicobacter pylori colonising its heterotopic gastric mucosa. This is a rare histopathologic finding. We also reviewed the literature of other similar cases published in English.
Introduction
Meckel diverticulum is one of the more common congenital abnormalities of the gastrointestinal system. Although most Meckel diverticula are asymptomatic, they can also present with bleeding, obstruction, or perforation. 1 An ulcer can develop within the heterotopic mucosa that can be present in about 25% of Meckel diverticulum. Helicobacter pylori is pathognomonic for the development of a peptic ulcer. H pylori is a Gram-negative rod that has virulence factors allowing them to survive in the acidic gastric environment. The bacteria can also be found in foci of gastric metaplasia in the duodenum, or gastric-type epithelium in Barrett oesophagus. The presence of H pylori in a heterotopic gastric mucosa in a Meckel diverticulum is rare. We present a case report and review of the English literature of this uncommon histopathologic finding. Informed patient consent to publish this case study was obtained.
Case Report
A 24-year-old man presented to the emergency department of Dandenong Hospital with a 2-day history of lower abdominal pain, worst on his right iliac fossa, and was associated with anorexia, nausea, and vomiting. He did not have any obstructive symptoms, per rectal bleeding, or anaemia. On physical examination, he had a localised peritonism over right iliac fossa. Blood tests showed raised white cell count and C-reactive protein, without any anaemia. Based on the strong clinical suspicion for appendicitis, the patient was taken to theatre for laparoscopic appendicectomy.
At operation, the patient had a nonoedematous looking appendix and lying in the right lower quadrant, a perforated Meckel diverticulum walled-off by small bowel mesentery. Procedure converted to a small infra-umbilical midline laparotomy, where a wedge small bowel resection of the involved small bowel segment and appendicectomy were performed (Figure 1). The patient had an uncomplicated postoperative recovery.

Intraoperative image of a minilaparotomy showing Meckel diverticulum (arrowhead – Meckel diverticulum; arrow – small intestine).
The final histopathology showed inflamed heterotopic acid-secreting-type gastric mucosa within a Meckel diverticulum, with evidence of localised peritonitis (Figure 2). No evidence of malignancy was noted. Immunostains also confirmed the presence of abundant H pylori organisms in an area of inflamed heterotopic gastric mucosa. Appendiceal histology showed mild periappendicitis towards the tip of the appendix.

Histopathologic findings: (A) low-power histopathologic view of the small bowel mucosa (right) and gastric mucosa with acid-secreting glands (left) (H&E). (B) Medium-power histopathologic view of the clusters of parietal cells acid-secreting glands with scattered lymphocytes present between the glands (H&E). (C) Immunohistochemical staining with anti-Helicobacter pylori (SP48) Rabbit Monoclonal Primary Antibody (VENTANA anti-H pylori (SP48)) confirmed diagnosis of H pylori infection. H&E indicates haematoxylin and eosin.
The case was discussed in our multidisciplinary meeting, and the decision was to perform gastroscopy and eradication of H pylori. Follow-up gastroscopy was performed 3 weeks postdischarge, and random biopsies of gastric mucosa did not find any evidence of H pylori colonisation. The patient remained well and asymptomatic at 8 weeks postoperative review.
Discussion
Meckel diverticulum is a fairly common gastrointestinal developmental anomaly, found in 2% of the population. It is usually found 2 feet from the ileocaecal valve, 2 in. in length, with twice the male preponderance. Heterotopic gastric mucosa is present in about half of the cases, with associated bleeding from adjacent small bowel mucosa. However, the presence of H pylori organism in heterotopic gastric mucosa in Meckel diverticulum is a rare histological finding. We performed a literature review using PubMed, MEDLINE and Embase with 2 combined keywords of ‘Meckel diverticulum’ and ‘Helicobacter pylori’ for both adult and paediatric cases. In the last 22 years, we found 12 published reports that specifically looked into the presence of H pylori in a heterotopic gastric mucosa in a Meckel diverticulum (Table 1).
Published reports of Helicobacter pylori in heterotopic gastric mucosa in Meckel diverticulum.
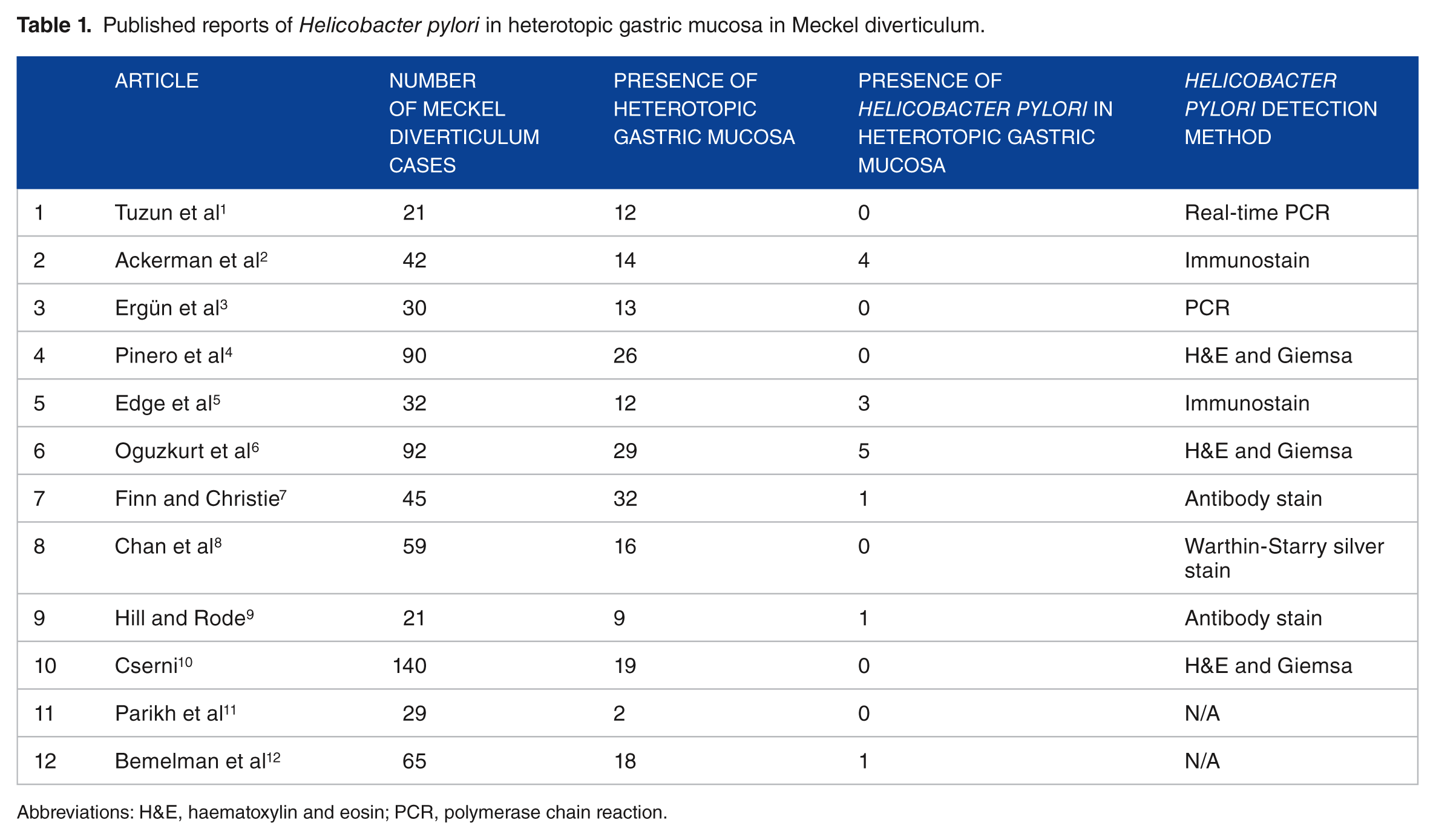
Abbreviations: H&E, haematoxylin and eosin; PCR, polymerase chain reaction.
We found 15 cases (2.25%) of H pylori in heterotopic gastric mucosa out of a total of 666 reported cases of Meckel diverticulum published in the literature. There were 202 cases (30.3%) of heterotopic gastric mucosa found in the series of Meckel diverticulum. The association between the presence of H pylori in heterotopic gastric mucosa and complicated Meckel diverticulum is unclear, unlike the established association of the bacteria with gastric mucosal ulceration. The role of the bacteria in the pathogenesis of the ulceration is hard to prove because the presence of the H pylori bacteria in the heterotopic gastric mucosa itself is quite uncommon. In our case, it is slightly more unusual to find the absence of H pylori in the gastric mucosa on gastroscopy, in the presence of the bacteria in the heterotopic gastric mucosa in Meckel diverticulum.
This case illustrates the rare presence of H pylori in heterotopic gastric mucosa in a complicated Meckel diverticulum – with about 2% found in the case series that we reviewed. One should consider an addition to the rule of 2 when encountered with a Meckel diverticulum.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
TSS and ZH managed the patient; TSS and ZH performed the operation and follow-up; HK provided the histopathological details; TSS collected the data and responsible for the final manuscript.