
Abstract
Herein, we report a rare case of metastatic secondary cardiac myxofibrosarcoma in a 33-year-old female patient. The tumor infiltrated the right lung and was extending into the heart via the right superior pulmonary vein. The patient who initially presented with a stroke was found to be at a high risk of recurrent embolic events and therefore was managed successfully surgically with a complex joint thoracic and cardiac tumor resection. This case illustrates that, in the setting of an extensive metastatic myxofibrosarcoma, an aggressive palliative surgical resection can be successfully performed to improve quality of life.
Introduction
Although primary cardiac tumors are rare, metastasis to the heart is more common than previously appreciated, ranging from 0.7% to 3.5% at autopsy in the general population and in up to 18.3% in patients with known malignancies. 1 Herein, we present a rare case of a metastatic cardiac myxofibrosarcoma in a 33-year-old female patient which was managed successfully by means of surgery.
Case Report
A 33-year-old female patient presented with facial droop and lower body weakness. Brain imaging (computed tomography [CT]) revealed an acute right basal ganglia embolic infarct. The patient’s history was significant for a left thigh myxofibrosarcoma, which had been resected 5 years earlier. One year prior to the current admission, she had developed metastatic disease to her left lateral neck, right upper pulmonary lobe, as well as a right forehead nodule. Following the discovery of these metastases, she underwent doxorubicin chemotherapy and a staged resection for her neck mass. Workup for the patient’s presenting stroke on this admission revealed that the pleural-based mass in the right upper lobe had significantly increased in size, and that this tumor now extended from the right upper lobe into the chest wall via the right superior pulmonary vein into the left atrium, across the mitral valve, and into the left ventricle (Figure 1A and B). CT scan revealed no other metastatic foci. The management of the patient was discussed in multidisciplinary rounds. The main goal of the proposed operation was to prevent sudden death and recurrent cerebrovascular embolic events. This case was presented to a multidisciplinary cardiac tumor team consisting of cardiology, oncology, cardiac surgery, and palliative care, with input from the patient and her family.
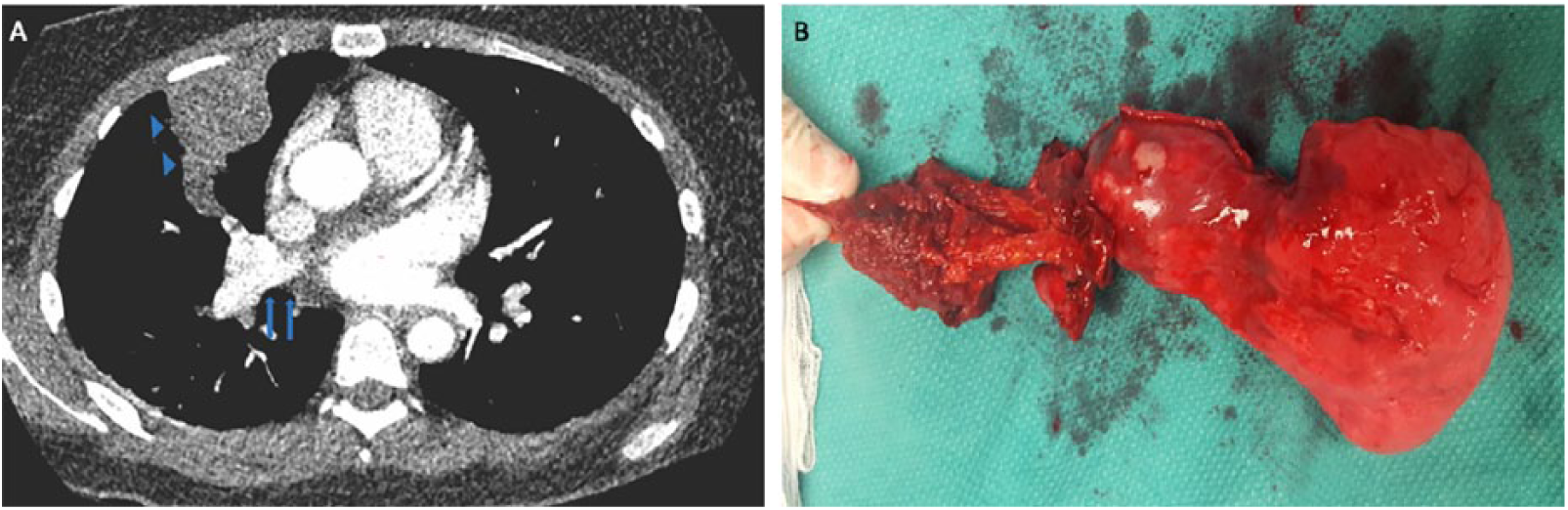
(A) Computed tomography image of the chest (transverse plane) showing the tumor extending from the chest wall and the right upper lobe (blue arrowheads) to the pulmonary vein and the left atrium (blue arrows). (B) Gross image of the excised thoracic component of the tumor (including chest wall, ribs, and pulmonary right upper lobe).
The patient underwent a complex joint thoracic and cardiac tumor resection. After median sternotomy, the chest wall component of the tumor—involving the second and third ribs—was resected. Following initiation of cardiopulmonary bypass and cardioplegic arrest, a left atriotomy was performed, through which a 10-cm myxoid tumor was resected (Figure 2A and B). The orifice of the right superior pulmonary vein from which the tumor entered the left atrium was closed primarily. Subsequently, a right upper lobectomy along with chest wall resection was performed, leaving a large defect, which was reconstructed using a methylmethacrylate mesh. Intraoperative frozen section examination came back showing negative lung and chest wall margins. The patient had an uncomplicated postoperative course and she was asymptomatic at follow-up 6 months after surgery, whereas the post-resection CT thorax remained negative for metastatic disease. Histologic evaluation demonstrated a high-grade myxoid neoplasm with aggressive features and condensation of malignant cells around curvilinear blood vessels consistent with metastatic myxofibrosarcoma.

(A) The cardiac myxoid tumor resected via a left atriotomy (patient’s head is on the left side of the figure). Blue arrow marks the myxoid tumor on the mitral valve. (B) Gross image of the excised cardiac myxoid tumor.
Discussion
Angervall et al 2 were the first to use the term myxofibrosarcoma to describe a lesion of fibroblastic origin with a myxoid matrix. Myxofibrosarcoma—which was formerly known as the myxoid variant of malignant fibrous histiocytoma—is one of the most frequent sarcomas in elderly patients, and usually arises in the extremities, occupying dermal or subcutaneous planes. 3 The primary sites of metastasis for myxofibrosarcomas are pulmonary, bone, and lymph node. 3 The efficacy of radiotherapy and chemotherapy for the treatment of these tumors is not well established. There is a paucity of clinical data regarding the clinical behavior of these tumors. Myxofibrosarcoma is typically associated with better survival than other sarcoma subtypes and also a higher rate of local recurrence. 4
Surgical resection is rarely considered in the setting of metastatic heart tumors as these patients usually present with widespread disease and limited life expectancy. In this case, the multidisciplinary team decided that the patient presented a high risk of recurrent embolic events and/or acute life-threatening hemodynamic obstruction. Therefore, the patient was offered a high-risk palliative surgical resection with the clear understanding that the procedure may not prolong life. During surgery, all sources of potential embolism were removed and a R0 resection was achieved. The patient is still alive 6 months post-surgery and her quality of life is substantially improved as there was no exacerbation of her neurologic symptoms. This case illustrates that, in the setting of an extensive metastatic myxofibrosarcoma, an aggressive surgical approach may be indicated as a palliative strategy to improve quality of life and possibly add some reasonable life extension.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
DK and AM : Writing and literature research; BY: Data analysis and interpretation, approved final manuscript; DL: Final approve of the manuscript.
Informed Consent
The authors confirm that informing written patient consent was obtained for this case study.