
Abstract
We herein report a case with aneurysm rupture in the arc of Bühler (AOB) caused by median arcuate ligament syndrome (MALS). The patient experienced a sudden onset of upper abdominal pain. Contrast-enhanced abdominal computed tomography (CT) showed an iso- to hyper-enhancing area mainly ranging from the dorsal aspect of the pancreatic head to the retroperitoneum around the right kidney. Abdominal angiography revealed marked stenosis in the origin of the celiac artery caused by MALS and a 7-mm saccular aneurysm in the AOB. Thus, we diagnosed the pain as having been caused by aneurysm rupture in the AOB due to MALS. The patient’s symptoms and anemia also improved to normal range without surgery. Careful follow-up, considering possible recurrence of aneurysm at other sites in the future, is essential.
Case Report
A 60-year-old previously healthy woman was brought to our department by ambulance for sudden onset of upper abdominal pain at night. A blood test showed a low serum hemoglobin level of 10.8 g/dL, and contrast-enhanced abdominal computed tomography (CT) revealed an iso- or hyper-enhancing area mainly ranging from the dorsal aspect of the pancreatic head to the retroperitoneum around the right kidney. This site does not have contrast enhancement, and no free air or extravasation was observed inside (Figure 1). Since hemoperitoneum was suspected, abdominal angiography was performed. It was difficult to insert a catheter into the celiac artery; hence, vasoconstriction at the origin of the celiac artery was suspected. Arteriography of the superior mesenteric artery revealed retrograde enhancement of the gastroduodenal and dorsal pancreatic arteries. A 7-mm saccular aneurysm was detected in the arc of Bühler (AOB) (Figure 2). The aneurysm was embolized with a metal coil. The three-dimensional CT on admission marked that stenosis caused by the median arcuate ligament was detected at the origin of the celiac artery (Figure 3). The patient was diagnosed as having a ruptured aneurysm in the AOB caused by median arcuate ligament syndrome (MALS). After surgery, upper abdominal pain resolved without aggravation of the anemia. Esophagogastroduodenoscopy (EGD) was performed, revealing edematous stricture that was presumably caused by compression exerted from the lateral aspect of the duodenum by a hematoma in the descending portion of the duodenum (Figure 4). After 2 weeks, EGD revealed that this stricture had resolved, and the patient was discharged on hospital-day 34.

Contrast-enhanced abdominal computed tomography: ascites is observed on the surface of the liver.
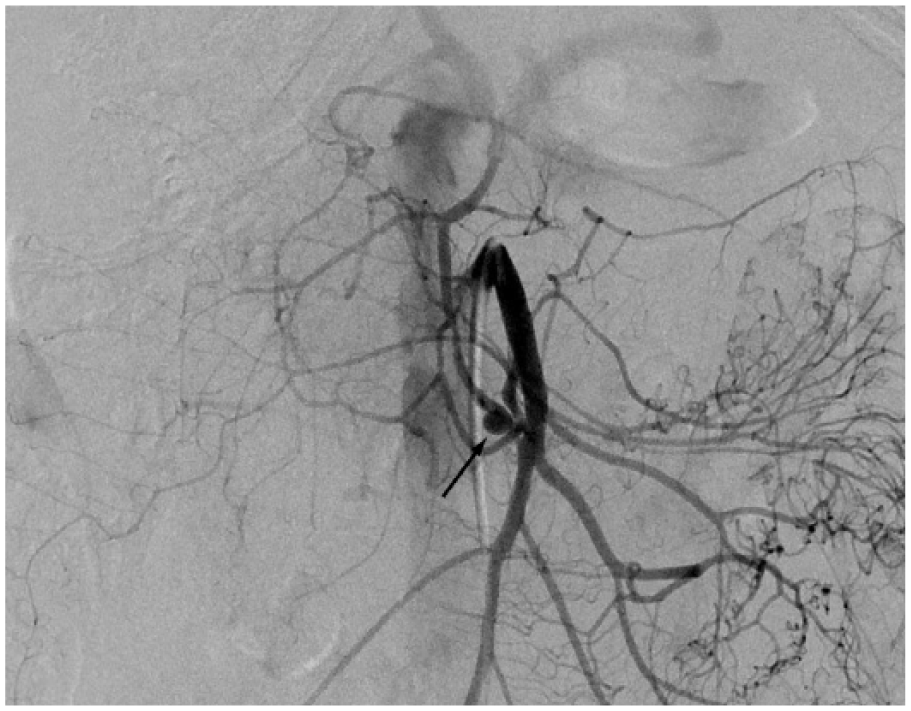
Arteriography of the superior mesenteric artery: a 7-mm saccular aneurysm was detected in the arc of Bühler (arrow).

Contrast-enhanced three-dimensional abdominal computed tomography: the origin of the celiac artery is compressed from the rostral aspect and appears stenotic (arrow).

Esophagogastroduodenoscopy: circumferential and edematous stricture is observed in the descending portion of the duodenum.
The causes of abdominal visceral artery aneurysms include stenosis at the origin of the celiac artery, arteriosclerosis, trauma, infection, pancreatitis, and tumor. 1 In MALS, the median arcuate ligament compresses and constricts the celiac artery. Consequently, the intraluminal pressure differs between the superior mesenteric and celiac arteries, and compensatory blood flow increases in the AOB, which is a direct anastomotic artery between these arteries 2 and in the pancreaticoduodenal artery. This mechanism is considered to induce an increase in arterial blood pressure, which weakens the arterial wall, where an aneurysm develops. 3
Symptoms rarely manifest unless complications occur due to the rupture. 4 Hematemesis or hemorrhagic stool and acute abdomen may develop if the rupture occurs in the gastrointestinal tract and in the abdominal cavity, respectively. If the rupture occurs into the retroperitoneal space, the affected individual usually has no symptoms other than anemia. 5 In addition, a statistically significant correlation was found between the range of carotid artery (CA) stenosis and the presence of collateral circulation. Furthermore, ischemia as a result of mesenteric vessel narrowing by the median arcuate ligament may occur more often than indicated by clinical symptoms and described in literature. 6 This patient developed acute abdomen and anemia, and abdominal CT revealed hematoma in the abdominal cavity and retroperitoneal space. Thus, we needed to consider this symdrome in the differential diagnosis. Computed tomography angiography (CTA), magnetic resonance angiography (MRA), Doppler ultrasound (US), and intravascular ultrasound (IVUS) are useful as diagnostic methods.7,8 Regarding treatment, with advances in intervention radiology (IVR), non-invasive transcatheter procedures have been established as safe and effective therapeutic strategies. 9 Previous reports have raised the possibility that the development of new aneurysms is low after administration of only IVR as treatment for focal aneurysms without resection of the arcuate ligament. 10 However, careful follow-up still appears to be necessary in consideration of the possible recurrence of aneurysms at other sites.
In conclusion, although such cases are rare, if a patient complains of acute upper abdominal pain and imaging shows retroperitoneal hematoma or hemoperitoneum, we should suspect this syndrome and confirm the existence of an aneurysm with angiography.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
KA and KT wrote the manuscript. MI and YM provided the images. KT, SM, NI, and AI reviewed the manuscript. KT is the article guarantor.
Informed Consent
Informed consent was obtained for this case report.