
Abstract
Of 129 esophagectomies at our institute from June 2010 to March 2015, we experienced three preoperative positron emission tomography-computed tomographic (PET/CT) false positives. Bone metastasis was originally suspected in 2 cases, but they were later found to be bone metastasis negative after a preoperative bone biopsy and clinical course observation. The other cases suspected of mediastinal lymph node metastasis were diagnosed as inflammatory lymphadenopathy by a pathological examination of the removed lymph nodes. Conducting a PET/CT is useful when diagnosing esophageal cancer metastasis, but we need to be aware of the possibility of false positives. Therapeutic decisions should be made based on appropriate and accurate diagnoses, with pathological diagnosis actively introduced if necessary.
Background
Positron emission tomography-computed tomography is useful for diagnosing primary and metastatic lesions of esophageal cancer. The sensitivity and specificity of a PET/CT are also relatively preferable to other diagnostic imaging tools. 1 Although the number of cases is few, false positives exist in which an inflammatory tumor mass and a nonspecific tumor mass are difficult to differentiate between, even when combined with other image findings. In cases of esophageal cancer, the types of treatment and their prognosis are greatly affected if there is a metastasis or recurrence. Positron emission tomography-computed tomographic false positives cannot simply be ignored even if they appear to be due to inflammation or some other factors. This case report discusses the reasons to conduct a PET/CT test and its limitations in diagnosing esophageal cancer.
Methods
The subjects of this investigation had suspected metastasis from a PET/CT which occurred before surgery of the 129 resected cases of esophageal cancer at our department from June 2010 to March 2015. However, after surgery, biopsy and/or follow-up observation, only the cases that were confirmed as metastasis negative were considered to be PET/CT false positives for this assessment.
Results
There were 3 cases of preoperative PET/CT false positives (Table 1). Two cases in which bone metastasis was suspected revealed almost normal range of squamous cell carcinoma (SCC)−associated antigen, alkaline phosphatase, and serum calcium levels. The other case was suspected of right upper mediastinal lymph node metastasis.
Cases of esophageal cancer metastasis preoperative positron emission tomography-computed tomographic false positives.

Abbreviations: LN, lymph node; M, metastasis; Mt, middle thoracic lesion of esophagus; N, node; T, tumor; Ut, upper thoracic lesion of esophagus.
In case 1, a 59-year-old man, without particular medical history, had a diagnosis of esophageal carcinoma by endoscopy. Multiple bone metastases were suspected by a PET/CT in the spine, sternum, ribs, and pelvic bone (Figure 1). After conducting a CT-guided biopsy of the right iliac bone, the patient was determined to be metastasis negative. A radical esophagectomy via a right thoracotomy, reconstructed with gastric tube was performed. Pathological diagnosis was carcinosarcoma invading to a submucosal layer, without lymph node metastasis. One course of adjuvant chemotherapy (5-fluorouracil and cisplatin) was performed. The patient is alive with no recurrence 4 years and 10 months after surgery, although the false-positive lesions in pelvic bone are still detected by PET/CT.

In the case 1, multiple bone metastases were suspected by a positron emission tomography-computed tomography in the pelvic bone (SUVmax = 2.94).
In case 2, a 71 year-old man, without particular medical history, was diagnosed with hypopharynx cancer and esophageal cancer. Abnormal accumulations of fluorodeoxyglucose (FDG) in the manubrium sterni, vertebra Th5, and the pedicle of vertebral arch were found by PET/CT. The lesions were suspected to be multiple bone metastases. Bone metastasis was not confirmed by other clinical findings. Therefore, after the sufficient informed consent, the patient underwent a laryngopharyngeal esophagectomy, a transhiatal esophagectomy without thoracotomy, and reconstruction with the gastric tube through the posterior mediastinal route. Pathological finding showed poorly differentiated SCC of esophagus and moderately differentiated SCC of hypopharynx with a cervical lymph node metastasis. The patient is alive with no recurrence 3 years and 11 months after the surgery.
In case 3, a 76-year-old man, without particular medical history, had a diagnosis of a superficial esophageal cancer by endoscopy. He was suspected of lymph node metastasis of right recurrent nerve lymph node (Figure 2) by preoperative PET/CT. The lymph node was diagnosed as inflammatory lymphadenopathy by a pathological examination. Scattered silicotic nodules and inflammatory lymphadenopathy might be caused by pneumoconiosis (Figure 3).
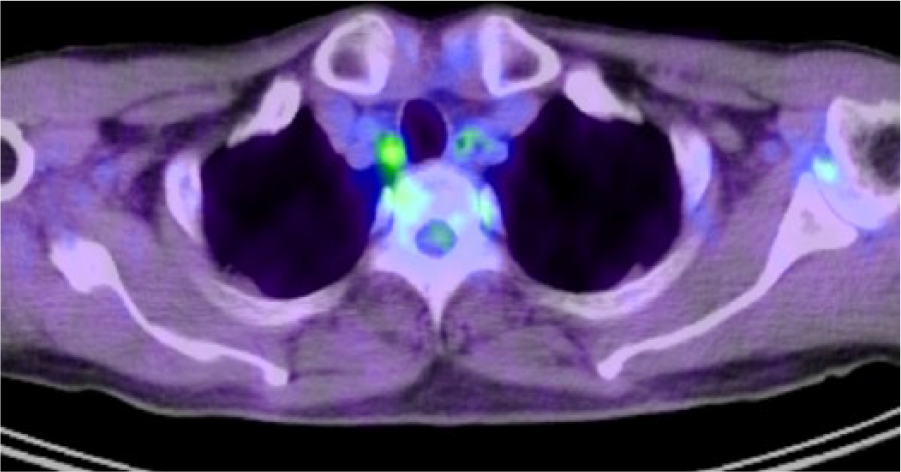
Case 3 was suspected of right recurrent nerve lymph node metastasis by preoperative positron emission tomography-computed tomography (SUVmax = 3.00).
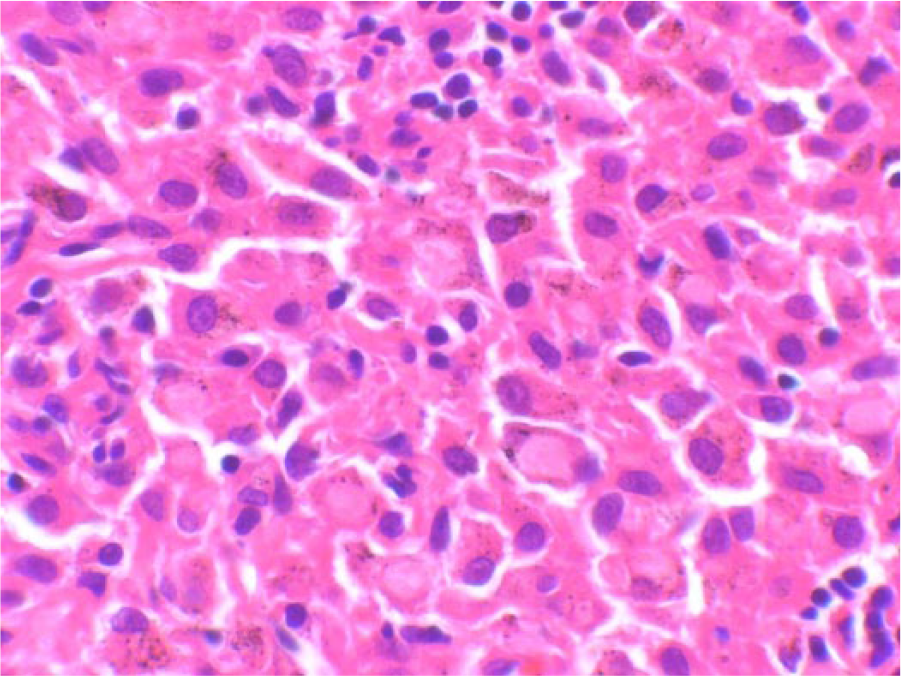
Pathological finding of case 3 revealed scattered silicotic nodules in resected lymph nodes with infiltration of histiocytosis to sinusoid.
Discussion
In esophageal cancer treatment, FDG-PET/CT is also used to diagnose metastases and to judge the effectiveness of treatment. Especially, pretherapeutic staging is extremely important when choosing the treatment for a progressing esophageal cancer. There are cases when the surgery may not apply to a patient if remote metastasis or high-grade lymph node metastasis is found. Many cases have already been reported claiming that FDG-PET is a useful modality for a pretherapeutic staging. 1
Esophageal cancer causes 30% to 40% of lymph node metastases among cancers that spread to the submucosa, and the prognosis of esophageal cancer is known to be defined by the presence of lymph node metastasis, how many metastases are present, and how much the metastasis spreads. Therefore, evaluating lymph node metastasis is a very important factor in deciding the course of treatment. The diagnosability of lymph node metastasis using a FDG-PET for esophageal cancer is generally reported to have a sensitivity of 32% to 51.9%, a specificity of 94.2% to 100%, and an accuracy of 48% to 93%. 2 This is considered to be more accurate than CT by itself. In addition, FDG-PET/CT, which is a combination of a FDG-PET and a CT, improves the diagnosability even more. Yuan et al 3 have reported that they evaluated the diagnosability of lymph node metastasis using FDG-PET/CT for esophageal squamous cancer and found a sensitivity of 94%, a specificity of 92%, and an accuracy of 92%.
However, the size of a lymph node that can be detected by PET/CT is said to be only 6 to 8 mm,1,2 thus it is difficult to detect micrometastasis. Also, detecting metastasis to neighboring lymph nodes could be difficult in cases with a lot of FDG accumulation in the primary lesion, or accumulation in the intestinal tract such as in the stomach, or in the heart. The FDG accumulates in inflamed lymph nodes as well, so false positives often appear in hilar lymph nodes or in patients who have chronic lung disease. 4 Lymph node metastasis was suspected after a preoperative PET/CT for the case 3, as described above, but it was actually an inflammatory lymphadenopathy caused by pneumoconiosis. Dual-time-point FDG-PET has been reported to be useful in reducing this kind of false positive. 5 It uses the time differences of peak FDG accumulation for inflammation versus for tumors. After injecting the FDG, 2 measurements are taken at intervals.
In earlier studies, PET has revealed occult distant metastases at nodal and non-nodal sites in 5% to 40% of patients. 6 Distant metastases of esophageal squamous cancer are mainly found in the lungs, liver, and bones. Bone metastases were found in 2% to 6% of all cases. 7 Kato et al reported the diagnosability of FDG-PET for esophageal cancer as having a sensitivity of 92%, a specificity of 94%, and an accuracy of 93%. When comparing those numbers to bone scintigraphy, whose diagnosabilities are 77%, 84%, and 82%, respectively, the diagnosability of FDG-PET is superior, especially for osteolytic lesions. But 2 false positives out of 44 cases came from PET, showing that FDG-PET is not perfect. 8
The SUVmax of metastic tumor might be helpful to increase the accuracy of PET/CT. Our previous study demonstrated that The SUVmax of the primary tumor was positively correlated with tumor size and vessel invasion and was positively related to the SUVmax of metastic tumor. 9 In the report, the diagnostic accuracy of PET/CT (87.3%) was higher than that of conventional CT scans. 9
When diagnosing metastatic bone tumors, the positive predictive value of bone metastasis is known to be quite high if the findings for both PET and CT match. 10 Therefore, even when bone metastasis is suspected due to abnormal FDG accumulation after a FDG-PET, yet no bone destruction image is found in the same site by CT, then interventional radiology or a surgical biopsy should be conducted to obtain a pathological diagnosis. Obtaining an accurate disease staging diagnosis is necessary to decide on an appropriate treatment.
Conclusions
This case report was on 3 patients with suspected metastasis due to a false-positive PET/CT who were later confirmed to not have metastasis. The metastases were originally suspected after conducting a PET/CT before surgery to treat esophageal cancer or during the postoperative course. Conducting a PET/CT is useful when diagnosing esophageal cancer metastasis, but there should be an awareness of the possibility of false positives. Therapeutic decisions should be made based on appropriate and accurate diagnoses, and a pathological diagnosis should be actively introduced if necessary.
Footnotes
Peer review:
Three peer reviewers contributed to the peer review report. Reviewers’ reports totaled 332 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TY designed the study, NI, MT, JH and YN contributed to analysis and interpretation of data, and assisted in the preparation of the manuscript. KS wrote the initial draft of the manuscript. KY, AU, and MH have contributed to data collection and interpretation, and critically reviewed the manuscript. The final version of the manuscript was approved by all authors.
Ethical Statement
This case report was in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent or substitute for it was obtained from all patients for being included in the study.