
Abstract
Uncontrolled diabetes and acute coronary syndrome share a complex dynamic that results in significant ambiguity when interpreting biomarker elevations in this setting. This is concerning because myocardial infarction has been shown to be the most common cause of death in the first 24 hours of admission for uncontrolled diabetes. Literature shows that elevation in cardiac biomarkers in patients with uncontrolled diabetes could be from viral myopericarditis, although a clear clinical significance is still lacking.1 It is, however, clear that elevation in cardiac biomarkers portends a poor long-term prognosis in patients with uncontrolled diabetes mellitus. We present a rare case of myopericarditis in a middle-aged patient with uncontrolled diabetes. The patient had elevated troponin I level reaching a peak of 7.3 ng/mL with associated ST elevations on electrocardiography. Coronary angiogram was subsequently done revealing clean coronaries. To our knowledge, this is the first description of myopericarditis in uncontrolled diabetes without a known cause.
Introduction
Elevated cardiac biomarkers in uncontrolled diabetes in the absence of an acute coronary syndrome have been described in several case reports. Acute uncontrolled diabetes and acute coronary syndrome (ACS) share a complex dynamic that results in significant ambiguity when interpreting biomarker elevations in this setting. This is concerning because myocardial infarction has been shown to be the most common cause of death in the first 24 hours of admission for acute uncontrolled diabetes.
Ketoacidemia may contribute to elevations in cardiac enzymes. Clinical significance of cardiac biomarkers elevation in uncontrolled diabetes is still not clear. The literature suggests that elevations in cardiac biomarkers portend a poor long-term prognosis in patients with uncontrolled diabetes mellitus. We present a rare case of myopericarditis in uncontrolled diabetes in a middle-aged patient. To our knowledge, this is the first description of myopericarditis in uncontrolled diabetes.
Clinical Vignette
A middle-aged patient presented to the emergency department with complaints of persistent nausea and vomiting of 1-day duration. Medical history was significant for insulin-dependent diabetes mellitus and noncompliance with home regimen of 25U Lantus subcutaneous at night and 7U of NovoLog before every meal. Physical examination revealed blood pressure—149/79, pulse—88, temperature—36.7, and respiratory rate—26. Patient appeared clinically dehydrated. Cardiorespiratory system was unremarkable. Abdominal examination revealed nothing of significance. Patient was alert and oriented ×3. Neurological examination was within normal limits. Initial labs showed β-hydroxybutyrate level of 8.65 mmol/L, blood glucose level 565 mg/dL, pH 6.99, HCO3 <5 mEq/L, lactic acid of 6 mg/dL, blood urea nitrogen/serum creatinine 17/1.4 mg/dL, anion gap 36 mEq/L, serum potassium level 5.8 mEq/L, and troponin level 0.012 ng/mL. Electrocardiography (ECG) showed normal sinus rhythm. Patient was admitted to the medical intensive care unit for diabetic ketoacidosis (DKA) and treated with intravenous fluid, intravenous insulin, and K replacement per institution protocol, and DKA was resolved within 24 hours of admission. By day 2, the patient complained of pleuritic chest pain, relieved by sitting up and leaning forward. Serum troponin I level started trending upward reaching a peak of 7.3 ng/mL. ST elevations were also noted on ECG. Computed tomographic angiogram of chest ruled out pulmonary embolism and pneumomediastinum. Echocardiogram was normal. Coronary angiogram revealed nonobstructive coronary vessels (Figures 1 to 3). A diagnosis of myopericarditis was made. Patient was treated with aspirin and colchicine with resolution of chest pain. Troponin levels started trending downward on day 3. Patient was discharged home on day 4 with close clinic follow-up.
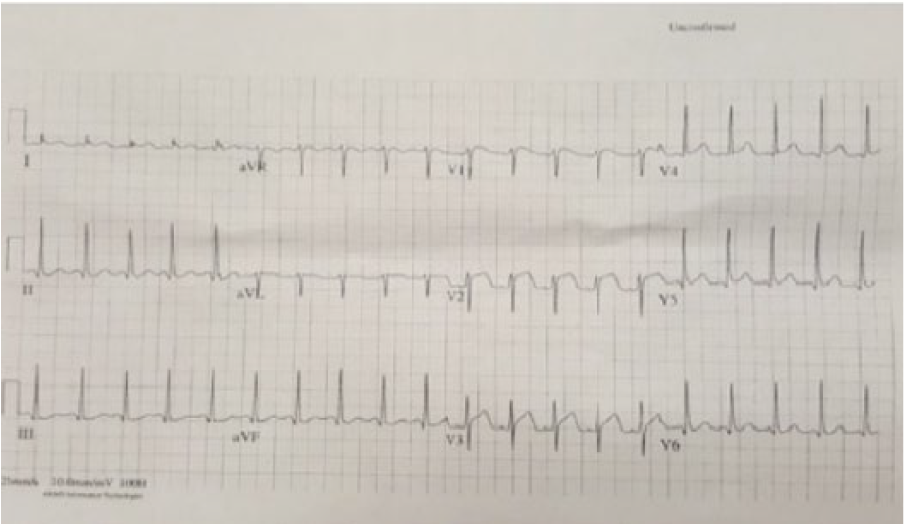
Electrocardiography during active chest pain. Diffuse ST elevations seen in V1-V3.

Electrocardiography at the time of discharge. ST elevations previously seen in V1-V3 are not observed.

Coronary angiogram from patient showing nonobstructive coronary vessels.
Discussion
Cardiac biomarker elevation in uncontrolled diabetes is difficult to explain in the absence of ACS. The incidence of troponin elevation in this setting may be as high as 34% and is associated with later major adverse cardiac outcomes. One paper reports serum pH of less than 7.0 as an independent prognostic factor for elevations in serum troponin without angiographic evidence of coronary artery disease. 2 Myocarditis in uncontrolled diabetes has been described in the literature; however, in all the cases, a described viral cause was responsible for the clinical findings. Campbell et al 1 described pericarditis in DKA with no apparent cause and suggested that dehydration may be responsible leading to subepicardial injury.
Diabetic ketoacidosis does cause acute myocardial necrosis, although the mechanism remains unclear. 3 Several theories include severe acid-base and electrolyte abnormalities, as well as dehydration triggering coronary artery spasms and low cardiac output, increased blood viscosity, increased platelet aggregation, impaired blood flow, increased red blood cell rigidity, and hemostatic changes all enhance the development of thrombosis. 4
The transient ECG abnormalities in DKA include ST depression, prolongation of the QT interval, abnormalities of the T wave, and prominent U waves. These changes, although not well-understood, are believed to be related to metabolic disturbances and hyperkalemia present in DKA. ST segment elevation is not a recognized ECG abnormality in ketoacidosis. Our patient had evidence of new ST elevation on ECG with associated elevations in cardiac biomarkers. Coronary angiogram showed no evidence of coronary artery disease resulting in a provisional diagnosis of myopericarditis. These findings could be explained by the metabolic disturbances observed in this patient. Further investigation into myocardial muscle involvement needs to be considered by Cardiac magnetic resonance imaging and or biopsy if indicated. Our patient had no echocardiographic evidence of reduction in ejection fraction and hence did not have further imaging. The prognostic importance of elevated troponin in DKA as a marker for worse cardiac outcomes may soon warrant further evaluation of myocardial muscle involvement in DKA. 5
Conclusions
To the best of our knowledge, this is the first time myopericarditis has been observed with no clear cause in the setting of uncontrolled diabetes. Similar to the observation of elevated cardiac biomarkers without ACS in DKA, the clinical significance remains to be interpreted. Current literature forecasts poor later outcomes in this patient population. Further studies will be required to elucidate the exact significance of elevated biomarkers in uncontrolled diabetes. Clear guidelines for management of these patients are still lacking.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MZ, AO, RK: Management and diagnosis of the patient. AO, RK, AA, BJ, RA: Research, writing and proof reading of the case report.